Swift Onset, Swift Recovery: Unusual Nonrheumatic Myocarditis in a Young Adult Post Group A Streptococcal Pharyngitis
Andres Rios, Colby Wood, Ricardo Isaiah Garcia, Emily C. Mitchell, Jacob Nichols

TL;DR
A young adult developed and recovered quickly from nonrheumatic myocarditis after a strep throat infection, highlighting the need for prompt diagnosis and treatment.
Contribution
This case report presents an atypical and rapid-onset nonrheumatic myocarditis case in a young adult post-strep throat.
Findings
Nonrheumatic myocarditis can occur rapidly in young adults following Group A streptococcal pharyngitis.
Amoxicillin and anti-inflammatory therapy effectively managed the patient's symptoms.
Timely clinical intervention is crucial for atypical myocarditis presentations.
Abstract
This case report highlights the unusual presentation and management of nonrheumatic myocarditis in a 24-year-old male, an age demographic not commonly associated with myocardial complications following Group A streptococcal pharyngitis. The patient, devoid of any prior medical history, manifested symptoms one day after being diagnosed with Group A streptococcal pharyngitis, a stark contrast to the typical progression of myocardial complications. The swift onset of symptoms and the patient's subsequent clinical presentation necessitated a comprehensive diagnostic approach. The patient's symptoms were successfully alleviated with amoxicillin and anti-inflammatory therapy, underscoring its potential efficacy in managing nonrheumatic myocarditis. This case serves as a poignant reminder of the importance of maintaining a broad differential diagnosis, especially in atypical presentations, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
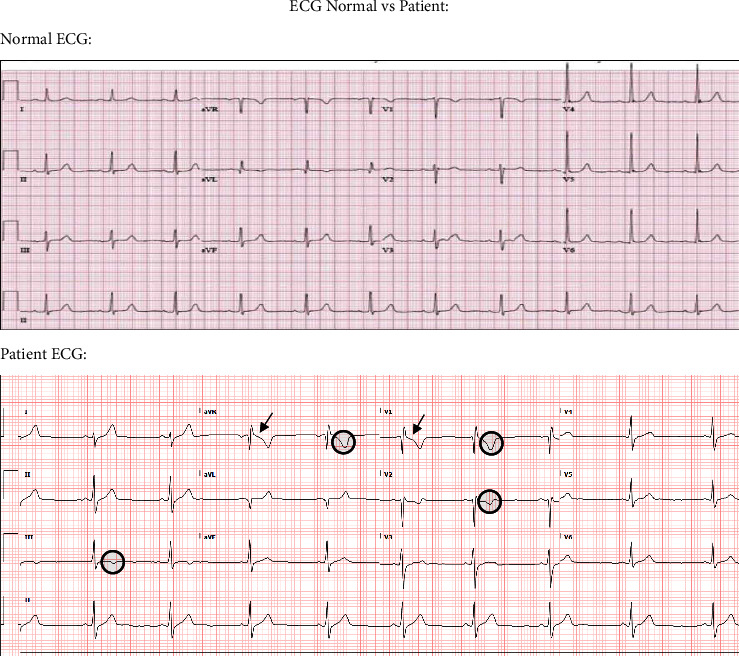 Figure 1
Figure 1- —Texas Tech University Health Sciences Center
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Immunology Research · Streptococcal Infections and Treatments · Infective Endocarditis Diagnosis and Management
1. Introduction
Nonrheumatic myocarditis (NRM) is a distinct clinical entity that stands apart from the more commonly recognized acute rheumatic fever (ARF) [1]. Unlike ARF, which typically presents weeks after a Group A streptococcal (GAS) infection, NRM makes its appearance in a much shorter timeframe. This rapid onset of symptoms, coupled with its clinical manifestations, can often lead to diagnostic challenges [2]. ECG changes, particularly ST elevations, further complicate the clinical picture, making it imperative for clinicians to differentiate between an actual myocardial infarction and NRM [2]. The differentiation is crucial, as the management strategies for both conditions differ significantly. While the pathophysiology of ARF is better understood, involving molecular mimicry that triggers cross-reactive immune responses between host cardiac antigens and Streptococcus antigens, the pathophysiology of NRM is less understood and is thought to arise from direct invasion of the myocardium by the GAS organism or through a toxin-mediated mechanism [1, 3]. In contrast to a toxin-mediated pathophysiology, a recent article found that bacteria, neutrophilic infiltrate, and microabscesses were found on histological examination of a patient with recurrent myocarditis on autopsy [4]. Given these diverging conclusions, current literature on the pathophysiology of NRM is poorly understood and therefore further warrants future research to be done [5]. This difference in pathogenesis further underscores the need for a precise diagnosis.
While the immediate treatment might appear similar, the long-term management and follow-up vary [2]. Recent case reports generally indicate that treatment aimed at addressing Streptococcal infection also serves as the primary approach for nonrheumatic myocarditis, often resulting in resolution of symptoms within a few days to one week [6, 7]. This suggests that treatment typically includes antibiotics like penicillin, supplemented occasionally by supportive care such as rest, NSAIDs, and colchicine, which have been endorsed as beneficial management options [6, 8]. Additionally, the rarity of NRM in developed nations often leads to a lower index of suspicion among healthcare providers [2]. However, given the potential severity of the condition and its implications, a heightened awareness and understanding of NRM are essential. This case of a 24-year-old male emphasizes the importance of considering NRM in the differential diagnosis when young adults present with cardiac symptoms following a GAS infection [2].
2. Case Presentation
The patient is a 24-year-old male with no previous medical history who presented to an urgent care clinic with nonradiating central chest pain onset of a few hours. One day prior, the patient was evaluated at a family medicine clinic for a sore throat where rapid antigen testing was positive for GAS pharyngitis for which he was prescribed amoxicillin 500 mg PO q12 h for 10 days. Vitals at that time were significant only for tachycardia with a heart rate of 116 beats per minute. On arrival to the urgent care, an ECG was performed showing sinus bradycardia with T wave inversions in leads III, aVR, V1, and V2 and ST depressions in leads aVR and V1 can be seen in Figure 1. Subsequently, the patient was escorted to the emergency room (ER) for further evaluation.
In the ER, vital signs again revealed bradycardia, but were otherwise unremarkable. Patient received a one-time dose of aspirin 324 mg PO. Labs were obtained and pertinent results are present in Table 1.
Due to the elevated troponin T value, the patient was started on a heparin drip and cardiology was consulted. Based on their evaluation, it was felt that the patient most likely had myocarditis and less likely acute coronary syndrome. A transthoracic echocardiogram was significant only for trace tricuspid and mitral regurgitation. Additionally, Cardiology reported that ECGs obtained during urgent care and ER could be a normal variant given that repeat ECGs continued to show the same findings. No ECG demonstrated any evidence of acute coronary syndrome.
The infectious diseases team was consulted for evaluation and treatment recommendations as well. Based on their evaluation and timing of chest pain just one day after the diagnosis of streptococcal pharyngitis, it was felt that the patient was likely experiencing nonrheumatic myocarditis rather than acute rheumatic fever, although concurrent viral myocarditis was thought to be a possibility. The patient was initially treated with penicillin G IV 24 MU q24 h for GAS coverage and clindamycin 600 mg PO q12 h to decrease toxin production. Serological studies were ordered for adenovirus, CMV, EBV, echovirus (9, 11, 30), HHV 6 and 8, parvovirus B19, and a respiratory viral panel by PCR. Given clinical improvement over the following two days, the patient was prescribed indomethacin 25 mg TID, colchicine 0.6 mg BID, and amoxicillin 875 mg BID for 5, 7, and 10 days, respectively.
At follow up visits with family medicine and cardiology, symptoms had resolved completely. Echo viral 4, 7, 9, 11, and 30 antibodies were detected in serum during patient's admission into the hospital; however, subsequent convalescent titers were not performed given the patient's symptomatic improvement with antibiotics and anti-inflammatory medications. No long-term pharmacological prophylaxis was indicated at this time due to complete resolution of symptoms. Nonpharmacological treatments included rest and limited physical activity for a few months with slow return to baseline as tolerated. Prognosis included a return to baseline with no future complications. After a year of follow-up appointments, the patient was medically cleared and follow ups were no longer scheduled.
3. Discussion
This case brings forth several considerations in the clinical approach and management of NRM, especially in atypical presentations. The patient's experience underscores the importance of considering NRM and its complications in adult populations.
3.1. Diagnostic Distinctions between ARF and Nonrheumatic Myocarditis
The diagnostic criteria for ARF and NRM differ significantly, particularly in the context of a recent GAS infection. While ARF typically presents 2 to 3 weeks post-GAS infection, nonrheumatic myocarditis can manifest symptoms in a much shorter timeline [2]. Laboratory findings, such as elevated troponin levels, and specific EKG readings, including ST-segment elevation, are more indicative of nonrheumatic myocarditis [9]. In fact, a study found that cardiac troponin T (cTnT) levels typically remained within normal ranges in patients with acute rheumatic carditis, suggesting that cTnT might not be the most reliable diagnostic marker for ARF [10]. Conversely, other cases discussing the instance of nonrheumatic streptococcal myocarditis presented with progressively rising troponin levels [11, 12]. These distinctions are crucial in the diagnostic setting, as they guide clinicians in differentiating between these two conditions, which, although related to GAS infection, require different therapeutic approaches.
3.2. Underrepresentation in Young Individuals
One of the major defining factors in this case is the patient's age. The presentation in a 24-year-old male highlights the necessity for healthcare providers to maintain a high index of suspicion for GAS infection complications across a broader age range. Young individuals presenting with chest pain following a strep infection are often not immediately considered for nonrheumatic myocarditis. The prevailing clinical perception leans towards ARF, especially given its historical association with GAS infections [13]. However, nonrheumatic myocarditis can mimic STEMI presentations in young adults, emphasizing the need for heightened clinical suspicion [2].
3.3. The Imperative of Recognizing Nonrheumatic Myocarditis
Despite its rarity, NRM post-GAS infection should be a more prominent differential in patients presenting with the aforementioned symptoms. This case and multiple others emphasize the importance of distinguishing between ARF and NRM, especially given the potential cardiac complications associated with the latter [13–17]. A noteworthy point of mention is that titers were positive for echovirus 4, 7, 9, 11, and 30. These titers were deemed necessary to rule out their role on this patient. Nonetheless, successive titers were not performed due to the pathology resolution when treated with antibiotics and anti-inflammatories. Furthermore, there have been documented instances where nonrheumatic myocarditis poststreptococcal pharyngitis presented as acute ST-elevation myocardial infarction, further emphasizing the clinical significance of this differential [9, 11, 12, 18, 19]. Furthermore, a systematic review of 70 patient studies revealed that approximately half (47.1%) of the patients exhibited ST-segment elevations, with the majority showing other notable EKG abnormalities as well [20]. Interestingly, unlike those cases, which often exhibited ECG patterns resembling acute ST elevated myocardial infarctions, this particular case showed elevated troponin levels alongside a normal ECG reading (due to cardiologist normal variant findings). Therefore, while this case shares similarities with others involving NRM, it stands out due to its clinical presentation with a normal ECG reading.
4. Conclusion
In conclusion, while ARF remains a significant concern post-GAS infection, the potential for nonrheumatic myocarditis should not be overlooked, especially in young individuals presenting with chest pain. The diagnostic distinctions between these conditions, coupled with the underrepresentation of nonrheumatic myocarditis in clinical settings, underscore the importance of maintaining a broad differential diagnosis. As the literature suggests, a more inclusive approach can lead to timely and appropriate interventions, ultimately improving patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Silva R. Puga L. Teixeira R. Botelho A. Lourenço C. Gonçalves L. Acute non-rheumatic myopericarditis: a rare complication of pharyngitis European Journal of Case Reports in Internal Medicine 2018512 p. 110.12890/2018_000987 PMC 634697330755999 · doi ↗ · pubmed ↗
- 2Upadhyay G. A. Gainor J. F. Stamm L. M. Weinberg A. N. Dec G. W. Ruskin J. N. Acute nonrheumatic streptococcal myocarditis: STEMI mimic in young adults The American Journal of Medicine 2012125121230123310.1016/j.amjmed.2012.06.0162-s 2.0-8486922724523062402 · doi ↗ · pubmed ↗
- 3Benjanuwattra J. Juarez M. Rogers B. Jenkins L. A. Abstract 13153: non-rheumatic streptococcal myocarditis manifesting as acute non-ST-elevation myocardial infarction Circulation 2023148 Suppl_110.1161/circ.148.suppl_1.13153 · doi ↗
- 4Hiraiwa H. Morimoto R. Ando R. Recurrent fulminant non-rheumatic streptococcal myocarditis proven by endomyocardial biopsy and autopsy Journal of Cardiology Cases 2022261626510.1016/j.jccase.2022.02.00435923528 PMC 9214811 · doi ↗ · pubmed ↗
- 5Chatzantonis G. Meier C. Bietenbeck M. Surprising diagnosis in a patient with acute coronary syndrome: a case report of acute streptococcal pharyngitis-associated perimyocarditis European Heart Journal - Case Reports 2020421610.1093/ehjcr/ytaa 017PMC 718056432352068 · doi ↗ · pubmed ↗
- 6Mc Heik B. Ayach H. B. El Koubayati G. Non-rheumatic streptococcal acute myocarditis: the first documented sibling case Cureus 2024165 e 6099010.7759/cureus.60990 PMC 1119393738910751 · doi ↗ · pubmed ↗
- 7Baltzinger P. El Ghannudi S. Germaini M. Von Hunolstein J.-J. Zeyons F. Imperiale A. Recurrent non-rheumatic streptococcal myocarditis: 18F-FDG PET/CMR findings QJM: International Journal of Medicine 2024117645745910.1093/qjmed/hcae 02038273703 · doi ↗ · pubmed ↗
- 8Saeed S. Käsk L. Rajani R. Larsen T. H. Incidence, clinical presentation, and management of myocarditis following m RNA-based covid-19 vaccines: a brief report Cardiology 2022147440641210.1159/00052221635104821 PMC 9059023 · doi ↗ · pubmed ↗