An Investigation of Mortality Associated With Comorbid Pneumonia and Thrombocytopenia in a Rural Southwest Missouri Hospital System
Tabitha Ranson, Hannah Rourick, Rajbir Sooch, Nicole Ford, Nova Beyersdorfer, Kerry Johnson, John Paulson

TL;DR
This study found that patients with both pneumonia and low platelet count (thrombocytopenia) had significantly higher mortality rates compared to those with pneumonia alone.
Contribution
The study provides new evidence on the increased mortality risk associated with comorbid pneumonia and thrombocytopenia in a rural hospital setting.
Findings
Patients with both pneumonia and thrombocytopenia had a 43% mortality rate, compared to 14% for those with pneumonia alone.
The mortality rate increase was 28.93% for patients with both conditions compared to those with pneumonia only.
Abstract
Background: Pneumonia places a significant burden on individuals and society, contributing to a substantial number of hospital admissions, emergency department visits, deaths, and healthcare costs each year. Comorbidities can greatly increase the risk of poor outcomes when associated with pneumonia. One comorbidity that has yet to be thoroughly researched is thrombocytopenia, which is known to play an important role in activating the immune response to infections. A decrease in platelet count may limit the immune response and consequently increase mortality in patients with pneumonia. The purpose of this study was to investigate whether comorbid thrombocytopenia and pneumonia are associated with poor outcomes. Methods: This study was a retrospective cohort analysis comparing mortality rates among patients with comorbid thrombocytopenia and pneumonia, pneumonia without thrombocytopenia,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
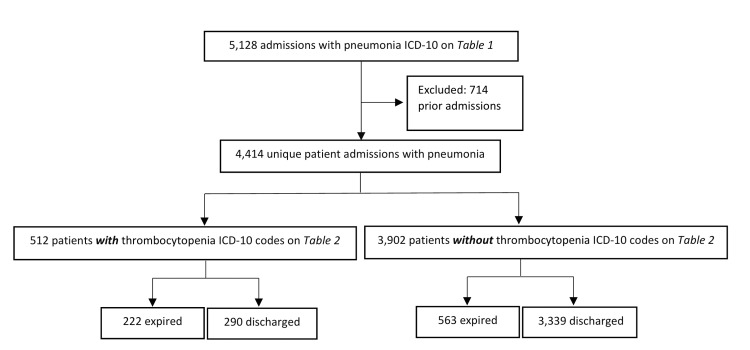 Figure 1
Figure 1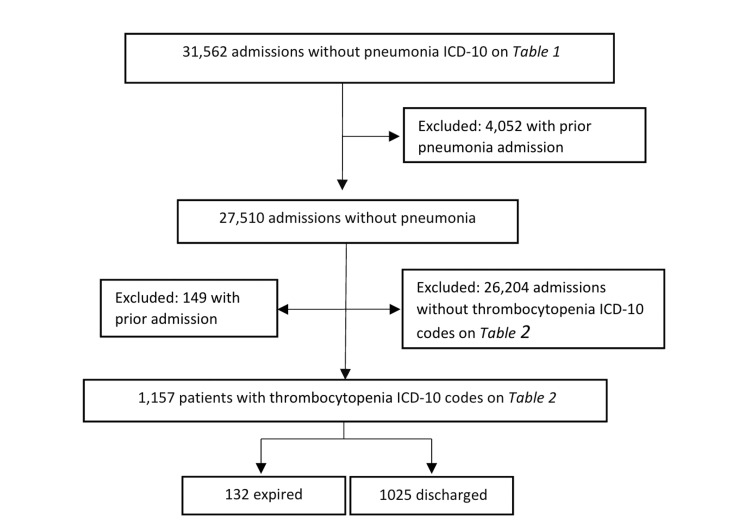 Figure 2
Figure 2| ICD-10 Code | Diagnosis |
| J1000 | Influenza due to other identified influenza viruses with unspecified types of pneumonia |
| J1001 | Influenza due to other identified influenza viruses with the same identified influenza virus pneumonia |
| J1008 | Influenza due to other identified influenza viruses with other specified pneumonia |
| J1100 | Influenza due to an unidentified influenza virus with an unspecified type of pneumonia |
| J1108 | Influenza due to an unidentified influenza virus with specified pneumonia |
| J120 | Adenoviral pneumonia |
| J121 | Respiratory syncytial virus pneumonia |
| J122 | Parainfluenza virus pneumonia |
| J123 | Human metapneumovirus pneumonia |
| J1281 | Pneumonia due to SARS-associated coronavirus |
| J1282 | Pneumonia due to coronavirus disease 2019 |
| J1289 | Other viral pneumonia |
| J129 | Viral pneumonia, unspecified |
| J13 | Pneumonia due to |
| J14 | Pneumonia due to |
| J150 | Pneumonia due to |
| J151 | Pneumonia due to |
| J1520 | Pneumonia due to |
| J15211 | Pneumonia due to methicillin-susceptible |
| J15212 | Pneumonia due to methicillin-resistant |
| J1529 | Pneumonia due to other |
| J153 | Pneumonia due to |
| J154 | Pneumonia due to other streptococci |
| J155 | Pneumonia due to |
| J156 | Pneumonia due to other gram-negative bacteria |
| J157 | Pneumonia due to |
| J158 | Pneumonia due to other specified bacteria |
| J159 | Unspecified bacterial pneumonia |
| J168 | Pneumonia due to other specified infectious organisms |
| J17 | Pneumonia in diseases classified elsewhere |
| J180 | Bronchopneumonia, unspecified organism |
| J181 | Lobar pneumonia, unspecified organism |
| J188 | Other pneumonia, unspecified organism |
| J189 | Pneumonia, unspecified organism |
| J84116 | Cryptogenic organizing pneumonia |
| J851 | Abscess of the lung with pneumonia |
| J95851 | Ventilator-associated pneumonia |
| ICD-10 Code | Diagnosis |
| D6942 | Congenital and hereditary thrombocytopenia purpura |
| D6949 | Other primary thrombocytopenia |
| D6959 | Other secondary thrombocytopenia |
| D696 | Thrombocytopenia, unspecified |
| D7582 | Heparin-induced thrombocytopenia (HIT) |
| Sample Populations | Mortality | Sample Proportion | Lower 95% CI | Upper 95% CI |
| P1 | 222 of 512 | 43.36% | 39.07% | 47.65% |
| P2 | 563 of 3902 | 14.43% | 13.33% | 15.53% |
| P3 | 132 of 1157 | 11.41% | 9.58% | 13.24% |
| Comparison | Mortality Sample 1 | Mortality Sample 2 | Sample 1 vs Sample 2 | Lower 95% CI | Upper 95% CI | P-value |
| P1 vs P2 | 222 of 512 | 563 of 3902 | 28.93% | 24.50% | 33.36% | <0.0001 |
| 43.36% | 14.43% | |||||
| P1 vs P3 | 222 of 512 | 132 of 1157 | 31.95% | 27.28% | 36.62% | <0.0001 |
| 43.36% | 11.41% | |||||
| P2 vs P3 | 563 of 3902 | 132 of 1157 | 3.02% | 0.88% | 5.16% | 0.0088 |
| 14.43% | 11.41% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections · Tuberculosis Research and Epidemiology · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
Introduction
The nationwide yearly incidence of admissions for pneumonia in the United States is estimated to be 649 hospitalizations per 100,000 adults, making it a significant healthcare and economic concern [1]. In 2022, there were 1,542,000 emergency department visits and 41,309 deaths due to pneumonia in the United States [2]. The incidence and severity of pneumonia have led to increased costs for both individual patients and hospital systems. In the United States, where pneumonia is the eighth leading cause of death, the total cost of treatment has been estimated at seventeen billion dollars per year, with the average cost of hospitalization per patient due to pneumonia being $61,928 [3, 4]. These numbers demonstrate the significant burden pneumonia places on both society and individuals. Patients with pneumonia are exceedingly prone to hospital readmission, with rates up to 20% in elderly populations [5]. As with many other diseases, when combined with comorbidities, the body’s ability to recover from pneumonia can be significantly impacted. Short- and long-term effects of pneumonia include readmission, cardiac events, cognitive impairment, and death [6]. Understanding factors that contribute to poor outcomes can inform treatment strategies to decrease secondary effects and mortality.
One possible factor contributing to poor outcomes in pneumonia is thrombocytopenia, defined as a platelet count of less than 150,000 per microliter of blood [7]. While platelets are primarily involved in hemostasis, they also have key interactions with both the innate and adaptive immune systems. Platelets utilize both direct and indirect pathways to clear bacterial pathogens from the body. Directly, platelets bind bacterial pathogens through GP1ba, GPIIb/IIIa, integrin surface receptors, and toll-like receptors, which ultimately leads to phagocytosis, intracellular killing, mechanical removal of bacteria, neutrophil extracellular trapping, and complement-induced killing [8]. When activated, platelets act indirectly by releasing granules containing chemokines that increase vascular permeability and leukocyte extravasation [8].
In addition to their role in bacterial infections, platelets have also been shown to impact the response to viral infections. A decreased platelet count is correlated with disease severity in viral infections [9]. Platelets appear to affect RNA translation, directly impacting viral replication [10]. Given the important role platelets play in both bacterial and viral infections, understanding the relationship between platelets and the immune response, and their correlation with patient outcomes, is valuable for patient care.
Given the crucial role of platelets in clearing bacterial and viral pathogens, patients with low platelet counts may have a reduced ability to fight these infections. Patients with both pneumonia and thrombocytopenia admitted to the ICU have been found to have a higher need for invasive mechanical ventilation and increased rates of sepsis [11]. Efficient recognition of this comorbidity is useful in preparing for possible complicated clinical courses and aggressive treatment plans. Therefore, patients with conditions leading to low platelets or those taking medications that decrease platelet function may be at increased risk for poor outcomes with pneumonia.
Previous studies have been limited by only examining the association between thrombocytopenia and pneumonia through the lens of specific pathogens, a singular pneumonia type, or patients within distinct units of the hospital and were often limited by small population sizes [12, 13]. This study sought to analyze a larger, more generalized population of patients within an entire hospital setting. It aims to fill the gap in current research by determining whether those with a combination of thrombocytopenia and pneumonia are at an increased risk for poor outcomes. This information is relevant to providers as it can inform treatment strategies to mitigate the risk of poor outcomes.
The purpose of this study was to investigate thrombocytopenia as a risk factor for poor outcomes in hospitalized patients with pneumonia. Given the various roles of platelets in activating the immune response to both bacterial and viral pathogens, we hypothesized that thrombocytopenia would be associated with increased mortality in patients with pneumonia compared to those without thrombocytopenia. To evaluate this hypothesis, a retrospective observational study was conducted by extracting the International Classification of Disease, Tenth Revision (ICD-10) codes for the diagnoses of pneumonia and thrombocytopenia in hospitalized patients. We then evaluated the differences in mortality rates among these populations and their comorbid states.
Materials and methods
Data collection
This retrospective observational cohort study used patient data collected from electronic medical records at Freeman Health System (FHS), a not-for-profit hospital located in Joplin and Neosho, Missouri, with 410 and 25 licensed beds, respectively. Data were extracted from discharges between January 1, 2019, and December 31, 2021. All participants were over 18 years old, with no other restrictions regarding demographics. Due to the retrospective nature of the study, informed consent was not required.
Statistical analysis
Data for our chosen patient populations were extracted using ICD-10 codes to identify patients with or without diagnoses of pneumonia and thrombocytopenia (Tables 1, 2). The initial sample of patients with a pneumonia diagnosis consisted of 5,128 patients. Exclusions were made in all groups if patients had prior admissions, leaving an initial sample size of 4,414 unique patients with a pneumonia diagnosis. Within that sample, 512 patients had both pneumonia and thrombocytopenia (P1). Additional stratification identified 3,902 patients with pneumonia but without thrombocytopenia (P2) (Figure 1). The initial sample of patients without pneumonia was 31,562, of which 4,052 were excluded due to prior admission with pneumonia. Of the remaining 27,510 patients in that sample, 1,157 were identified as having thrombocytopenia without pneumonia (P3) (Figure 2). Statistical analysis determined proportion differences between populations using two-sample proportion summary hypothesis tests. Individual sample proportions were analyzed using Wald’s method. Data were considered significant with a P-value <0.05, and a 95% confidence interval (CI) was used in the analysis.
Pneumonia population group numbers separated into categories with and without thrombocytopenia diagnoses. ICD: International Classification of Diseases.
Population group numbers of those without pneumonia separated into categories with and without thrombocytopenia diagnoses. ICD: International Classification of Diseases.
Results
The sample with pneumonia and thrombocytopenia had a mortality rate of 43.36% (95% CI: 39.07-47.65%), significantly higher than the population with pneumonia but without thrombocytopenia (Table 3). Both populations with a pneumonia diagnosis had a significantly higher mortality rate than the population without a pneumonia diagnosis. The sample with both pneumonia and thrombocytopenia had a 31.95% (P < 0.0001; 95% CI: 27.28-36.62%) higher mortality rate than the population without pneumonia, while the group with pneumonia but without thrombocytopenia had a 3.02% (P < 0.0088; 95% CI: 0.88-5.16%) higher mortality rate than the group without pneumonia but with thrombocytopenia (Table 4).
Discussion
The purpose of this study was to determine if comorbid pneumonia and thrombocytopenia are associated with poor outcomes in hospitalized patients. Previous studies have demonstrated that hospital-acquired and ventilator-associated pneumonia are major risk factors for mortality in settings such as the ICU and found that approximately one out of three patients hospitalized with community-acquired pneumonia died within one year [1, 14]. Other studies have indicated that thrombocytopenia is linked to adverse outcomes in patients with community-acquired pneumonia and that rising platelet counts are indicators of increased survival while falling platelet counts are prognostic of poor outcomes [11, 15]. Our results indicate that patients with concurrent pneumonia and thrombocytopenia have a higher mortality rate than those diagnosed with pneumonia without thrombocytopenia and those with thrombocytopenia without pneumonia. This association may be related to the role of platelets in immunity. While platelets are well-known for their role in coagulation, they also play an important role in aiding immunity during infection. During an infection, inflammatory cytokines and chemokines induce platelet activation. Platelets then release granules containing immunoregulatory proteins that can halt pathogen proliferation and even destroy some pathogens [8, 16-18]. Given the role of platelets in immunity, worse outcomes could be expected in patients diagnosed with comorbid pneumonia and thrombocytopenia.
Our results also indicated that patients with pneumonia but without thrombocytopenia had a significantly higher mortality rate compared to patients with thrombocytopenia but without pneumonia; however, the difference was found to be as low as 0.88%, as indicated by the confidence interval. Compared to the much larger significant differences found between the other comparison groups, this small difference may indicate that thrombocytopenia on its own may also be associated with inpatient mortality.
Our results suggest that thrombocytopenia has the potential to be an indicator of mortality risk in patients admitted with pneumonia in rural populations in Southwest Missouri. Identifying risk factors for poor outcomes in patients with pneumonia can inform providers of the level of intervention needed for these patients. This information can also assist both patients and their families in making decisions about life-saving versus supportive care in cases of severe pneumonia. The association found between thrombocytopenia, pneumonia, and poor outcomes may also indicate that those with thrombocytopenia have an increased risk of mortality when contracting pneumonia compared to the general population, suggesting a need to increase pneumonia prevention efforts in certain high-risk populations. Prevention efforts could emphasize pneumococcal vaccination or increased avoidance of exposure in immunosuppressed populations.
In addition to thrombocytopenia being a potential indicator of mortality risk in patients with pneumonia, thrombocytopenia on its own may be an ominous finding, as the mortality rate of thrombocytopenia without pneumonia was only slightly higher than that of pneumonia without thrombocytopenia. These findings are interesting, as pneumonia is historically considered a more severe disease. However, in ICU patients, thrombocytopenia has been found to be an independent variable for risk stratification, with platelet counts lower than 150,000 indicating increased mortality [19]. Another study analyzed the association between platelet counts and mortality in critically ill patients with tumors and found that both thrombocytopenia and thrombocytosis were associated with higher mortality rates [20]. These studies suggest that platelet levels may be associated with a worse prognosis in critically ill patients.
Limitations
The generalizability of our study is limited to people in rural communities in Southwest Missouri with pneumonia severe enough to require hospital admission. Currently, it is unclear whether the data linking thrombocytopenia to poor outcomes in patients with pneumonia can be applied to other geographic locations or to patients with pneumonia who are not admitted to the hospital.
Other important limitations of this study include potential bias and errors of imprecision. As this is a retrospective study, the population was not randomized, which may skew the magnitude of the results in a positive direction. Without the ability to randomize subjects, this data may not be representative of the population as a whole. Given the retrospective design, all variables were determined prior to initiating the study. Since the data were already reported, a lack of standardization could be a concern. The lack of standardized reporting makes the data vulnerable to errors, including underdiagnosed pneumonia, misdiagnosis of pneumonia, and possible lab errors indicating thrombocytopenia. Underdiagnosing pneumonia may negatively skew results, while misdiagnosis of pneumonia or lab error indicating thrombocytopenia could positively skew our results. A generalized lack of standardization for cutoff values of thrombocytopenia may also impact our results. Confounding factors, including age, gender, comorbid conditions, and disease severity, may also contribute to bias in this study, affecting the determination of pneumonia and thrombocytopenia as independent risk factors for mortality.
Given the retrospective study design, we cannot determine whether thrombocytopenia occurred before or after pneumonia. Information regarding temporality would more accurately inform the care of those with preexisting thrombocytopenia. The current data limits our ability to determine whether thrombocytopenia played a role in decreased immunity, possibly leading to pneumonia, or if thrombocytopenia occurred as a result of pneumonia. Understanding this cause-and-effect relationship could allow for more accurate guidance of treatments. If thrombocytopenia increases the risk of poor outcomes in pneumonia, then medical intervention to increase platelet counts could improve the disease course. However, if thrombocytopenia occurs as a result of the severity of pneumonia, it may indicate an ominous prediction regarding immune system function.
Another consideration is the type of pneumonia and the relative risk associated with thrombocytopenia. The methodology for this study used ICD-10 codes for several different types of pneumonia, including both bacterial and viral. Some evidence indicates a stronger role for platelets in the antibacterial immune response compared to the antiviral immune response [8]. Therefore, thrombocytopenia may increase the risk of mortality associated with bacterial infections compared to viral infections. The results of this study could be positively skewed based on the prevalence of bacterial versus viral pneumonia.
Recommendations
While our research indicates a link between thrombocytopenia and pneumonia, more research is needed to determine the specific role of decreased platelets in increased mortality. Future research may include studies examining the potential cause-and-effect relationship between the two diagnoses and how this relationship may pertain to those with preexisting thrombocytopenia. Confounding factors such as age, gender, comorbid disease, and severity of the conditions should also be explored as variables. Future evidence regarding the role of platelets in pneumonia-associated mortality can help inform healthcare providers as they determine the clinical course and medical interventions for their patients.
Conclusions
With pneumonia being one of the most common causes of hospital admission and a significant risk to many populations, studying its outcomes and comorbidities is critical for treatment planning and mitigation. Our study indicates that the risk of poor outcomes is significantly higher in patients with pneumonia and comorbid thrombocytopenia compared to those diagnosed with pneumonia or thrombocytopenia alone. Interestingly, pneumonia without thrombocytopenia shows only a minimal increase in mortality compared to thrombocytopenia without pneumonia, demonstrating a potential link between platelet counts and patient mortality. Further studies are needed to investigate the cause-and-effect relationship between pneumonia and thrombocytopenia, which could further assist in treatment management. Additionally, larger and more varied populations should be studied to increase generalizability.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adults hospitalized with pneumonia in the United States: incidence, epidemiology, and mortality Clin Infect Dis Ramirez JA Wiemken TL Peyrani P 180618126520172902016410.1093/cid/cix 647 · doi ↗ · pubmed ↗
- 2National Center for Health Statistics. Pneumonia. Atlanta, GA: Centers for Disease Control and Prevention; Fast Stats 1 2024 2023 https://www.cdc.gov/nchs/fastats/pneumonia.htm
- 3Burden of community-acquired pneumonia in North American adults Postgrad Med File TM Jr Marrie TJ 13014112220102020346410.3810/pgm.2010.03.2130 · doi ↗ · pubmed ↗
- 4The annual economic burden among patients hospitalized for community-acquired pneumonia (CAP): a retrospective US cohort study Curr Med Res Opin Divino V Schranz J Early M Shah H Jiang M De Koven M 1511603620203156600510.1080/03007995.2019.1675149 · doi ↗ · pubmed ↗
- 5Readmission following hospitalization for pneumonia: the impact of pneumonia type and its implication for hospitals Clin Infect Dis Shorr AF Zilberberg MD Reichley R 3623675720132367787210.1093/cid/cit 254 · doi ↗ · pubmed ↗
- 6Community-acquired pneumonia Lancet Aliberti S Dela Cruz CS Amati F Sotgiu G Restrepo MI 90691939820213448157010.1016/S 0140-6736(21)00630-9 · doi ↗ · pubmed ↗
- 7Thrombocytopenia in critically ill patients receiving thromboprophylaxis: frequency, risk factors, and outcomes Chest Williamson DR Albert M Heels-Ansdell D 1207121514420132378828710.1378/chest.13-0121 · doi ↗ · pubmed ↗
- 8What function do platelets play in inflammation and bacterial and viral infections?Front Immunol Tokarz-Deptuła B Palma J BaranieckiŁ Stosik M Kołacz R Deptuła W 7704361220213497026010.3389/fimmu.2021.770436 PMC 8713818 · doi ↗ · pubmed ↗