Association of maternal infection of SARS-CoV-2 and neonatal susceptibility: A retrospective cohort study
Xiao-Dan Zhu, Yan-Jie Peng, Ying Chen, Mei Xue, Ai-Juan Zhang, Yu Peng, Rong Mei, Mei-Rong Tian, Lin Zhang

TL;DR
This study found that maternal SARS-CoV-2 infection and vaccination during pregnancy may reduce the risk of neonatal infection.
Contribution
The study identifies maternal infection and vaccination as protective factors against neonatal SARS-CoV-2 infection.
Findings
Maternal vaccination reduced neonatal infection risk by 37%.
Maternal SARS-CoV-2 infection reduced neonatal infection risk by 55%.
Higher BMI and older age at first pregnancy increased neonatal infection risk.
Abstract
This study aims to assess the risk of neonatal susceptibility to COVID-19 among pregnant women. We conducted a retrospective cohort study involving 1089 pregnant women ≥28 weeks of gestational age, who were categorized into infected and uninfected groups. Data for all participants were collected through a comprehensive review of electronic medical records and follow-up phone calls. The primary outcome was neonatal infection with SARS-CoV-2, while secondary outcomes included delivery patterns and gestational age at delivery. Maternal vaccination (OR 95%CI:0.63[0.46, 0.85]) and maternal infection with SARS-CoV-2 (OR 95%CI: 0.45[0.34, 0.60]) were found to be associated with a decreased risk of neonatal infection. The infected group exhibited a lower neonatal SARS-CoV-2 infection rate (25.93%) compared to the uninfected group (45.15%). Logistic regression analysis identified several risk…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
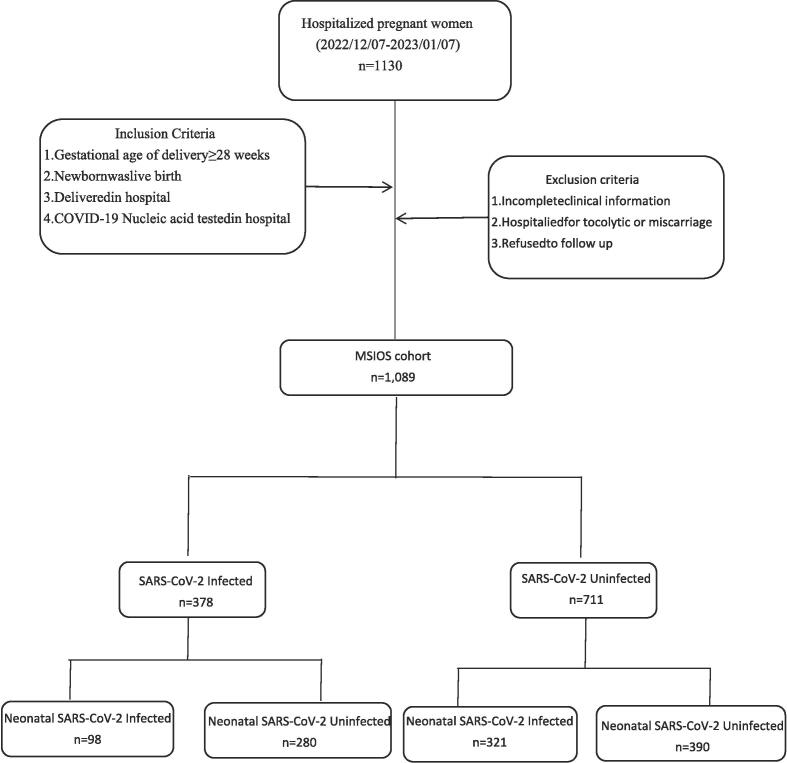 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Impact on Reproduction · Maternal Mental Health During Pregnancy and Postpartum · Pregnancy and Medication Impact
Introduction
1
Coronavirus disease 2019 (COVID-19) is a highly contagious respiratory disease caused by SARS-CoV-2, its most common clinical symptoms include fever, cough, fatigue, headache, dyspnea, and diarrhea [1]. The World Health Organization (WHO)declared the COVID-19 outbreak as the sixth public health emergency of international concern on January 30,2020 then proclaimed it a global pandemic on March 11, 2020[2], [3]. More than 15 million people have died in the pandemic [4]. When loosened the COVID-19 restrictions on December 7,2022 in China, a large influx of pregnant women infected with COVID-19 posed a huge challenge for obstetricians to ensure the safety of mothers and infants.
Due to changes in physical, physiological, and immunosuppressive status, pregnant women are particularly prone to respiratory infections and severe pneumonia [5]. The mortality rate of pregnant women infected with SARS-CoV-2 is as high as 0.9 %[6]. Some studies suggest that infection with SARS-CoV-2 during pregnancy is associated with many adverse pregnancy outcomes, including pre-eclampsia, premature birth, and stillbirth, especially in pregnant women with severe COVID-19 disease [7], [8], [9]. However, others indicate that maternal infection with SARS-CoV-2 during pregnancy usually do not have severe consequences on mother and child [10], [11], [12]. As mentioned above, most of the studies mainly focus on the maternal and fetal outcomes in COVID-19-positive pregnant women, there is scarcely research on the susceptibility of newborns with SARS-CoV-2, and therefore this comparative retrospective cohort study was conducted with the aim to identify the risk of maternal SARS-CoV-2 infection on neonatal susceptibility.
Methods
2
Data source and study design
2.1
This retrospective cohort study involved 1089 pregnant women who were hospitalized in Shandong Provincial Maternal and Child Health Care Hospital between November 7, 2022 and January 7,2023, one month before and after the easing of COVID-19 control measures in China. The cohort had been registered and named Maternal SARS-CoV-2 Infection and Offspring Susceptibility (MSIOS, clinical registration number: MR-37-23-019409). All patient data including demographic characteristics, medication, and laboratory examination results were obtained from reviewing electronic medical records. Additional information, such as COVID-19 symptoms in pregnant women, paternal baseline characteristics, and neonatal SARS-CoV-2 infection status, were obtained by following up the patients within one month after discharge. The study was approved by the Institutional Review Board of the Shandong Provincial Maternal and Child Health Care Hospital Affiliated to Qingdao University. The personal information of all study participants was anonymized prior to statistical analysis.
Patient selection and cohorts
2.2
This study included a cohort of admitted pregnant women for delivery, and all study subjects were enrolled if they(a)The gestational age of delivery was more than 28 weeks,(b)The newborn was live birth,(c)Delivered in the hospital (natural delivery or Caesarean section),(d)COVID-19 Nucleic acid test was performed in the hospital (recorded positive polymerase chain reaction test negative or positive). If the pregnant women had incomplete clinical information, hospitalized for preventing miscarriage therpay or miscarriage, and refused to follow up would be excluded. All pregnant women with previous COVID-19 infections were also be excluded. The infection of SARS-CoV-2 was determined by nucleic acid test, with or without the presence of clinical symptoms such as fever, cough, shortness of breath or difficulty breathing, fatigue, muscle or body aches, headache, new loss of taste or smell, and sore throat. Finally, 1089 cases were included in the study and divided into two groups according to the infectious status of SARS-CoV-2 (Fig. 1).Fig. 1. The algorithm of study subject selection. Abbreviation: MSIOS, The cohort registered and named as Maternal SARS-CoV-2 Infection and Offspring Susceptibility.
Covariates and outcomes
2.3
All covariates were determined and included from variables that may influence maternal and fetal health, and were considered from three aspects of maternal, paternal, and neonatal. Maternal factors included age, BMI, education level, prenatal vaccination status, folic acid supplementation, medication use during pregnancy, age at first pregnancy and menarche, the number of parturitions, history of preterm birth or abortion, menstrual cycle regularity, gestational age at delivery, delivery mode, and conception method. Paternal factors included age, BMI, cigarette and alcohol consumption, and education level. Neonatal factor was the sex of the newborn. The primary outcome of the study was neonatal infection with SARS-CoV-2, and the secondary outcomes were delivery pattern and gestational age at delivery.
Statistical analysis
2.4
All data were collected using Microsoft Excel 2019 then visualized and statistically analyzed using R version 4.3.0 for Windows. Baseline characteristics were described as median with interquartile range for continuous variables and frequency with proportion for categorical variables. A logistic regression model was established to predict the risk of neonatal infection with SARS-CoV-2. A two-tailed p-value < 0.05 was considered statistically significant.
Results
3
Demographic characteristics of study subjects
3.1
A total of 1089 hospitalized pregnant women from November 7,2022 to January 7,2023 were included in this cohort. of these, 378 were diagnosed with COVID-19 and 711 were not (Table 1). Compared to the uninfected group, the infected pregnant women had lower rate of folic acid supplementation. The pregnancy body mass index, maternal vaccination rate, pregnancy medication in the infected group were higher than that in the uninfected group. The differences of other indicators were of no statistical significance between these two groups.Table 1. Baseline characteristics of study pregnant women and comparison between the SARS-CoV-2 infected and uninfected groups.ALL(n = 1089)Uninfected(n = 711)Infected Control group(n = 378)p valueMaternal factorsAge at pregnancy (yrs)31.00 [28.00;33.00]30.00 [28.00;33.00]31.00 [28.00;34.00]0.359Pregnancy BMI (kg/m^2^)26.73 [24.09;29.36]26.64 [23.73;29.22]26.87 [24.61;29.57]0.048Education background (n)0.092 High school and the following degree130(11.94 %)94(13.22 %)36(9.53 %) University Graduate806 (74.01 %)515 (72.43 %)291 (76.98 %) Postgraduate153 (14.05 %)102 (14.35 %)51 (13.49 %)SARS-CoV-2 infection (n)− Infected378 (34.71 %)−− Uninfected711(65.29 %)−−Prenatal vaccination (n)0.004 Yes846 (77.69 %)533 (74.96 %)313(82.80 %) No243 (22.31 %)178 (25.04 %)65(17.20 %)Folic acid supplementation (n)0.001 Yes1026 (94.21 %)683 (96.06 %)343 (90.74 %) No63 (5.79 %)28 (3.94 %)35 (9.26 %)Pregnancy medication(n)0.040 Yes91 (8.36 %)58 (8.22 %)38 (9.92 %) No998(91.64 %)648 (91.78 %)345 (90.08 %)Age at first pregnancy (yrs)28.00 [25.00;30.00]28.00 [25.00;30.00]27.00 [25.00;29.75]0.328Delivery history0.643 0441 (40.50 %)292 (41.07 %)149 (39.42 %) 1648 (59.50 %)419 (58.93 %)229 (60.58 %)History of preterm birth (n)0.092 01069 (98.16 %)702 (98.73 %)367 (97.09 %) ≥120 (1.84 %)9 (1.27 %)11 (2.91 %)History of Abortion (n)0.927 01029 (94.49 %)671 (94.37 %)358 (94.71 %) ≥160 (5.51 %)40 (5.63 %)20 (5.29 %)Age at menarche (yrs)14.00 [14.00;14.00]14.00 [14.00;14.00]14.00 [14.00;14.00]0.037Menstrual days (days)6.00 [5.50;6.00]6.00 [5.50;6.00]6.00 [5.50;6.00]0.743Menstrual cycle days (days)30.00 [30.00;30.00]30.00 [30.00;30.00]30.00 [30.00;30.00]0.425Menstrual cycle regularity (n)0.142 Regular1013 (93.02 %)655 (92.12 %)358 (94.71 %) Irregular76 (6.98 %)56 (7.88 %)20 (5.29 %)Conception method (n)0.986 Artificial technology56 (5.14 %)36 (5.06 %)20 (5.29 %) Natural pregnancy1033 (94.86 %)675 (94.94 %)358 (94.71 %)Paternal factorsAge30.00 [27.00;34.00]30.00 [27.00;34.00]30.00 [27.00;34.00]0.234BMI24.80 [22.86;27.17]24.84 [23.01;26.99]24.67 [22.61;27.70]0.697Smoke consumption(n)0.420 Yes303 (27.82 %)204 (28.69 %)99 (26.19 %) No786 (72.18 %)507 (71.31 %)279 (73.81 %)Alcohol consumption (n)0.492 Yes417 (38.29 %)278 (39.10 %)139 (36.77 %) No672 (61.71 %)433 (60.90 %)239 (63.23 %)Education background (n)0.798 High school and the following degree196 (18.00 %)133(18.70 %)63 (16.67 %) University Graduate746 (68.50 %)480 (67.51 %)266 (70.37 %) Postgraduate147 (13.50 %)98 (13.78 %)49 (12.96 %)Abbreviations: BMI, body mass index. Values reported for continuous variables are medians with interquartile ranges (IQR).
Primary and secondary outcomes
3.2
Compared to the uninfected group, the rate of neonatal infection with SARS-CoV-2 was lower in the infected group, with 321 cases in the uninfected group and 98 cases in the infected group, accounting for 45.15 % and 25.93 %, respectively(Table 2). There were no statistically significant differences between the infected and uninfected groups with regard to the rate of vaginal delivery or gestational age at delivery. Also, no significant differences were observed between paternal factors and other neonatal outcomes.Table 2. The outcomes of the maternal and neonatal between the SARS-CoV-2 infected and uninfected groups.ALL (n = 1089)Uninfected(n = 711)Infected Control group (n = 378)P valueDelivery outcomesDelivery weeks39.29 [38.57;40.14]39.29 [38.50;40.14]39.29 [38.57;40.14]0.898Delivery mode (n)0.626 Vaginal delivery626 (57.48 %)413 (58.09 %)213 (56.35 %) Cesarean delivery463 (42.52 %)298 (41.91 %)165 (43.65 %)Neonatal factorsSARS-CoV-2 infection (n)<0.001 Infected419 (38.48 %)321 (45.15 %)98 (25.93 %) Uninfected670 (61.52 %)390 (54.85 %)280 (74.07 %)Sex assigned at birth (n)1.000 Male556 (51.06 %)363 (51.05 %)193 (51.06 %) Female533 (48.94 %)348 (48.95 %)185 (48.94 %)Birth weight3300.00 [3020.00;3550.00]3290.00 [3000.00;3560.00]3300.00 [3022.50;3550.00]0.477
Logistic regression analysis of risk factors for neonatal SARS-CoV-2 infection
3.3
The results of the logistic regression analysis(Table 3) showed that there was an increased risk of neonatal SARS-CoV-2 infection rate regarding the pregnancy BMI (OR 95 %CI: 1.04[1.01, 1.08]), age at first pregnancy (OR 95 %CI: 1.05[1.01, 1.10]), age at menarche (OR 95 %CI: 1.13[1.02, 1.26]) and parturition(Yes vs. No) (OR 95 %CI:1.4 [1.04,1.88]), while the decreased risk for neonatal infection was determined in maternal vaccination (OR 95 %CI:0.63[0.46, 0.85]) and maternal infection of SARS-CoV-2 (OR 95 %CI: 0.45[0.34, 0.60]).Table 3. Logistic regression analysis of neonatal infection with SARS-CoV-2.Variablescrude OR(95 %CI)adj. OR(95 %CI)P valueAge at pregnancy (yrs)1 (0.97,1.03)0.98 (0.94,1.02)0.27Pregnancy BMI (kg/m^2^)1.04 (1.01,1.07)1.04 (1.01,1.08)0.011Vaccination Yes vs. No0.61 (0.46,0.82)0.63 (0.46,0.85)0.003Age at menarche (yrs)1.17 (1.06,1.29)1.13 (1.02,1.26)0.009Parturition Yes vs. No1.27 (0.99,1.63)1.4 (1.04,1.88)0.026Menstrual days1.05 (0.91,1.21)1.08 (0.93,1.26)0.315Age at first pregnancy (yrs)1.02 (0.99,1.06)1.05 (1.01,1.1)0.025Menstrual cycle days0.995 (0.98,1.01)0.9913 (0.98,1.00)0.1Conception methodNatural vs. Artificial1.23 (0.7,2.17)1.28 (0.69,2.38)0.436Folic acid supplementation Yes vs. No1.3682 (0.79,2.36)1.0022 (0.56,1.78)0.994Pregnancy medication: Yes vs. No0.77 (0.49,1.21)0.76 (0.47,1.23) y0.253Maternal SARS-CoV-2 infectionInfected vs. Uninfected0.43 (0.32,0.56)0.45 (0.34,0.6)< 0.001GDM Yes vs. No0.96 (0.74,1.27)1.02 (0.77,1.37)0.872Paternal age0.99 (0.96,1.01)0.98 (0.95,1)0.077Paternal smoking Yes vs. No1.24 (0.95,1.63)1.31 (0.95,1.8)0.096Paternal drinking Yes vs. No1.04 (0.81,1.34)0.95 (0.71,1.26)0.705Paternal BMI (kg/m^2^)0.9951 (0.96,1.03)0.994 (0.96,1.03)0.737Preterm Birth Yes vs. No1.01 (0.56,1.82)1.17 (0.63,2.19)0.615Abbreviation: GDM, gestational diabetes mellitus, BMI, body mass index.
Discussion
4
During the COVID-19 pandemic, it has been a critical issue on how to protect young children from infection. Previous studies have suggested several strategies for reducing the risk of infection among young children, including vaccination of eligible household members, avoiding large crowds and maintaining physical distance, wearing masks in indoor public spaces or crowded outdoor settings, practicing good hand hygiene, and staying home when sick. However, the protective effects of maternal infection on neonates remain a subject of debate.
In this study, we found that maternal vaccination or perinatal infection with COVID-19 had protective effects on the newborn. These findings are consistent with a study conducted in Israel with 1094 participants, which showed that antenatal BNT162b2 mRNA vaccination elicited a strong maternal humoral IgG response that crossed the maternal-fetal interface and approached maternal titers in the fetus within 15 days following the first dose. Furthermore, the ratio of maternal to neonatal anti-COVID-19 antibodies did not differ when comparing sensitization (vaccine vs. infection)[13]. Similar studies indicated that COVID-19 vaccination during pregnancy can produce functional IgG antibodies in maternal circulation, which had been detected in cord blood at birth, and can protect newborns and infants from COVID-19 infection [14], [15], [13]. A study published by the JAMA Pediatrics manifested that the COVID-19 antibody in mother can not only be transmitted to the baby through the maternal fetal barrier, but also through breastfeeding[16]. There was a significant and positive correlation between maternal serum levels of SARS-Cov-2 IgG and cord blood (R = 0.483, p = 0.0001), neonatal blood spot (R = 0.515, p = 0.004), and breast milk levels (R = 0.396, p = 0.005) of SARS-CoV-2 IgG[17]. During breastfeeding, IgA, IgG and IgM confer neonatal mucosal immune protection by binding to commensal and pathogenic microbes and their virulence factors to mediate immune exclusion and neutralization [18].
Comparison of vaccinated with convalescent COVID-19 patients revealed significantly increased SARS −CoV-2 IgG levels in maternal serum and cord blood among vaccinated women (p < 0.001) [17]. Therefore, vaccination of pregnant women was an effective protective method for newborns to from infection. FIGO considered “there are no risks—actual or theoretical—that would outweigh the potential benefits of vaccination for pregnant women. We support offering COVID-19 vaccination to pregnant and breastfeeding women” [19]. Data from more than 180,000 vaccinated persons show that immunization against COVID-19 with an mRNA vaccine is safe for pregnant women [20]. Also, Vaccination of pregnant people reduces the COVID-19-related increase in maternal or fetal morbidity [21]. An interesting finding in our study was that the vaccination rate of pregnant women infected with COVID-19 was higher than that of the uninfected group, accounting for 37 % in infected group and 26.7 % in uninfected group, which seems contradictory. However, there may be three reasons. Firstly, the higher infection rate in vaccinated women compared to unvaccinated women could be due to a higher proportion of previously infected women with naturally acquired immunity in the latter group, women with a prior infection are more likely to have not received a COVID-19 vaccine because protected by natural immunity. Secondly, according to China's national conditions during the COVID-19 pandemic, pregnant women were not recommended to be vaccinated. Moreover, different doses of vaccination may produce different immune results. Lastly, the pregnant women who were not vaccinated had stronger sense of self-protection. In order to avoid infection, they may pay more attention to their hand hygiene and quarantine themselves conscientiously.
It is still inconsistent whether COVID-19 can affect the pattern of pregnancy delivery[22], [23], [24], [25], [8]. Although COVID-19 was not the indication of caesarean section, most studies showed that caesarean section was the primary choice of delivery for COVID-19 patients[22], [23]. Consistently, some studies reported similar findings with us[24], [8], where the rate of caesarean section in the infected group was higher as compared to the control, but we did not find statistical significances. Some studies focused on the impact of COVID-19 on preterm delivery, insisting that COVID-19 would lead to an increase in preterm delivery rate [24], [7]. The delivery weeks in our study had no statistical differences which was 39.29 [38.50;40.14] in the uninfected group and 39.29 [38.57;40.14] in the infected group.
This study has several strengths as it used information from parents to study the susceptibility of newborns to SARS-CoV-2 for the first time. The valuable information includes mother's Body mass index, mother's delivery history and menarche age which may provide some useful information for reducing the susceptibility of newborns. Also, there are several limitations in the study. Firstly, most of the pregnant women in this cohort were infected in the third trimester, and the extended studies need to include cases in the first and second trimester which make the study more comprehensive. Secondly, it is a single center study although the number of cases in this study exceeds one thousand. Further research needs to incorporate multi-center studies to make them more convincing. Thirdly, the limitation of this retrospective cohort study lies in the lack of prospective standardization in the detection, diagnosis, and management of COVID-19. The information collected through telephone interview may have introduced a desirability bias, such as the infections of newborns and father's habits that may be perceived as undesirable behaviours (e.g., smoking or alcohol consumption). Due to the reliance of this study on medical record data, there may be inconsistencies in the COVID-19 testing protocol, diagnostic criteria, and treatment methods between the entire study period and patients. The lack of standardized prospective testing, diagnosis, and treatment plans may lead to bias or affect observation results. A prospective study with predefined protocols will help standardize these factors and provide stronger evidence for the protective effects of COVID-19 infection in pregnant women and vaccination on neonatal susceptibility.
In conclusion, maternal vaccination (OR 95 %CI:0.63[0.46, 0.85]) or maternal infection with SARS-CoV-2 (OR 95 %CI: 0.45[0.34, 0.60]) can reduce the susceptibility of the newborn in the infected group. These findings provide strong evidence to support the vaccination of pregnant women against COVID-19, which can benefit not only the mother but the newborn by reducing the risk of infection.
Ethical approval statement
The study was approved by the Institutional Review Board of the Shandong Provincial Maternal and Child Health Care Hospital Affiliated to Qingdao University. The personal information of all study participants was anonymized prior to statistical analysis.
Funding
This study was supported by the Taishan Scholar Program of Shandong Province (No. tsqn202211359).
CRediT authorship contribution statement
Xiao-Dan Zhu: Writing – review & editing, Writing – original draft. Yan-Jie Peng: Investigation, Formal analysis, Data curation. Ying Chen: Investigation, Data curation. Mei Xue: Investigation, Data curation. Ai-Juan Zhang: Investigation, Formal analysis. Yu Peng: Investigation, Formal analysis, Data curation. Rong Mei: Formal analysis, Data curation. Mei-Rong Tian: Investigation, Data curation. Lin Zhang: Writing – review & editing, Supervision, Project administration, Conceptualization.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ochani R.Asad A.Yasmin F.Shaikh S.Khalid H.Batra S.COVID-19 pandemic: from origins to outcomes. A comprehensive review of viral pathogenesis, clinical manifestations, diagnostic evaluation, and management Infez Med 2912021 Mar 1203633664170 · pubmed ↗
- 2Lai C.C.Shih T.P.Ko W.C.Tang H.J.Hsueh P.R.Severe acute respiratory syndrome coronavirus 2 (SARS-Co V-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges Int J Antimicrob Agents 5532020 Mar 10592410.1016/j.ijantimicag.2020.105924 PMC 712780032081636 · doi ↗ · pubmed ↗
- 3Beig Parikhani A.Bazaz M.Bamehr H.Fereshteh S.Amiri S.Salehi-Vaziri M.The inclusive review on SARS-Co V-2 biology, epidemiology, diagnosis, and potential management options Curr Microbiol 7842021 Apr 109911143363867110.1007/s 00284-021-02396-x PMC 7913045 · doi ↗ · pubmed ↗
- 4Adam D.15 million people have died in the pandemic, WHO says Nature 60579092022 May 2063551345510.1038/d 41586-022-01245-6 · doi ↗ · pubmed ↗
- 5Jamieson D.J.Theiler R.N.Rasmussen S.A.Emerging infections and pregnancy Emerg Infect Dis 12112006 Nov 163816431728361110.3201/eid 1211.060152 PMC 3372330 · doi ↗ · pubmed ↗
- 6Wang H.Li N.Sun C.Guo X.Su W.Song Q.The association between pregnancy and COVID-19: A systematic review and meta-analysis Am J Emerg Med 562022 Jun 1881953541365510.1016/j.ajem.2022.03.060PMC 8986277 · doi ↗ · pubmed ↗
- 7Jamieson D.J.Rasmussen S.A.An update on COVID-19 and pregnancy Am J Obstet Gynecol 22622022 Feb 1771863453449710.1016/j.ajog.2021.08.054PMC 8438995 · doi ↗ · pubmed ↗
- 8Villar J.Ariff S.Gunier R.B.Thiruvengadam R.Rauch S.Kholin A.Maternal and neonatal morbidity and mortality among pregnant women with and without COVID-19 infection: the INTERCOVID multinational Cohort Study JAMA Pediatr 17582021 Aug 18178263388574010.1001/jamapediatrics.2021.1050 PMC 8063132 · doi ↗ · pubmed ↗