Relevance of Mediterranean diet as a nutritional strategy in diminishing COVID-19 risk: A systematic review
Ceria Halim, Miranda Howen, Athirah Amirah Nabilah binti Fitrisubroto, Timotius Pratama, Indah Ramadhani Harahap, Lacman Jaya Ganesh, Andre Marolop Pangihutan Siahaan, Nour Amin Elsahoryi, Nour Amin Elsahoryi, Nour Amin Elsahoryi

TL;DR
This review explores how following a Mediterranean diet may help reduce the risk of getting COVID-19, but its effects on symptoms and severity are unclear.
Contribution
The study systematically reviews the link between Mediterranean diet adherence and outcomes of COVID-19 in humans.
Findings
Four studies found a significant correlation between higher Mediterranean diet adherence and reduced risk of COVID-19.
One study reported a significant association between the diet and reduced severity of the disease.
Results on symptoms were mixed, with three studies finding no significant association.
Abstract
Mediterranean Diet has been reported to possess immunomodulatory and anti-inflammatory properties. These properties are closely associated with the immunopathogenesis of COVID-19. The present systematic review aimed to determine the association between Mediterranean Diet and COVID-19, COVID-19 symptoms, and COVID-19 severity. The protocol for this systematic review was registered in International Prospective Register of Systematic Reviews (PROSPERO) with identification number CRD42023451794. The literature search was conducted through Pubmed, Proquest, and Google Scholar on August 2023. The inclusion criteria were studies with a population of human subjects, reported the association between Mediterranean diet adherence with risk of COVID-19 infection, COVID-19 symptoms, or COVID-19 severity, and full text must be available in English. The exclusion criteria were reviews, editorials,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
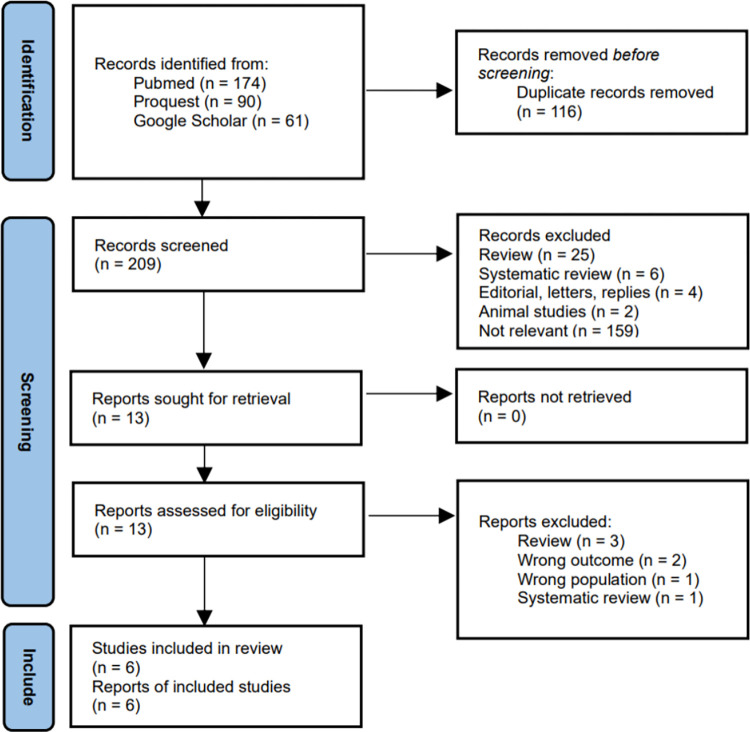 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutritional Studies and Diet · Child Nutrition and Water Access · Consumer Attitudes and Food Labeling
Introduction
The coronavirus disease 2019 (COVID-19) was declared as a pandemic in March 2020 and had a widespread impact on individuals across the globe, with total infection cases reaching more than 775 million in 4 years [1, 2]. Studies have reported main symptoms of COVID-19 including fever, cough, and shortness of breath. Other non-specific symptoms were also reported among COVID-19 patients, such as sore throat, nasal congestion, and shortness of breath. In addition to the typical respiratory symptoms, COVID-19 has also been associated with a range of atypical manifestation, such as headache, diarrhea, nausea, and vomiting [3]. The World Health Organization (WHO) has classified COVID-19 disease severity into four groups: mild, moderate, severe, or critical. This classification was based on a combination of symptoms, oxygen saturation, and inflammatory biomarkers [3]. COVID-19 severity largely played a role in COVID-19 mortality, as reflected from recent data that reported COVID-19 mortality ranged from 6.3% in average population [4], to 13.2% in inpatient population, and drastically increased to 55.9% in patients requiring mechanical ventilation [5]. Until this article was written, more than 7 million total deaths by COVID-19 were recorded [2].
Inflammation has been widely recognized as a critical factor in the development and the degree of severity in COVID-19. After the initial innate immune response, a potent uncontrolled inflammatory response called cytokine storm may follow. Cytokine storm, characterized by excessive inflammation caused by high levels of cytokines, particularly IL-6, IL-1, and TNF-α, can lead to advanced disease, multiorgan involvement, and serious consequences [6]. Cytokine storm has been identified as a potential target for therapeutic interventions, and multiple approaches. Immunomodulatory drugs, including dexamethasone and tocilizumab, as well as exosomes generated from mesenchymal stem cells and plasmapheresis, have been employed as ways to regulate this hyperinflammatory response [7]. These studies were just a few out of others that cemented the important role of inflammation in COVID-19.
The Mediterranean diet is a dietary pattern that consists primarily of plant-derived nutritional components, such as fruits, vegetables, legumes, nuts, and olive oil, and has been linked to anti-inflammatory properties and a reduced likelihood of developing cardiovascular disease [8]. Mediterranean diet is rich sources of polyphenols and polyunsaturated fatty acids (PUFAs), which are well-known antioxidants [9]. Adherence to Mediterranean diet has been reported to lower the expression of pro-inflammatory molecules, such as TNF-α, IL-1, IL-6 and CRP, as well as a reduction in the overall systemic inflammatory status, while also exerting antiviral effects by decreasing nuclear transcription factor kappa B (NF-κB) expression [10–12]. Mediterranean diet has been reported to benefit those with various disorders associated with persistent low-grade inflammation [10]. Researchers had suggested the potential association between diet and viral infections [13]. Fruits and fish oil, both vital components of Mediterranean diet, contain vitamin A, C, and D. These vitamins are effective antioxidant against reactive oxygen species (ROS) which are secreted by immune cells and help maintain body cells integrity, while also supporting epithelial barriers integrity. Vitamin D, which stimulate polymorphonuclear (PMN) and natural killer cells (NK) cells in producing potent anti-microbial peptides. The resulting effect are decreased risk of infection and increased viral clearance [13]. This has led to the growing proposition of the protective effects of Mediterranean diet towards COVID-19 [9, 11].
Based on the properties of Mediterranean diet that have been described above, this systematic review aims to address the association between Mediterranean diet and COVID-19 risk, COVID-19 symptoms, and COVID-19 severity.
Materials and methods
Protocol writing and registration
The protocol for this systematic review was registered on 15^th^ September 2023 with the International Prospective Register of Systematic Reviews (PROSPERO) with identification number CRD42023451794. This systematic review was reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [14].
Search strategy
Literature search was conducted on 3 search engines, Pubmed, Proquest and Google Scholar, on 16th August 2023. Literature search was done using the keyword "Mediterranean diet and COVID-19", with detailed search strategy and medical subject headings (MeSH) described below (S1 File). No additional article or abstract was selected from other sources.
Study selection
The inclusion criteria for this systematic review were studies with a population of human subjects, and reported the association between Mediterranean diet adherence with COVID-19 infection, COVID-19 symptoms, or severe COVID-19. No study design nor publication date restriction were applied. Full-text must be available in English. The exclusion criteria were reviews, editorials, letters, replies, systematic reviews, meta-analyses, studies on animals, and duplicates.
Deduplication was carried out using the Rayyan application [15]. The remaining articles were screened based on title and abstract manually by two reviewers working individually. No automation tool was used in the process. Each article would be sought for further review if at least one reviewer considered it to fulfill the criteria and was within the scope of this systematic review. Studies that passed the initial screening would be sought for retrieval. Two reviewers working together further reviewed the full-text of each literature for its eligibility.
Data extraction
Data were collected by two reviewers working separately using data collection standards set previously. This included name of the first author, year of publication, study location, study design, total and characteristics of participants. Mediterranean diet association with COVID-19 infection, symptoms, and severity, Mediterranean diet adherence and outcome definition were also recorded. All results that were compatible with each outcome domain in each study were sought. Missing data were not sought further.
Quality assessment
Non-randomized studies were assessed using Newcastle-Ottawa Scale (NOS) [16]. NOS criteria in cross-sectional studies were adapted from cohort criteria [17]. The NOS criteria were scored based on three categories: selection, comparability, and outcome, with each category consisted of 1–4 items. NOS score ranged from 0 (lowest quality) to 9 (highest quality). Randomized studies were assessed using revised Cochrane risk of bias tool for randomized trials (RoB2) [18]. Each successfully retrieved full-text article will be evaluated and scored by two reviewers working independently. Disagreement between reviewers’ judgement was resolved by soliciting a third reviewer’s opinion.
Data synthesis
Data was synthesized narratively. The minimum number of studies was two for each analysis. The outcome was measured with odds ratio (OR) for COVID-19 infection, symptoms, and severity. Study characteristics, risk of bias, and study findings, and other relevant data were reported and tabulated. Similarities, differences, strengths, and limitations were compared across studies. A structured summary was also presented, to further elaborate the extracted data [19]. No subgroup nor sensitivity analyses were carried out.
Reporting bias and certainty assessment
Reporting bias was evaluated using a tool by Page et al. [20] and RoBANS 2: A Revised Risk of Bias Assessment Tool for Nonrandomized Studies of Interventions [21]. We used the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach to define the certainty in the body of evidence [22].
Results
Literature search
A total of 325 records were identified across Pubmed, Proquest and Google Scholar. Duplicates were removed, with 209 records remained and screened. Thirteen articles were sought for retrieval and were further reviewed for eligibility. Six articles were deemed eligible and were included in this systematic review. A flow chart of selection process and exclusion reasons is provided below (Fig 1).
Article selection process flow diagram.
The study by Mohajeri et al. [23] appear to meet the inclusion criteria, but were excluded, as the outcome of COVID-19, COVID-19 symptoms, or COVID-19 severity were not reported. The study only reported outcome of inflammatory biomarkers.
Study characteristics
All 6 articles were observational studies, published in 2020–2023 [24–29]. The total sample was 55,489 patients, with study location across 5 countries. The majority of the studies had a prospective cohort design. Five studies reported the association between Mediterranean diet adherence and COVID-19 infection, four reported the association between Mediterranean diet adherence and COVID-19 symptoms, and three reported the association between Mediterranean diet adherence and severe COVID-19.
All studies measured the Mediterranean diet adherence using questionnaires, with scoring system varying between study to study. All Mediterranean diet adherence included categories such as, vegetables, fruits and nuts, cereals, legumes, fish, red meat, dairy, and alcohol consumption. Monounsaturated to saturated fat ratio was also an essential component in Mediterranean diet score, although four studies replaced monounsaturated fat to saturated fat ratio with olive oil intake [24–27]. The reason behind this was that the ratio of monounsaturated to saturated fats does not correspond to a specific food and the fact that olive oil is also the main source of monounsaturated fats in the traditional Mediterranean diet [25]. Newcastle Ottawa Scale (NOS), used to assess risk of bias was presented along the study characteristics in Table 1.
Table 1: Study characteristics.
Mediterranean diet and COVID-19
A total of five studies investigated the association between Mediterranean diet adherence and COVID-19 [24–28] with a sample size of 55,239 patients as listed in Table 2. Three studies analyzed Mediterranean diet adherence as continuous variable of 1-point increment, one study analyzed Mediterranean diet adherence as categorical variable in a cut-off determined by the respective study, and one study analyzed Mediterranean diet adherence as both categorical variable in quartiles and continuous variable of 1-SD increment. Four studies relied on self-report of previous history of COVID-19 to determine COVID-19 cases, while one study relied on both serologic testing and self-report.
Table 2: Mediterranean diet and COVID-19.
Three out of five studies reported Mediterranean diet adherence significantly lower risk of COVID-19, while two studies stated non-significant results. All five studies reported OR ranging between 0.75–0.948. The study by El Khoury et al., [24] reported the OR of being non infected by COVID-19 (OR = 1.055, 95%CI: 1.013–1.099, p = 0.01). This data was then inverted to properly reflect the odds of COVID-19 as noted in Table 2. Three studies adjusted for potential confounding variables. Three studies analyzed the association of Mediterranean diet individual components with COVID-19 risk. Among the food categories, higher olive oil consumption, lower red meat consumption, lower cereal consumption, moderate amounts of alcohol, and higher intake of fruit and nuts were reported to lower risk against COVID-19.
Mediterranean diet and COVID-19 symptoms
Four studies reported the association between Mediterranean diet adherence and COVID-19 symptoms [24, 25, 28, 29] with a sum of 53,069 patients. Differing comparison of Mediterranean diet adherence score was reported across studies with one each of, continuous variable of 1-point increment, categorical variable in a cut-off determined by the authors of the study, categorical variable in tertiles, and as both categorical variable in quartiles and continuous variable of 1-SD increment, as detailed in Table 3. All studies depended on self-report for the presence of COVID-19 symptoms, and analyzed the odds ratio using logistic regression with yes/no type outcome. Two studies analyzed for symptomatic COVID-19 outcome [25, 28], one study for moderate COVID-19 burden (defined as presence of 5–10 symptoms) [24], and one study analyzed for each COVID-19 symptom [29].
Table 3: Mediterranean diet and COVID-19 symptoms.
The study by Zargarzadeh et al. [29] found that higher Mediterranean diet adherence significantly decrease the odds for all reported COVID-19 symptoms, with OR varied between 0.06–0.34 for each symptom. Three studies reported insignificant association, with OR of each study ranging between 0.84–0.992, and p value >0.05, although the result from Yue et al. [28] did reach the limit of statistical significance (OR = 0.89, 95% CI: 0.80–0.99; P-trend = 0.0549). Perez-Araluce et al. analyzed the relation of individual components of Mediterranean diet with COVID-19 symptoms, yet no food categories were found to be significant [25].
Mediterranean diet and COVID-19 severity
The association between Mediterranean diet adherence and COVID-19 severity were analyzed in three observational studies [25, 28, 29], as listed in Table 4. The total sample was 52,670 patients, relatively similar with the previous two outcomes. Self-report of hospitalization due to COVID-19 was the main method to determine severe COVID-19 cases. One study examined the medical records of the participants for severe COVID-19, in accordance with the National Institute of Health’s Coronavirus Disease 2019 (COVID 19) Treatment Guidelines.
Table 4: Mediterranean diet and COVID-19 severity.
The study by Zargarzadeh et al. [29] found that participants with top tertile Mediterranean diet score were less likely to have severe COVID-19 (OR = 0.23; 95% CI: 0.11–0.50, P <0.001) than the bottom tertile. Two studies reported insignificant association with OR ranging 0.22–0.89, and p value > 0.05. Two studies analyzed the effects of Mediterranean diet individual components against COVID-19 severity. One study found no individual components were significant, while the study by Zargarzadeh et al. [29] reported higher consumption of vegetables, fruits, legumes, nuts, whole grains, and fish lower odds of severe COVID-19.
Reporting bias and evidence grading
Using the tool by Page et al. [20] and RoBANS 2 [21] for evaluating reporting bias, we considered the included studies were of low-to-moderate risk for reporting bias. A detailed assessment is attached (S2 File). To grade the quality of evidence, the tool Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) was used. On the outcome of COVID-19 risk, the authors considered the overall grading of the evidence to be of moderate certainty, meaning the true effect is probably close to the estimated effect. This was primarily because of the large number of patients for the outcome analyzed, similar effect estimates trend between studies (all outcome analyses reported OR <1), and adjustment for multiple confounding factors. For the outcome of COVID-19 symptoms and COVID-19 severity, we rated the evidence to be of low certainty, meaning the true effect might be markedly different from the estimated effect. Certainty for these outcomes was rated down for imprecision and that there were too few available studies included in the analyses.
Discussion
The protective mechanism of diet against viral respiratory disease progression has been acknowledged by several studies. A previous study found that healthy plant-based foods was associated with lower odds and severity of COVID-19 [30]. Another relevant finding was that the adoption of a Traditional Mediterranean Diet contributed towards to the improvement of patients with recurring colds and frequent inflammatory complications, with significantly reduced episodes and symptoms [31]. A previous systematic review found that Mediterranean diet was reported to lower inflammatory biomarker levels in obese/overweight adults [32]. Similarly, a precedent meta-analysis reported Mediterranean diet adherence effectively reduce SARS-CoV-2 infection by 78% (95% CI 69%–88%), although the authors recommended cautious interpretation due to the paucity of the included studies [33].
These previous studies were in line with our findings. For the outcome of COVID-19, interestingly, all studies reported OR<1, although there were differing reports on the significance of this association. Another interesting thing to note was the studies that didn’t adjust for confounding factors reported significant association, while two studies that adjusted for confounding factors reported non-significant association. An exception to this was the study with the largest number of participants. The study by Yue et al. [24] adjusted for multiple confounding factors and reported higher Mediterranean diet adherence proved to be significant in lowering odds of COVID-19. These results indicated that higher Mediterranean diet adherence was a protective factor against COVID-19, although the magnitude of the effect estimate was probably minor and thus was only observable in a larger population.
For the outcomes of COVID-19 symptoms and severity, all studies were adjusted for confounding variables, and almost all studies recorded non-significant association. Only the study by Zargarzadeh et al. [29] reported significant association for both outcomes. These differences could be explained by a few reasons. First, the study had a cross-sectional design, and as stated by its authors, the results cannot infer a causative association. In addition, although the study scored a high NOS score, this score was obtained by using a form adapted for cross-sectional study, and may not be comparable to the NOS from cohort studies. It bears mentioning that, despite the difference in significance, the effect estimates for both COVID-19 symptoms and severity outcomes across all studies showed a consistent trend of OR <1. It was necessary to put into consideration that the consistent effect of Mediterranean diet adherence in all studies may be more critical than the statistically insignificant p-value [34]. In fact, a nonsignificant result does not mean that there is no effect [34], albeit it might be too presumptive to assume a protective effect of higher Mediterranean diet adherence against COVID-19 symptoms and severity without conclusive evidence. Although a meta-analysis could produce a higher statistical power for this purpose, there were a few considerations as to why it was not performed. Multiple assessment index for Mediterranean diet adherence were used between studies. In addition, most studies assigned points for Mediterranean diet adherence depending on sex-specific median consumption in the respective study. Hence, we deemed a meta-analysis was not appropriate for the diverse data.
Several subtypes of food were inversely associated with COVID-19 risk. Higher olive oil consumption, lower red meat consumption, lower cereal consumption, moderate amounts of alcohol, and higher intake of fruit and nuts reduced COVID-19 risk, and higher consumption of vegetables, fruits, legumes, nuts, whole grains, and fish lowered odds of severe COVID-19. The presence of flavonoids, an antiviral and immunostimulatory compounds, linked fruit consumption to a reduced risk of SARS-CoV-2 infection [35]. Vitamin C, a major vitamin in fruits and vegetables, took part in inhibiting NLRP3 inflammasome pathway, decreasing pro-inflammatory cytokines, and improving neutrophil chemotaxis [35, 36]. These resulted in minimizing viral pathogenesis, enhancing recovery, while also preventing respiratory viral infection [36, 37]. Olive oil and fish were excellent sources of monounsaturated fatty acids (MUFAs) and polyunsaturated fatty acids (PUFAs), which had been known to exhibit immunomodulatory properties [38]. Docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) bind to peroxisome proliferator-activated receptors (PPARs), inhibiting cytokine expression by NF-κB inflammatory transcription factor [38]. Other pathways include decreasing lipid rafts and augmenting major histocompatibility complex 1 (MHC 1) expression [38]. In addition, virgin olive oil contained phenolic compounds, such as oleocanthal, that exerted potent anti-inflammatory actions, similar to ibuprofen [39]. Likewise, legumes possess bioactive compounds, such as peptides, polyphenols and saponins, which showed anti-inflammatory activity, inhibiting cyclooxygenase-1 (COX-1) and cyclooxygenase-1 (COX-2) enzyme expression [40]. Red wine, a prevalent alcoholic drink in Mediterranean diet, contains many types of antioxidants which neutralize free oxygen radicals released by neutrophils, minimizing cellular damage [41]. The overall beneficial anti-inflammatory properties of these food groups explained their effects in diminishing risk of COVID-19 and severe COVID-19.
Strengths and limitations
We further reviewed the strengths and limitations of each study, as listed in Table 5. The study by Sharma et al. used objective serology data coupled with self-reported data to define COVID-19 cases [27]. The study by Yue et al. had a large number of participants, and all participants were health professionals which ensured high-quality health information [28]. Most of the studies included were adjusted for multiple confounding variables.
Table 5: Strengths and limitations of each study.
The major limitation was that Mediterranean diet adherence of all studies was self-reported. Measurement errors in FFQs are known to affect results of studies and may have biased the observed effect estimates. FFQs were prone to biased responses, such as recall and estimation bias. However, FFQs were often used in large cohort studies because it is realistic and is logistically feasible. Two of the studies stated they had inadequate cases for observed outcome to produce a significant result [27, 28].
To our knowledge, this systematic review is the first to specifically investigate the relationship between Mediterranean diet and COVID-19 risk, symptoms, and severity. Additionally, each of the study selection and bias assessment process was conducted by multiple reviewers to ensure minimal bias. This was done in accordance with the Cochrane guidelines [42].
This systematic review has some limitations that should be considered when interpreting the results. First, there were few studies included in this systematic review. Second, as a meta-analysis is not performed, the magnitude of the effects could not be precisely measured.
Public health implications
This systematic review provides an up-to-date summary of the available evidence. As more and more countries have loosened on personal protective equipment (PPE) and social distancing regulations, a nutritional strategy may be more feasible and beneficial long-term. The results of the present study may shed some light on additional benefits of Mediterranean diet against COVID-19. The findings also suggest that specific food groups in the Mediterranean diet may be more important in reducing COVID-19 odds. More studies should be conducted before definitive conclusions can be drawn.
Conclusion
Overall, the analyses suggest higher Mediterranean diet adherence significantly reduced odds of COVID-19, with non-significant results against COVID-19 symptoms and severity.
Supporting information
S1 ChecklistPRISMA 2020 abstract checklist.(DOCX)
S2 ChecklistPRISMA 2020 main checklist.(DOCX)
S1 FileDetailed search strategies and MeSH.(DOCX)
S2 FileReporting bias risk assessment.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Rolling updates on coronavirus disease (COVID-19) [Internet]. [Updated 2020 Jul 31; cited 2023 Oct 16]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen
- 2World Health Organization. WHO COVID-19 dashboard [Internet]. Updated 7 July 2024; cited 17 July 2024]. Available from: https://data.who.int/dashboards/covid 19/
- 3Clinical management of COVID-19: Living guideline [Internet]. Geneva: World Health Organization; 2022 Jun 23-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 582435/35917394 · pubmed ↗
- 4Sousa GJB, Garces TS, Cestari VRF, Florêncio RS, Moreira TMM, Pereira MLD. Mortality and survival of COVID-19. Epidemiol Infect. 2020 Jun 25;148:e 123. doi: 10.1017/S 0950268820001405 ; PMCID: PMC 7330281.32580809 PMC 7330281 · doi ↗ · pubmed ↗
- 5Isath A, Malik AH, Goel A, Gupta R, Shrivastav R, Bandyopadhyay D. Nationwide Analysis of the Outcomes and Mortality of Hospitalized COVID-19 Patients. Curr Probl Cardiol. 2023 Feb;48(2):101440. doi: 10.1016/j.cpcardiol.2022.101440 Epub 2022 Oct 8. ; PMCID: PMC 9546497.36216202 PMC 9546497 · doi ↗ · pubmed ↗
- 6Manjili RH, Zarei M, Habibi M, Manjili MH. COVID-19 as an Acute Inflammatory Disease. J Immunol. 2020 Jul 1;205(1):12–19. doi: 10.4049/jimmunol.2000413 Epub 2020 May 18. ; PMCID: PMC 7333792.32423917 PMC 7333792 · doi ↗ · pubmed ↗
- 7Mathur P, Kottilil S. Immunomodulatory therapies for COVID-19. Front Med (Lausanne). 2022 Aug 3;9:921452. doi: 10.3389/fmed.2022.921452 ; PMCID: PMC 9381694.35991665 PMC 9381694 · doi ↗ · pubmed ↗
- 8Estruch R, Ros E, Salas-SalvadóJ, Covas MI, Corella D, Arós F, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N Engl J Med. 2018 Jun 21;378(25):e 34. doi: 10.1056/NEJ Moa 1800389 Epub 2018 Jun 13. .29897866 · doi ↗ · pubmed ↗