Is the Prognostic Nutritional Index a Novel Prognostic Factor in Patients With Unresectable/Metastatic Gallbladder and Cholangiocarcinoma Receiving Chemotherapy?
İlknur Deliktaş Onur, Hatice Gülgün Fırat, Elif Sertesen Çamöz, Fatih Yildiz

TL;DR
This study explores whether the Prognostic Nutritional Index (PNI) can predict survival outcomes in patients with advanced gallbladder and bile duct cancers undergoing chemotherapy.
Contribution
The study demonstrates that PNI is a novel and independent prognostic factor for overall survival in patients with unresectable/metastatic gallbladder and cholangiocarcinoma.
Findings
Patients with a PNI below 44 had significantly shorter median survival (8.93 months) compared to those with PNI ≥ 44 (12.58 months).
PNI was found to be an independent predictor of overall survival in multivariate analysis.
PNI, along with ECOG performance status and CA 19.9, showed statistical significance in predicting survival outcomes.
Abstract
Gallbladder and biliary tract tumors are rare but highly fatal cancers. In patients diagnosed with unresectable/metastatic gallbladder cancer and cholangiocarcinomas, systemic chemotherapy is recommended if the patient's performance is good. Randomized studies on this subject are limited, and there is no standard treatment choice. The prognostic nutritional index (PNI) is a measurement calculated using albumin and absolute lymphocyte value, reflecting the immunological and nutritional status of the cancer patient. The aim of our study is to evaluate the prognostic effectiveness of PNI in unresectable/metastatic gallbladder and biliary tract cancers. The PNI was calculated using albumin and lymphocyte values at the time of diagnosis (10 x albumin g/dL + 0.005 x total lymphocyte/mm3). The relationship between PNI and overall survival (OS) and progression-free survival was examined. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
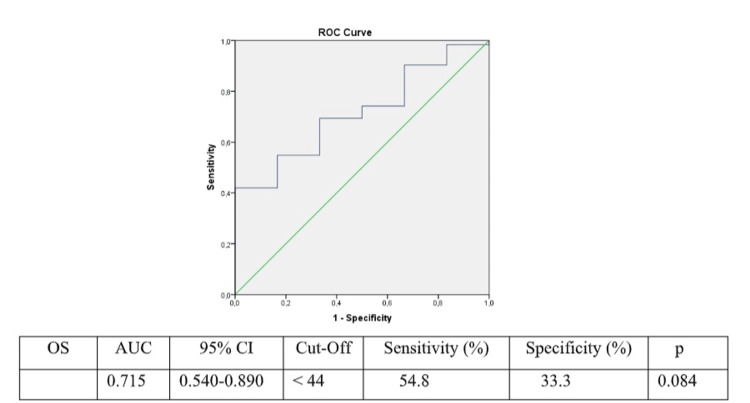 Figure 1
Figure 1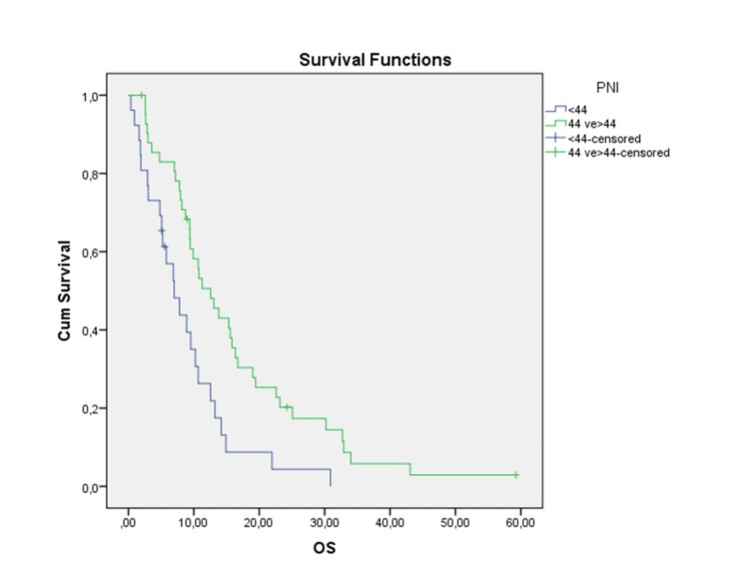 Figure 2
Figure 2| PNI < 44 (N: 26) | PNI ≥ 44 (N: 42) | P value | ||
| Age (median) (min-max) | 60 (95 % CI: 54-63) | 62 (95 % CI: 56-63) | ||
| Sex | ||||
| Female | 16 (39) | 25 (61) | 0.869 | |
| Male | 10 (37) | 17 (63) | ||
| Comorbidity | ||||
| Yes | 9 (28.1) | 23 (71.9) | 0.106 | |
| No | 17 (47.2) | 19 (52.8) | ||
| ECOG PS | ||||
| 0-1 | 12 (67.6) | 34 (73.9) | 0.003 | |
| ≥2 | 14 (63.6) | 8 (36.4) | ||
| Cholelithiasis History | ||||
| Yes | 3 (42.9) | 4 (57.1) | 0.790 | |
| No | 23 (37.7) | 38 (62.3) | ||
| Tumor Location | ||||
| Gall bladder | 13 (32.5) | 15 (53.6) | 0.245 | |
| Cholangiocarcinoma | 13 (46.4) | 27 (67.5) | ||
| Ca 19.9 | ||||
| <96 | 8 (26.6) | 22 (73.4) | 0.405 | |
| ≥ 96 | 11 (36.6) | 19 (63.4) | ||
| First Line Chemotherapy | ||||
| No | 4 (50.0) | 4 (50.0) | 0.499 | |
| Gemcitabine+Cisplatin | 12 (30.8) | 27 (69.2) | ||
| Gemcitabine | 4 (40.0) | 6 (60) | ||
| Capecitabine | 4 (57.1) | 3 (42.9) | ||
| Gemcitabine+Oxaliplatin | 1 (100) | 0 (0) | ||
| Folfox | 0 (0) | 1 (100) | ||
| Carboplatin+Paclitaxel | 1 (50.0) | 1 (50.0) | ||
| Second Line Chemotherapy | ||||
| No | 0.440 | |||
| Gemcitabine+Cisplatin | 1 (20.0) | 4 (80.0) | ||
| Gemcitabine | 1 (16.7) | 5 (83.3) | ||
| Capesitabine | 1 (11.1) | 8 (88.9) | ||
| Folfox | 3 (42.9) | 4 (57.1) | ||
| Gemcitabine+Nabpaclitaxel | 0 (0) | 1 (100) | ||
| Paclitaxel | 0 (0) | 1 (100) | ||
| PNI < 44 (months) | PNI ≥ 44 (months) | P value | |
| Receiving Chemotherapy | 8.90 | 12.58 | 0.010 |
| Factor | Univariate Analysis | Multivariate Analysis | ||
| 95 % CI | p | HR (95 % CI) | p | |
| Age(<65 yaş vs ≥65 yaş) | 0.73-2.09 | 0.41 | ||
| Sex | 0.58-1.61 | 0.90 | ||
| ECOG PS | 1.97-6.59 | 0.00 | 1.76-6.03 | 0.00 |
| Tumor Location | 0.59-1.34 | 0.96 | ||
| Ca 19.9 | 0.25-0.79 | 0.005 | 0.24-0.77 | 0.004 |
| PNI | 0.26-0.76 | 0.004 | 0.29-0.90 | 0.02 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Cancer Diagnosis and Treatment · Pancreatic and Hepatic Oncology Research
Introduction
Gallbladder and biliary tract tumors are rare but highly fatal cancers. The majority of gallbladder cancers are found incidentally in patients being investigated for cholelithiasis [1]. Poor prognosis is thought to be related to the advanced stage at diagnosis, depending on both the anatomical position of the gallbladder and the non-specificity of symptoms [2]. Many risk factors have been identified in gallbladder tumors, and most of the risk factors are related to chronic inflammation [3]. Among these risk factors are cholelithiasis, porcelain gallbladder, gallbladder polyps, primary sclerosing cholangitis, and salmonella infection [4]. The primary treatment of gallbladder tumors is surgery. Adjuvant therapy is recommended in early-stage completely resected muscle-invasive (≥T1b) or lymph node-positive or surgical margin-positive patients. Adjuvant chemoradiotherapy is recommended in patients with positive surgical margins or lymph node metastases and capecitabine monotherapy for six months or capecitabine plus gemcitabine in patients with negative surgical margins [5]. Depending on the patient's tolerance, gemcitabine plus cisplatin, gemcitabine plus oxaliplatin, or gemcitabine can be used as a single agent. Cholangiocarcinomas are rare malignancies originating from the epithelial cells of intrahepatic and extrahepatic bile ducts [6]. Cholangiocarcinoma is an aggressive tumor that can metastasize beyond the bile ducts to other intrahepatic regions, the peritoneum, and distant extrahepatic organs. Risk factors for cholangiocarcinoma are as follows: primary sclerosing cholangitis, fibropolycystic liver disease, and chronic intrahepatic stone disease (hepatolithiasis, also called recurrent pyogenic cholangitis) [7]. Chronic liver disease (cirrhosis and viral infection) is also considered a risk factor, especially for intrahepatic cholangiocarcinoma [8].
The primary treatment of cholangiocarcinomas is surgery [9]. The contribution of adjuvant and neoadjuvant therapy in resected patients is controversial. Meta-analysis has shown a survival contribution, especially in node-positive patients [10]. Adjuvant chemoradiotherapy is recommended in patients who do not undergo R0 resection or in node-positive patients [11]. In patients with unresectable/metastatic cholangiocarcinoma, the addition of immunotherapy (durvalumab or pembrolizumab) to gemcitabine plus cisplatin is recommended as the first step in patients with good Eastern Cooperative Oncology Group Performance Status (ECOG PS) and without hyperbilirubinemia. A contribution to the overall survival (OS) was observed in both studies in which durvalumab/pembrolizumab was added to chemotherapy [12,13]. The prognostic nutritional index (PNI) is a parameter calculated using albumin and absolute lymphocyte value, reflecting the immunological and nutritional status of the cancer patient. Recently, studies have been conducted showing the prognostic importance of PNI in many types of cancer such as esophageal cancer [14], colorectal cancer, and stomach cancer [15]. In clinical studies, patients' nutritional status and immunity have been found to be associated with tumor growth and prognosis [16]. Gallbladder and bile pathway tumors are very rare tumors, and the prognostic effectiveness of PNI has not been evaluated in this disease group.
The aim of our study is to evaluate the prognostic effectiveness of PNI in unresectable/metastatic gallbladder and biliary tract cancers.
Materials and methods
Sixty-eight patients aged 18 years or over diagnosed with unresectable/metastatic gallbladder cancer and cholangiocarcinoma, between January 2014 and January 2023, were included in the study. The study was conducted in a single center. Patient files were examined retrospectively. Age, gender, ECOG performance status, date of diagnosis, etiological factors, first- and second-line treatment protocols, chemotherapy responses, albumin, bilirubin, complete blood count parameters at the time of diagnosis, final status, and final status dates were recorded.
Patients with missing data, unconfirmed diagnosis, curative surgery for early stage, and multiple primary tumors were excluded from the study.
The PNI was calculated using albumin and lymphocyte values (10 x albumin g/dL + 0.005 x total lymphocyte/mm^3^). The PNI of each patient at the time of diagnosis was calculated separately. The relationship between PNI and age, gender, ECOG PS, tumor localization, and CA19.9 level with OS was assessed.
OS was defined as the time from diagnosis to death or last visit for patients still alive. Survival data were last updated in March 2024. The primary endpoint of our study was to evaluate the relationship between OS and PNI.
Statistical analysis
All analyses were performed using the Statistical Product and Service Solutions (SPSS, version 23.0; IBM SPSS Statistics for Windows, Armonk, NY) program. In the descriptive statistics of the study, continuous variables were used as mean (standard deviation), and median (range); categorical variables were presented as frequency (percentage). The chi-square test or Fisher's exact test was used to compare the categorical variables of two independent groups. Independent sample t-test and Mann-Whitney-U test were used to compare parametric and non-parametric data, respectively. OS was estimated with the Kaplan-Meier method and compared with a log-rank test. The optimal cut-off value of PNI for predicting OS was determined with the receiver operating characteristic (ROC) curve. Univariate and multivariate logistic regression models were applied to evaluate the factors predicting OS. A logistic regression model was created with variables with a p-value of <0.05, and independent factors predicting OS were identified.
Results
Sixty-eight patients were included in the study. The median age of the patients was 60 years, and 41 (60.3%) of the patients were female and 27 (39.7%) were male. Twenty-eight (41.2%) of the patients were diagnosed with gallbladder cancer, while 40 (58.8%) were diagnosed with cholangiocarcinoma (Table 1).
Table 1: Percentage of subgroups of a specific parameter should be given vertically (i.e., percentage of males and females in PNI < 44 group and >= 44 group)ECOG PS: Eastern Cooperative Oncology Group Performance Status, FOLFOX: 5-fluorouracil, oxaliplatin, leucovorin; PNI: Prognostic nutritional index
The PNI mean of the patients included in the study was 44.8 (95% CI: 42.9-46.7), and the median was 44.77 (minimum: 22, maximum: 61.4). ROC analysis demonstrated a statistically significant prediction of OS when the PNI was < 44. (AUC: 0.715, sensitivity: 54.8%, specificity: 33.3%; p=0.08) (Figure 1).
Value of prognostic nutritional index in predicting overall survival
Patients were divided into two groups: PNI < 44 and ≥ 44. The median OS in the PNI < 44 group was 6.9 months (95% CI: 3.92-10.06). In the PNI ≥ 44 group, the median OS was 12.58 months (95% CI: 8.76-16.39). OS was statistically significant between the two groups (p = 0.004) (Figure 2).
Kaplan-Meier curve according to the prognostic nutritional indexOS: Overall survival, PNI: Prognostic nutritional index
Sixty of our patients were able to receive chemotherapy. The prognostic effectiveness of PNI was evaluated in patients receiving chemotherapy. In patients receiving chemotherapy, the median survival was found to be 8.93 months in the PNI < 44 group, while the median survival was found to be 12.58 months in the PNI ≥ 44 group. The difference between both groups was statistically significant (p = 0.010) (Table 2).
The median value of Ca 19.9 was 96. When the patients were divided into two groups according to the median value, the median OS was 14.1 months in the < 96 group, while the mean OS was 7.9 months in the ≥ 96 group. OS was statistically significant between the two groups (p=0.005) (Table 3).
In univariate analysis, the ECOG performance status, Ca 19.9, and PNI were statistically significant variables in predicting OS (p < 0.05). In multivariate analysis, the ECOG performance status, Ca 19.9, and PNI were found to be independent factors in predicting OS (p < 0.05) (Table 3).
Discussion
In our study, we found that the PNI is prognostic in terms of OS in patients with unresectable/metastatic gallbladder cancer and cholangiocarcinoma and could be informative to the clinician in patient follow-up. There are many studies evaluating the prognostic effectiveness of PNI in cancer patients. Sun et al. included 14 studies in their meta-analysis, and it was shown that PNI was associated with OS and postoperative complications in cancer patients [17]. In another study, including 3,393 gastric cancer patients, it was found that low PNI was an indicator of advanced TNM stage and was associated with lower OS [15]. Studies have been conducted on the prognostic effectiveness of PNI in other types of cancer, as well as gastrointestinal system tumors. A meta-analysis of lung cancer patients showed that low PNI value was associated with shorter PFS and OS in both non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC) patients. Being overweight is common in breast cancer patients, as opposed to malnutrition [18]. In a study evaluating the relationship of PNI with pathological response and survival in breast cancer, it was found that higher PNI values were associated with lower pathological complete response and shorter disease-free survival [19].
Gallbladder cancer and cholangiocarcinoma are rare tumors of the gastrointestinal system, data in this area are limited, and various studies are needed in both diagnosis and treatment methods. The most important prognostic factor in gallbladder tumors is the disease stage. Studies have found that age, gender, and surgery methods are also prognostic [20]. In a study conducted by Wang et al., a nomogram was developed to calculate the benefit of adjuvant chemotherapy and chemoradiotherapy in operated gallbladder cancers. In this study, it was determined that ≥ T2 and ≥ N1 tumors had the greatest benefit from adjuvant chemoradiation [21]. In another study evaluating prognostic factors in metastatic gallbladder cancer, neutrophil/lymphocyte ratio, Ca 19.9 level, carcinoembryonic antigen (CEA) level, and the presence of liver metastasis were found to be prognostic [22]. In our study, the Ca 19.9 level was found to be prognostic, consistent with this study.
Cholangiocarcinoma is a heterogeneous group, including intrahepatic and extrahepatic tumors, and prognostic factors were evaluated separately in subgroups. The most important prognostic factor in both groups is the disease stage, as in gallbladder tumors. The prognosis of resectable tumors is significantly better. A study found that, among the components of the American Joint Committee on Cancer (AJCC) staging, nodal positivity affects staging most strongly. In this study, microvascular invasion was found to be prognostic, as well as the AJCC stage [23]. In a study conducted on metastatic cholangiocarcinoma, the Ca 19.9 level and ECOG performance status were found to be prognostic [24]. In our study, both factors were found to be prognostic, consistent with this study.
In our study, we evaluated the prognostic effectiveness of PNI in the subgroup of patients who could receive chemotherapy. Patients who could not receive chemotherapy were generally unable to receive treatment because their performance was poor or their laboratory parameters were not suitable for chemotherapy. The low PNI in this group was the result we expected. Patients who could receive chemotherapy constituted a more homogeneous group. For this reason, we think that the prognostic importance of PNI may be more valuable in this group.
Conclusions
In conclusion, in our study, we evaluated the prognostic effectiveness of the PNI in two rare tumors and found that it was associated with survival. It is very valuable as it is the first study in the literature to evaluate the effectiveness of the PNI in these tumors. We believe that the PNI can be used as a marker to assist the clinician in evaluating the prognosis of patients in the clinic and predicting treatment tolerance. The main limitations of our study were the small number of patients and the retrospective study design.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gallbladder carcinoma in the era of laparoscopic cholecystectomy Arch Surg Yamaguchi K Chijiiwa K Ichimiya H 9819841311996879016910.1001/archsurg.1996.01430210079015 · doi ↗ · pubmed ↗
- 2A prospective analysis of 1518 laparoscopic cholecystectomies N Engl J Med The Southern Surgeons Club 107310783241991182614310.1056/NEJM 199104183241601 · doi ↗ · pubmed ↗
- 3Gallbladder cancer worldwide: geographical distribution and risk factors Int J Cancer Randi G Franceschi S La Vecchia C 1591160211820061639786510.1002/ijc.21683 · doi ↗ · pubmed ↗
- 4Epidemiologic aspects of gallbladder cancer: a case-control study of the SEARCH Program of the International Agency for Research on Cancer J Natl Cancer Inst Zatonski WA Lowenfels AB Boyle P 11321138891997926225110.1093/jnci/89.15.1132 · doi ↗ · pubmed ↗
- 5Adjuvant therapy in the treatment of biliary tract cancer: a systematic review and meta-analysis J Clin Oncol Horgan AM Amir E Walter T Knox JJ 193419403020122252926110.1200/JCO.2011.40.5381 · doi ↗ · pubmed ↗
- 6Neoplasms of the liver Mod Pathol Goodman ZD 06020 Suppl 1200710.1038/modpathol.380068217486052 · doi ↗ · pubmed ↗
- 7Risk factors for biliary tract carcinogenesis Ann Oncol Chapman RW 3083114199910436847 · pubmed ↗
- 8Risk factors for intrahepatic and extrahepatic cholangiocarcinoma: a systematic review and meta-analysis J Hepatol Clements O Eliahoo J Kim JU Taylor-Robinson SD Khan SA 951037220203153674810.1016/j.jhep.2019.09.007 · doi ↗ · pubmed ↗