A Case of Fibular Aplasia-Tibial Campomelia-Oligosyndactyly (FATCO) Syndrome Associated With Split Hand/Foot Syndrome With Long Bone Deficiency (SHFLD) and Review of the Literature
Theodora- Eleftheria Deftereou, Vaya R Karapepera, Christina Angelika Alexiadi, Stylianos Tologkos, Vasiliki Papadatou, Georgios Alexiadis, Dimitrios Karamanidis, Lambropoulou Maria

TL;DR
This paper reports a rare case of a fetus with combined limb defects and reviews similar cases in medical literature.
Contribution
The novelty lies in reporting a rare combination of SHFLD and FATCO syndromes in a Greek fetus.
Findings
A male fetus was found to have SHFLD combined with FATCO syndrome.
This is the first reported case of FATCO syndrome in Greece.
The paper reviews existing literature on these rare limb defects.
Abstract
Split hand/foot malformation is a heterogeneous congenital disorder mainly presented with a median cleft of hands or/and feet. It can be associated with long bone aplasia, a syndrome also known as split hand/foot syndrome with long bone deficiency (SHFLD), which is a very rare condition. We report a very rare case of a male fetus with SHFLD syndrome combined with fibular aplasia, tibial campomelia, and oligosyndactyly (FATCO) syndrome. FATCO syndrome is also an extremely infrequent congenital limb defect by itself. Based on our review of the literature, there appears to be no other FATCO case reported in Greece.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2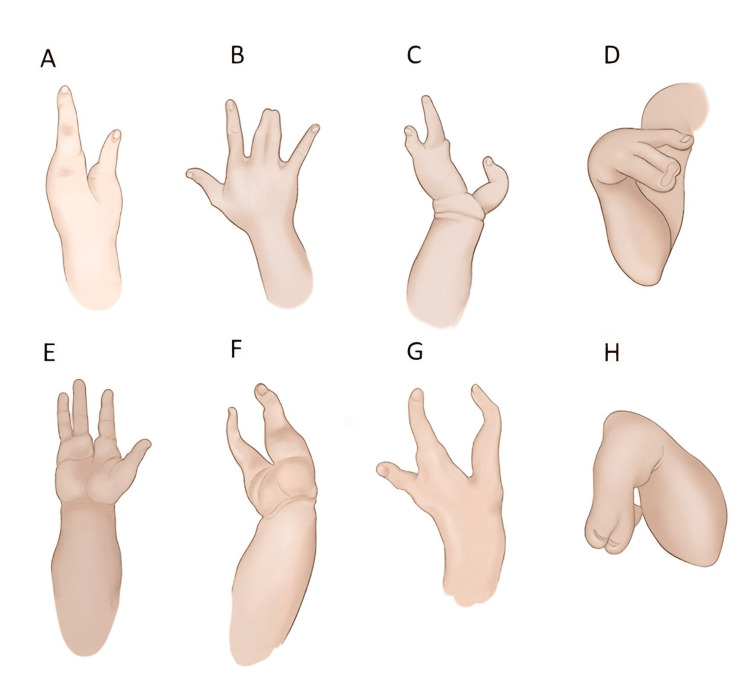 Figure 3
Figure 3| S. No. | References | Sex | Upper extremities | Lower extremities | Other malformations | Family history |
| 1 | Hecht and Scott (1981) [ | Male | Bilateral hands absence | Left fibular aplasia, Left tibia aplasia, Bilateral foot absence | Cardiomegaly | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
| 2 | Hecht and Scott (1981) [ | Female | Right hand absent, Left hand oligosyndactyly | Left fibular aplasia, Bilateral tibia shortening and campomelia, Right tibia with soft tissue dimpling, Bilateral foot oligosyndactyly | None | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
| 3 | Huber et al. (2003), Case 1 [ | Male | Bilateral postaxial polydactyly | Bilateral fibular aplasia, Left tibia shortening, campomelia with skin dimpling, Bilateral oligodactyly, Bilateral clubfeet, Bilateral tarsal aplasia | Dislocation of hip | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
| 4 | Huber et al. (2003), Case 2 [ | Male | Right hand oligodactyly | Bilateral fibular aplasia, Bilateral tibia campomelia with skin dimpling, Bilateral oligodactyly | Retrognathia, Ear lobule crease | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
| 5 | Cuillier et al. (2004) [ | Not mentioned | Normal | Right fibula aplasia, Right tibia hypoplasia, Right foot oligodactyly, Right club-foot | None | Not mentioned affinity in couple, not mentioned family history of skeletal disorders |
| 6 | Courtens et al. (2005) [ | Male | Left hand syndactyly | Right fibula aplasia, Right tibia shortening and campomelia with soft tissue dimpling, Right foot oligodactyly, Left foot dysmorphia | Mild micrognathia | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
| 7 | Monteagudo and Timor-Tritsch (2006) [ | Female | Normal | Right fibula aplasia, Right tibia campomelia, Right foot oligosyndactyly, Right club-foot | None | Not mentioned affinity in couple, not mentioned family history of skeletal disorders |
| 8 | Kitaoka et al. (2009) [ | Male | Right hand oligosyndactyly | Right fibula hypoplasia, Left fibula aplasia, Left tibia shortening with campomelia and soft tissue dimpling, Bilateral foot oligodactyly | Left cleft lip and cleft palate | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
| 9 | Karaman and Kahveci (2010)[ | Male | Normal | Left fibula aplasia, Left tibia shortening with campomelia and soft tissue dimpling, Left oligosyndactyly | Not mentioned | Not mentioned affinity in couple, not mentioned family history of skeletal disorders |
| 10 | Vyskocil et al. (2011) [ | Male | Normal | Left fibula aplasia, Left tibia shortening campomelia and skin dimpling, Left foot oligodactyly and calcaneous nucleous hypoplasia | None | Not mentioned affinity in couple, no family history of congenital disorders |
| 11 | Ekbote and Danda (2012) [ | Male | Normal | Left fibula aplasia, Left tibia campomelia and soft tissue dimpling, Left oligosyndactyly | Klinefelter syndrome, Micropenis | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
| 12 | Bieganski et al.(2012), Case 1 [ | Female | Bilateral oligosyndactyly | Bilateral fibular aplasia, Bilateral tibia camptomelia with skin dimpling, Bilateral oligodactyly, Bilateral tarso-calcaneal coalition and hypoplastic central ray, Bilateral equinous hindfoot, Bilateral tarsal coalition | Isolated membranous ventricular septal defect closed spontaneously | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
| 13 | Bieganski et al. (2012), Case 2 [ | Male | Bilateral oligosyndactyly, Bilateral U-shaped hand, | Right fibular aplasia, Left fibular hypoplasia, Bilateral tibia campomelia with skin dimpling, Bilateral oligodactyly, Right plano-valgus foot, Left foot with talipes equinovarus | None | Non-consanguineous couple, family history unremarkable. Mother with bilateral partial skin foot syndactyly |
| 14 | Bieganski et al. (2012), Case 3 [ | Male | Normal | Bilateral fibular aplasia, Bilateral tibia shortening and campomelia with skin dimpling, Bilateral oligosyndactyly | Not mentioned | Non-consanguineous couple, family history unremarkable |
| 15 | Sezer et al. (2014) [ | Male | Right hand oligodactyly, Left hand oligosyndactyly | Bilateral fibular aplasia, Bilateral tibia shortening with camptomelia and skin dimpling, Bilateral oligosyndactyly, Bilateral club foot | None | Non-consanguineous couple, family history unremarkable |
| 16 | Goyal et al. (2014) [ | Male | Normal | Right fibula hypoplasia, Right tibia campomelia with skin dimpling, Right foot oligosyndactyly, Right talus hypoplasia | Not mentioned | Non-consanguineous couple, family history unremarkable |
| 17 | Bastaki et al. (2014) [ | Male | Normal | Bilateral fibular aplasia, Bilateral tibia camptomelia with skin dimpling, Bilateral oligosyndactyly, | None | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
| 18 | Smets et al. (2016) [ | Female | Normal | Left fibular hypoplasia, Left tibia shortening with campomelia and soft tissue dimpling, Bilateral oligosyndactyly | None | Not mentioned affinity in couple, no relevant family history |
| 19 | D’Amato Gutiérrez and Palacio Díaz (2016) [ | Male | Normal | Right fibular aplasia, Right tibia shortening and campomelia, Right foot oligodactyly | None | Not mentioned affinity in couple, not mentioned family history of skeletal disorders |
| 20 | Hazan et al. (2016) [ | Male | Normal | Bilateral fibular aplasia, Bilateral camptomelia, Bilateral oligosyndactyly | None | Not mentioned affinity in couple, not mentioned family history of skeletal disorders |
| 21 | Nogueira et al. (2016), Case 1 [ | Male | Ulnar deviation of the hands | Right fibular aplasia, Right tibia shortening and campomelia, Bilateral oligosyndactyly, Bilateral Rocker-Bottom foot | Intra-orbital grooves, Micrognathia, Bifurcated cardiac apex due to the left ventricle | Non-consanguineous couple, no family history of skeletal dysplasia |
| 22 | Nogueira et al. (2016), Case 2 [ | Male | Normal | Left fibular aplasia, Left tibia campomelia with soft tissue dimpling, Bilateral oligosyndactyly, Bilateral clubfoot | Big phallus | Not mentioned affinity in couple, no family history of skeletal dysplasia |
| 23 | Nogueira et al. (2016), Case 3 [ | Female | Normal | Right fibular aplasia, Right tibia campomelia with soft tissue dimpling, Bilateral oligosyndactyly | Micrognathia, Esophageal atresia with tracheal fistula | Not mentioned affinity in couple, no family history of skeletal dysplasia |
| 24 | Nogueira et al. (2016), Case 4 [ | Male | Arachnodactyly | Left fibular aplasia, Left tibia campomelia, Left foot oligosyndactyly, Left tarsal bones hypoplasia | None | Non-consanguineous couple, no family history of skeletal dysplasia |
| 25 | Abdalla and El- Beheiry (2017) [ | Female | Normal | Bilateral fibular aplasia, Bilateral tibia camptomelia with skin dimpling, Bilateral femoral angulation, Right foot oligodactyly, Left foot oligosyndactyly, Left foot aplasia of calcaneus, talus and cuboid bones, Left split- foot malformation | None | Non-consanguineous couple, no family history of congenital disorders |
| 26 | Amhad et al. (2017) [ | Male | Not mentioned | Right fibular aplasia, Right tibia campomelia, Right foot oligodactyly, Right talus aplasia | None | Non-consanguineous couple, no family history of congenital disorders |
| 27 | Petricevic et al. (2017) [ | Male | Right hand syndactyly | Bilateral fibular aplasia, Bilateral tibia camptomelia with soft tissue dimpling, Bilateral oligosyndactyly | None | Not mentioned affinity in couple, not mentioned family history of skeletal disorders |
| 28 | Önder Yılmaz et al. (2018) [ | Female | Right hand with hypoplasia of fourth metatarsal bone, Left hand with duplication of fourth finger’s distal phalanx | Left fibular aplasia, Left tibia campomelia, Left foot oligodactyly, Right foot with duplication of the third metatarsus | None | Non-consanguineous couple, no family history of congenital or skeletal disorders |
| 29 | Guevara Zárate et al. (2018) [ | Male | Not mentioned | Left fibular aplasia, Left tibia shortening and campomelia, Left foot oligodactyly | Not mentioned | Not mentioned affinity in couple, not mentioned family history of skeletal disorders |
| 30 | Isik et al (2019)[ | Female | Left hand oligosyndactyly | Right fibular aplasia, Right tibia campomelia, Right foot oligodactyly | Ventricular dilatation and hydrocephaly | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
| 31 | Marinho et al. (2020), Case 1 [ | Male | Normal | Right fibular aplasia, Right tibia shortening and campomelia. Bilateral feet oligosyndactyly, Right clubfoot | Micrognathia | Not mentioned affinity in couple, no family history of skeletal disorders |
| 32 | Marinho et al (2020), Case 2 [ | Female | Normal | Right fibular aplasia, Right tibia campomelia with soft tissue dimpling, Right femur shortening, Bilateral oligosyndactyly | Micrognathia, Esophageal atresia with tracheal fistula | Not mentioned affinity in couple, no family history of skeletal disorders |
| 33 | Izadi and Salehnia (2020) [ | Female | Normal | Right fibular aplasia, Right tibia shortening, Right foot oligosyndactyly, Right talus aplasia, Right calcaneus hypoplasia, Right split foot malformation | None | Consanguineous couple, no family history of congenital or skeletal disorders |
| 34 | Igoche and Umaru (2020) [ | Female | Not mentioned | Left fibular aplasia, Left tibia shortening and campomelia, Left foot oligodactyly | Ventricular septal defect | Not mentioned affinity in couple, not mentioned family history of skeletal disorders |
| 35 | Kavipurapu et al. (2021), Case 1 [ | Male | Left hand oligodactyly, Right hand syndactyly | Left fibular aplasia, Left tibia campomelia with skin dimpling | Spina bifida occulta | Consanguineous couple, family history was unremarkable |
| 36 | Kavipurapu et al. (2021), Case 2 [ | Male | Normal | Right fibular aplasia, Right tibia campomelia with skin dimpling, Right femoral shortening and dysplasia, Right foot oligosyndactyly, Left foot oligodactyly, Right equino-valgus foot | Not mentioned | Non-consanguineous parents, family history was unremarkable |
| 37 | Mishra and Verma (2021) [ | Male | Normal | Left fibula hypoplasia, Left tibia hypoplasia, Left foot oligosyndactyly, Left talus aplasia | None | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
| 38 | Yucel Celik et al. (2021) [ | Male | Bilateral oligodactyly | Right fibular aplasia, Right tibia campomelia, Right foot oligodactyly, Bilateral clubfoot | Hyperechogenic bowel | Consanguineous couple, no family history of congenital or skeletal disorders |
| 39 | Matalon et al. (2022), Case 1 [ | Male | Right hand symbrachydactyly | Bilateral fibular aplasia, Left foot syndactyly | None | Unknown |
| 40 | Matalon et al. (2022), Case 2 [ | Female | Left hand symbrachydactyly | Bilateral fibular aplasia, Bilateral tibia shortening, Bilateral split foot malformation | None | Unknown |
| 41 | Matalon et al. (2022), Case 3 [ | Male | Right hand oligosyndactyly, Left hand syndactyly | Right fibular aplasia, Right tibia shortening and slight campomelia, Bilateral oligosyndactyly | None | Not mentioned affinity in couple, not mentioned family history of skeletal disorders |
| 42 | Georgeos and Elgzzar (2022) [ | Male | Right hand oligodactyly | Right fibula hemimelia, Right tibia campomelia with skin dimpling, Right foot oligosyndactyly (split foot malformation) | Brachycephaly | Consanguineous couple with strong history of genetic diseases and congenital anomalies |
| 43 | Benli et al. (2022)[ | Female | Normal | Left fibular aplasia, Left tibia campomelia, Left foot oligodactyly | None | Non-consanguineous parents, not mentioned family history of congenital or skeletal disorders |
| 44 | Hashmi et al. (2022) [ | Male | Normal | Right fibular rudimentary, Right tibia shortening and campomelia, Right foot oligodactyly | None | Consanguineous couple, no family history of limb abnormalities |
| 45 | Georgesku et al. (2022) [ | Not mentioned | Normal | Right fibular aplasia, Right tibia shortening and campomelia, Right foot oligodactyly | None | Not mentioned affinity in couple, not mentioned family history of skeletal disorders |
| 46 | Sifre-Ruiz et al. (2023) [ | Female | Normal | Right fibular aplasia, Right tibia shortening and campomelia, Right genu valgum and hyperflexion, Right foot oligodactyly, Right split foot malformation, Right clubfoot | None | Non-consanguineous parents, not mentioned family history of congenital or skeletal disorders |
| 47 | Current study | Male | Left ulnae hypoplasia, Bilateral oligosyndactyly, Bilateral split hand malformation | Right fibular aplasia, Right tibia shortening and campomelia, Bilateral oligosyndactyly | None | Non-consanguineous couple, not mentioned family history of congenital or skeletal disorders |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital limb and hand anomalies · Prenatal Screening and Diagnostics · Genomic variations and chromosomal abnormalities
Introduction
Congenital limb anomalies are common skeletal birth defects, affecting one in 1,000 births [1], with anomalies in upper limbs clearly dominating [2]. It has been estimated that over 15% of all limb defects concern the split-hand foot malformation (SHFM), a congenital distal limb absence mainly observed in the central rays of hands and/or foot [3,4].
In the literature, SHFM has been also described as “ectrodactyly”, “cleft hand”, “lobster claw hand”, “crab claw hand” and “symbrachydactyly” [5]. The incidence of SHFM is one in 18,000 newborns. Among those, 80% present with only a single abnormal limb, mainly affecting the upper limbs [6,7]. SHFM demonstrates a wide heterogeneity in clinical severity, even among different limbs of an individual, and generally is shown in an asymmetric pattern between left and right limbs [8].
The typical type is defined by the absence of the central rays resulting in a cleft appearance, but also oligodactyly, monodactyly, syndactyly, camptodactyly, clinodactyly, metacarpal or metatarsal, and phalangeal aplasia can occur [3,4,9]. This rare condition can be non-syndromic, mostly associated with autosomal dominant inheritance with variable expressivity and reduced penetrance [8], or part of a syndrome involving other extra-limb abnormalities [9], as more than 50 syndromes have been associated with SHFM [10]. The most frequent SHFM-associated syndromes are ectrodactyly-ectodermal dysplasia-cleft lip and palate (EEC), acro-derma-to-ungual-lacrimal-tooth (ADULT), lacrimo-auriculo-dento-digital (LADD), and limb-mammary syndrome [3,4].
SHFM associated with long bone deficiency has been termed the split hand/foot syndrome with long bone deficiency (SHFLD) syndrome, an extremely rare defect occurring in one in 1,000,000 newborns [11]. In this condition, SHFM is almost always accompanied by tibial aplasia or hypoplasia and generally an intact fibula. Less frequent long bone anomalies concern defects of the femur and ulnae [10,12,13].
On the other hand, fibular aplasia-tibial campomelia-oligosyndactyly (FATCO) syndrome was first described by Hetch et al. in 1981 [14]. Since then, only a few cases have been reported in the literature as fibular aplasia, tibial campomelia, and oligosyndactyly [15].
In this study, we report the postnatal findings in a fetus 21+6 weeks after elective termination of pregnancy due to multiple limb anomalies and we summarize the literature concerning these uncommon conditions.
Case presentation
A 36-year-old healthy Caucasian primigravida with no exposure to radiation or drug intake, requested a pregnancy termination at 22 weeks after the second-trimester scan, as the fetus was diagnosed with upper and lower limb abnormalities. The parents were nonconsanguineous and family history was referred unremarkable. The fetus was delivered at the Laboratory of Histology-Embryology of Democritus University of Thrace (DUTH), Greece, and clinical examination and X-ray were performed to establish the diagnosis.
Fetal autopsy in upper limbs revealed bilateral split hand malformation with an asymmetric pattern in left-right abnormalities. Absence of both thumbs and bilateral oligosyndactyly were observed. Ectrodactyly of the right hand involved the absence of two digits (thumb and fifth) resulting in a median cleft and soft tissue syndactyly of second and third digits. On the left hand, the thumb and a central digit were missed, whereas the fifth digit was present but dysmorphic and hypoplastic (Figure 1). Clinical examination of the lower limbs showed shortening of the right limb, anterior bowing in the right tibia with skin dimpling, bilateral oligodactyly, and bilateral cutaneous incomplete syndactyly (Figure 1).
Post-abortum photograph of fetus showing bilateral ectrodactyly of upper limbs with right lower limb shortening, anterior bowing, and overlying skin dimpling with associated bilateral feet oligosyndactyly.
Radiographic evaluation of upper limbs revealed missing metacarpal bones and digits, bilaterally. Ulnae hypoplasia was detected on the left limb. On the right hand, two metacarpals and three proximal and three distal phalanges were observed. The left hand comprised two metacarpals and two phalanges (Figure 2A). X-ray examination of lower limbs showed skeletal malformation on the right side with complete fibular aplasia. The presence of campomelic and shortened right tibia was also confirmed. On each foot, four metatarsal bones and four well-formed digits were observed (Figure 2B).
(A) Fetal X-ray showing bilateral hand malformations and left ulnae hypoplasia; (B) Radiograph of lower limbs showing right fibular aplasia and tibial campomelia with missing metatarsal bones and digits bilaterally.
No other anomalies of the spine, pelvis, or skull were detected. External genitalia were normal. No facial malformations or other external abnormalities were detected. Karyotype analysis revealed a normal male karyotype (46, XY).
Discussion
In this report, we presented a case of a male fetus with both FATCO and SHFLD syndromes present. To the best of our knowledge, till date, this is the first report of a case with the coexistence of these two extremely rare syndromes in the literature.
SHFLD is defined by the presence of upper or lower limb ectrodactyly and long bone defects. As previously reported, SHFLD is mainly associated with tibial aplasia or hypoplasia [12,16] and ectrodactyly phenotype may show significant heterogeneity, as presented in Figure 3.
Schematic representation of various split hand malformations, including our case.(A) Dorsal view of bidactylous with thumb and one digit separating by a cleft; (B) Dorsal view of hand with syndactyly and two mild clefts; (C) Dorsal view of split hand with three malformed digits and large cleft extended to the carpometacarpal joint; (D) Absence of the thumb and one digit, median cleft, and syndactyly (right hand of our case); (E) Palmar view of a hand with the absence of the third digit and median cleft; (F) Dorsal view of ectrodactyly with only two digits present separating by a large cleft; (G) Dorsal view of split hand with thumb and two digits; (H) Ectrodactyly with thumb and a central digit absent, hypoplasia of fifth digit, and syndactyly of two central digits (left hand of our case).Image Credit: Vaya Karapepera
SHFLD cases with defective femur, ulnae, or radius have also been reported [13,17,18]. To the best of our knowledge, no reported SHFLD case with tibial campomelia has been recorded in the literature [9,16,19]. Furthermore, a common locus for SHFLD is that it rarely affects the fibula [12]. These findings played a major role in leading us to strongly believe that in this case, two separate clinical syndromes coexist.
The most common long bone agenesis is considered to be fibular aplasia [20], which can occur besides FATCO syndrome, in other conditions like femur-fibula-ulna (FFU) syndrome, Furhmann syndrome, Du Pan syndrome, and thrombocytopenia-absent radius (TAR) syndrome [1]. The main diagnostic finding that can differentiate FATCO syndrome from other fibula-related entities is the absence of femoral and radial defects [21]. In particular, Furhmann syndrome which has been already presented in the literature to overlap with FATCO syndrome [22], in this case, was ab initio excluded by the confirmation of the straight femora. Normal femora should also rule out the diagnosis of FFU syndrome [1]. Fibular aplasia with ectrodactyly has been considered by some as the clinical entity that should include FATCO syndrome [23], but in the literature, there is no agreement [22,12]. Isik et al. recently suggested that ectrodactyly with fibular aplasia and no additional findings should be considered as FATCO syndrome [24]. However, as the etiology of FATCO remains unclear, the vast majority of cases demonstrating the clinical triad of fibular aplasia, tibial campomelia, and oligosyndactyly are considered FATCO syndrome [1,11,22,24].
It is suggested that the diagnosis of FATCO syndrome should initially be based on abnormalities of lower limbs. Then, all associated syndromes should be ruled out based on phenotypic features. Of course, the scenario of overlapping conditions should be kept in mind, as these clinical entities may share a common genetic basis [25].
In general, FATCO syndrome is an extremely rare condition, with less than 30 cases reported worldwide [1,2,26]. After a thorough review of the literature [1,2,11,12,14,15,20-48], we found that the total number of cases increases to 46 if FATCO variants are also included (Table 1) [27-29]. It is noteworthy to clarify that previous studies included some cases demonstrating the characteristics of FATCO syndrome which, however, had been diagnosed as fibular hemimelia [30,31]. On the other hand, two cases of Fuhrmann syndrome were presented by Huber et al. in 2003. Regarding these cases, the authors strongly believe that they should be counted as FATCO syndrome because the femora and pelvis were found normal, thus the diagnosis of Fuhrmann syndrome was excluded [32]. For this reason, in the newest studies, these incidents were included as FATCO syndrome [11,33,34].
Among all the reported cases, a wide range of variability has been demonstrated [35,36]. However, common findings in FATCO syndrome include the tendency to affect the right side, the anterior bowing of the tibia, and the skin dimpling located in the distal third [21], as observed in our case.
Based on our literature search, almost half of FATCO cases have been recorded in Asia with Turkey and India with the majority of cases. Interestingly, cases in which parental consanguinity was declared were also observed in these countries (Table 1) [37-48]. Based on clinical and radiographical findings, we report here the first case with FATCO syndrome presented in Greece demonstrating the classic triad in lower extremities: fibular aplasia, tibial campomelia, and bilateral oligosyndactyly. Concurrently, the diagnosis of SHFLD was made with the clinical detection of ectrodactyly of upper limbs and the presence of left ulnae hypoplasia on X-ray imaging.
To date, the majority of published FATCO syndrome cases provided clinical data from the postnatal period. Our study is one of the few that highlights the fetal phenotypic features, aiming to familiarize fetal physicians with this rare condition, as prenatal diagnosis and counseling could be essential in the management of these cases. Taking into account the above-mentioned cases, it seems that our case is the second FATCO case overlapping with another limb syndrome, the first being reported by Abdalla et al. [22], which in this instance involves the upper limbs.
According to the most recent study, the involvement of the upper limb in FATCO syndrome seems to be rare, as only a few cases were recorded with upper limb defects, exclusively located in the hands [11]. For that reason, the presence of exhibited unilateral ulnae hypoplasia, which is a finding that had never been associated with FATCO syndrome (Table 1), raised the suspicion in our case that two distinct abnormal entities concurrently exist. Based on previously reported cases, a male preponderance has been established in FATCO syndrome [2] and the sex ratio (male/female), including our case, is now approximately estimated at 2:1 (Table 1).
Conclusions
In this report, we presented an extremely unusual case of a fetus with a phenotype of FATCO syndrome associated with another rare upper limb disorder, SHFLD. To the best of our knowledge and based on the literature search presented, this is the first case with both FATCO syndrome and SHFLD reported. Considering the high clinical and genetic heterogeneity of these conditions, the diagnosis often seems to be difficult. Our case may contribute to further understanding of these rare conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prenatal diagnosis of fibular aplasia-tibial campomelia-oligosyndactyly syndrome: two case reports and review of the literature J Clin Ultrasound Marinho M Nunes S Lourenço C Melo M Godinho C Nogueira R 6256294920213333097410.1002/jcu.22969 · doi ↗ · pubmed ↗
- 2Newborn male with fibular aplasia, tibial campomelia, and oligosyndactyly syndrome: a new case report putting the condition under spotlight Cureus Georgeos MK Elgzzar DR 014202210.7759/cureus.21702 PMC 888237335237492 · doi ↗ · pubmed ↗
- 3Clinical, genetic, and molecular aspects of split-hand/foot malformation: an update Am J Med Genet A Gurrieri F Everman DB 28602872161 A 20132411563810.1002/ajmg.a.36239 · doi ↗ · pubmed ↗
- 4Insights into the pathogenesis and treatment of split/hand foot malformation (cleft hand/foot)J Hand Surg Eur Vol Guero S Holder-Espinasse M 80874420193038099010.1177/1753193418807375 · doi ↗ · pubmed ↗
- 5Insights into the pathogenesis and treatment of split/hand foot malformation (cleft hand/foot)J Hand Surg Eur Vol Guero S Holder-Espinasse M 80874420193038099010.1177/1753193418807375 · doi ↗ · pubmed ↗
- 6Prenatal diagnosis of ectrodactyly in the first trimester by three-dimensional ultrasonography AJP Rep Blitz MJ Rochelson B 046201610.1055/s-0036-1579653 PMC 479443726989570 · doi ↗ · pubmed ↗
- 7An unusual presentation of bilateral split hand-foot malformation (SHFM) in family: a tale of two generations Curr Health Sci J Singh SV Puri G Gemmy AE 3563594820223681508010.12865/CHSJ.48.03.16PMC 9940929 · doi ↗ · pubmed ↗
- 8Genetic regulatory pathways of split-hand/foot malformation Clin Genet Kantaputra PN Carlson BM 1321399520193010146010.1111/cge.13434 · doi ↗ · pubmed ↗