The Investigation of Preoperative Factors Associated With Postoperative Outcomes Following Total Knee Arthroplasty for Osteoarthritis: A Scoping Review
Takafumi Nasu, Junya Yamanoi, Takashi Kitagawa

TL;DR
This review identifies preoperative factors linked to post-surgery discharge destinations after knee replacement surgery for osteoarthritis.
Contribution
The study systematically identifies 26 preoperative factors associated with non-home discharges after TKA, offering insights for optimizing medical resource use.
Findings
Age, gender, comorbidities, and obesity are among preoperative factors linked to discharge destinations.
Selecting discharge destinations based on preoperative factors may improve medical resource efficiency.
Future research should consider these factors within healthcare systems and hospital stay durations.
Abstract
This study aimed to investigate preoperative factors associated with non-home discharges from acute care hospitals in patients undergoing total knee arthroplasty (TKA) due to osteoarthritis. It was a scoping review focused on patients who received their first unilateral TKA for osteoarthritis. The research targeted observational studies that examined the destinations of patients post-surgery based on preoperative factors, with a literature search conducted in April 2023. Out of 3,255 identified papers, 28 met the eligibility criteria. A total of 26 preoperative factors were identified as potentially related to discharge destinations, including age, gender, comorbidities, and obesity. By selecting an appropriate discharge destination based on preoperative factors, there may be potential for more efficient use of medical resources. Future studies should consider preoperative factors in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
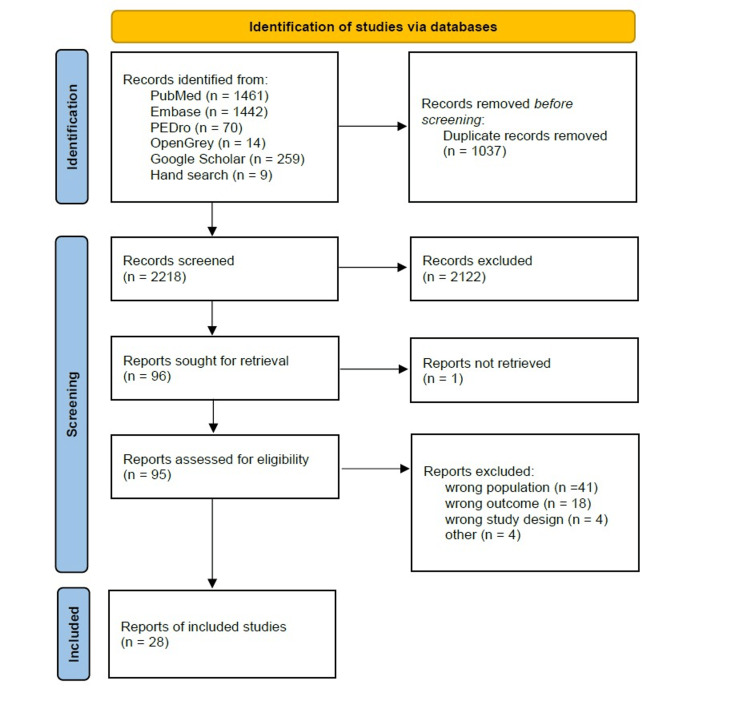 Figure 1
Figure 1| Search strategy |
| MEDLINE (via PubMed) search strategy |
| ("Arthroplasty, Replacement, Knee"[mh] OR "Knee Prosthesis"[mh] OR "knee replacement"[tiab] OR "total knee arthroplasty"[tiab] OR "TKR"[tiab] OR "TKA"[tiab] OR "KR"[tiab]) AND ("predict*"[tiab] OR "determin*"[tiab] OR "preoperative"[tiab] OR "factors"[tiab] OR "characteristic*"[tiab] OR "influence"[tiab] OR "affects"[tiab]) AND ("discharge*"[tiab] OR "Patient Discharge"[mh] OR "discharge disposition"[tiab] OR "discharge destination"[tiab] OR "rehabilitation ward"[tiab] OR "inpatient rehabilitation"[tiab] OR "Hospitals, Rehabilitation"[mh] OR "Subacute Care"[mh]) |
| Embase (via Elsevier) search strategy |
| ('Arthroplasty, Replacement, Knee'/exp OR 'Knee Prosthesis'/exp OR 'knee replacement':ti,ab OR 'total knee arthroplasty':ti,ab OR TKR:ti,ab OR TKA:ti,ab OR KR:ti,ab) AND (predict*:ti,ab OR determin*:ti,ab OR preoperative:ti,ab OR factors:ti,ab OR characteristic*:ti,ab OR influence:ti,ab OR affects:ti,ab) AND (discharge*:ti,ab OR 'Patient Discharge'/exp OR 'discharge disposition':ti,ab OR 'discharge destination':ti,ab OR 'rehabilitation ward':ti,ab OR 'inpatient rehabilitation':ti,ab OR 'Hospitals, Rehabilitation'/exp OR 'Subacute Care'/exp) |
| Author and year of publication | Country of origin | Age (years) | Gender (female) | Sample size | Length of stay (days) |
| Neuwirth et al. 2022 [ | USA | 60>: 23.1%, 60-70: 42.0%, 71-80: 27.3%, 81≦: 7.6% | 62% | 1,98,233 | NA |
| Issa et al. 2021 [ | USA | Mean; 68 (41-87) | 72.50% | 229 | 3 (1-22) |
| Zeng et al. 2021 [ | USA | Mean; 67.6 (SD 8.6) | 60.10% | 1,481 | NA |
| Gwam et al. 2020 [ | USA | Mean; home: 66 (SD 9.1), SNF: 71 (SD 9.3), rehabilitation 69 (SD 9.7) | Home: 59.1%, SNF: 72.8%, rehabilitation: 69.5% | 1,71,093 | NA |
| Rondon et al. 2017 [ | USA | Mean; home: 65.7, rehabilitation: 73.8 | Home: 57.3%, rehabilitation: 79.4% | 2,281 | Home: 2.0, rehabilitation: 3.4 |
| McLawhorn et al. 2017 [ | USA | 65≧: 45.1%, 66-75: 35.2%, 76≦: 19.7% | 62.40% | 1,01,256 | NA |
| Chan et al. 2018 [ | Singapore | Mean; home: 67.2 (SD 7.8), CH: 70.7 (SD 7.7) | Home: 77.5%, CH: 86.7% | 1,065 | Home: NA, CH: 23 (17-32) |
| Black et al. 2019 [ | USA | NA | NA | 2,058 | Albumin≦3.5 g/dL: 3.2, albumin>3.5 g/dL: 2.3 |
| Prohaska et al. 2017 [ | USA | Mean; 63.4 (SD 11.3) | 59% | 679 | NA |
| Robinson et al. 2017 [ | USA | Mean; male: 66.5 (SD 9.67), female: 66.8 (SD 9.82) | 62.30% | 87,177 | Hospitalization for more than 3 days, male 7.4%, female 7.9% |
| Rissman et al. 2015 [ | USA | Mean; 64.7 (SD 10.4) | 57% | 738 | 3.3 (1.2-13.5) |
| Lung et al. 2023 [ | USA | Mean; dehydration level none: 65.4, moderate: 67.6, severe: 68.5 | Dehydration level none: 45.5%, moderate: 31.8%, severe: 19.3% | 3,44,744 | Severe dehydration is likely to keep the patient in the hospital for more than two days |
| Hadad et al. 2022 [ | USA | Mean: black 64; white 67 | Black: 55%, white: 45% | 3,603 | Blacks are more likely to stay in the hospital for more than 3 days |
| Schwarzkopf et al. 2019 [ | USA | Mean; HCV-C: 63.0 (SD 7.5), HCV-UT: 61.7 (SD 6.9) | HCV-C: 46.9%, HCV-UT: 46.1% | 127 | HCV-C: 2.9, HCV-UT: 3.4 |
| Kerbel et al. 2021 [ | USA | Mean; 65.1 (17.9-87.7) | 66.20% | 1,614 | Non-obese (<30 kg/m2): 2.6 (SD 1.3), obese (30-39 kg/m2): 2.5 (SD 1.0), morbidly obese (≧40 kg/m2): 2.8 (SD 2.0) |
| Schwarzkopf et al. 2016 [ | USA | Mean; 68.7 | 62.70% | 28,611 | NA |
| Chen et al. 2023 [ | USA | Mean; national cohort 67 (58-76), institutional cohort 69 (60-78) | National: 59.5%, institutional: 62.8% | National: 424,354, institutional: 10,196 | National: 2.3 (SD 1.9), institutional: 2.8 (SD 1.4) |
| Ramkumar et al. 2019 [ | USA | Median; SNF: 72 (SD 9.7), non-SNF: 65 (SD 10.1) | SNF: 72.3%, non-SNF: 61.2% | 32,18,419 | SNF: 3.7 (SD 1.8), non-SNF: 3.1 (SD 1.6) |
| Pan et al. 2023 [ | USA | Mean; home: 66.1 (SD 9.2), non-home: 70.6 (SD 9.7) | Home: 59.3%, non-home: 70.7% | 4,62,858 | 2011 years: home: 3.3 (SD 4.5), non-home: 3.7 (SD 5.9), 2020 years: home: 1.4 (SD 1.6), non-home: 3.6 (SD 3.1) |
| Jorgenson et al. 2015 [ | USA | 65>: 56,575, 65≦: 72,947 | 64.20% | 1,29,522 | NA |
| Krishnan et al. 2021 [ | USA | Mean; cognitive: 75.75 (SD 6.27), non-cognitive: 75.32 (SD 6.17) | Cognitive: 69.2%, non-cognitive: 70.1% | 208 | Cognitive: 3.62, non-cognitive: 3.35 |
| Shichman et al. 2023 [ | USA | Mean; MetS: 64 (56-72), No MetS: 64 (55-73) | MetS: 76.5%, No MetS: 77% | 782 | MetS: 3.4 (1-5.8), No MetS: 3.0 (1.6-4.5) |
| Kooner et al. 2021 [ | Canada | Mean; psychiatric: 66.7 (SD 9.7), non-psychiatric: 66.7 (SD 9.6) | Psychiatric: 62.8%, non-psychiatric: 62.8% | 1,000 | Psychiatric: 6.0 (SD 7.00), non-psychiatric: 5.23 (SD 6.18) |
| Rudy et al. 2020 [ | USA | 55>: 10.7%, 55-64: 26.9%, 65-74: 39.2%, 75≦: 23.2% | 63.30% | 1,910 | 3.2 (2.3-3.3) |
| Crawford et al. 2011 [ | USA | Mean; 63.97 (SD 9.90) | 51.80% | 413 | 4.35 |
| Takada et al. 2021 [ | Japan | Mean; home: 71.4 (SD 8.9), hospital transfer: 76.1 (SD 8.1) | Home: 62%, hospital transfer: 88% | 89 | Median home: 18, hospital transfer: 17 |
| Oki et al. 2020 [ | Japan | Mean; 71.8 (SD 10) | NA | 60 | NA |
| Yamada et al. 2019 [ | Japan | Mean; home: 69.2 (SD 9.9), hospital transfer: 77.7 (SD 7.5) | 71% | 72 | Hospitalization for more than 14 days |
| Author | Country of origin | Preoperative factors |
| Neuwirth et al. 2022 [ | USA | Preoperative anemia, hematocrit ≥ 36%, hemoglobin > 12 g/dl |
| Issa et al. 2021 [ | USA | Age (older) |
| Zeng et al. 2021 [ | USA | Age (older), use of walking aids, exercise habits, dementia, neurological disorder |
| Gwam et al. 2020 [ | USA | Age (older), gender (female), race (Black), diabetes, BMI (high), preoperative white blood cells, hematocrit (low) |
| Rondon et al. 2017 [ | USA | Age (older), gender (female), insurance status (Medicare), race (non-Caucasian), comorbidities (CCI), history of depression |
| McLawhorn et al. 2017 [ | USA | Age (older), gender (female), BMI (high), comorbidities (CCI, ASA-AP), preoperative functional status (non-independent) |
| Chan et al. 2018 [ | Singapore | Age (older), gender (female), lower education |
| Black et al. 2019 [ | USA | Low albumin level (<3.5 g/dl) |
| Prohaska et al. 2017 [ | USA | Age (older), gender (female), preoperative anemia, preoperative obesity |
| Robinson et al. 2017 [ | USA | Gender (female) |
| Rissman et al. 2015 [ | USA | Age (older), gender (female), comorbidities (CCI), preoperative obesity, preoperative pain catastrophizing scale |
| Lung et al. 2023 [ | USA | Dehydration (moderate to severe) |
| Hadad et al. 2022 [ | USA | Race (Black) |
| Schwarzkopf et al. 2019 [ | USA | Untreated hepatitis C virus, insurance status |
| Kerbel et al. 2021 [ | USA | Obesity (30-39 kg/m²), morbidly obese (≥ 40 kg/m²) |
| Schwarzkopf et al. 2016 [ | USA | Age (older), comorbidities (CCI), race (Asian, Black), insurance status |
| Chen et al. 2023 [ | USA | Age (>68), gender (female), BMI (>33.35 kg/m²), comorbidities |
| Ramkumar et al. 2019 [ | USA | Age (older), gender (female), race (Black), comorbidities (CCI) |
| Pan et al. 2023 [ | USA | Age (older), gender (female), obesity (BMI > 40 kg/m²), comorbidities (ASA-AP, CCI), race (Black, Asian), preoperative functional status (non-independent), smoker |
| Jorgenson et al. 2015 [ | USA | Race (African American) |
| Krishnan et al. 2021 [ | USA | Preoperative cognitive impairment |
| Shichman et al. 2023 [ | USA | Morbidly obese, metabolic syndrome |
| Kooner et al. 2021 [ | Canada | Psychiatric illness |
| Rudy et al. 2020 [ | USA | Married/partnered, comorbidities (CCI), insurance status |
| Crawford et al. 2011 [ | USA | Age (older), comorbidities (ASA-AP) |
| Takada et al. 2021 [ | Japan | Non-operative side extensor strength |
| Oki et al. 2020 [ | Japan | TUG test, comfortable gait speed |
| Yamada et al. 2019 [ | Japan | Comfortable gait speed |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTotal Knee Arthroplasty Outcomes · Cardiac, Anesthesia and Surgical Outcomes · Orthopaedic implants and arthroplasty
Introduction and background
Total knee arthroplasty (TKA) is commonly performed as a treatment for osteoarthritis, which causes pain, decreased physical function, and reduced activities of daily living, and is considered one of the most cost-effective surgeries [1]. Its frequency is on an increasing trend in many developed countries, with projections indicating a 673% increase in the United States by 2030 [2]. In Japan, the number of surgeries exceeded 70,000 in 2021, and it is expected to continue to rise annually until 2030 [3-5]. The rapid increase in TKA patients leads to significant economic burdens on healthcare systems, necessitating reductions in healthcare costs to sustain the current systems [6-7]. The costs associated with TKA are primarily due to hospitalization expenses, and there is a trend toward reducing the length of hospital stays [8].
In the United States, the average length of stay in acute care hospitals has been decreasing annually, reaching two to three days [9]. Regarding discharge destinations, the short duration of hospital stays may contribute to home discharge rates ranging from 10% to 40% [10-11]. In contrast, in Japan, the average length of stay in acute care hospitals is about 24 days [12]. Due to the longer hospital stays compared to Western countries, 80-90% of patients are reported to return home [12], although a certain number traditionally transfer to rehabilitation hospitals. Nagaoka and Nitta have suggested that differences in the medical insurance system and the number of acute care beds per capita influence the length of hospital stays in Japan [13]. It is unclear if the high rate of home discharge can be maintained if hospital stays decrease like in other countries. Japan must also efficiently utilize medical resources and select appropriate discharge destinations in anticipation of the increasing number of TKA patients each year [14]. Considering discharge destinations preoperatively is essential for smooth discharge planning within limited postoperative hospital stays. Prior studies examining preoperative factors related to discharge destinations have indicated that being female is a predictor for discharge to rehabilitation facilities [15]. However, these studies did not include research conducted in Japan. A comprehensive examination of the latest preoperative factors, including studies from Japan, is expected to provide valuable insights for determining appropriate discharge destinations.
Therefore, we comprehensively collected information on preoperative factors associated with the transfer from acute care hospitals to rehabilitation hospitals or discharge destinations other than home after TKA due to osteoarthritis of the knee. We summarized the current evidence from various countries, including Japan.
Review
Subjects and methods
This scoping review was conducted to examine preoperative factors related to outcomes following TKA for osteoarthritis of the knee. This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension for Scoping Reviews [16]. Additionally, the research protocol was registered in advance with the Open Science Framework, following the methodology for scoping reviews.
The selection criteria of the study were determined using the Patient, Concept, Context (PCC) framework [17]. The subjects were patients in acute care hospitals who underwent unilateral TKA due to osteoarthritis, with no restrictions on age or gender. Excluded were patients who underwent unicompartmental knee arthroplasty, revision surgeries, bilateral surgeries, or had postoperative mobility restrictions such as non-weight bearing. Although postoperative hospital stay lengths vary internationally due to different insurance systems, this study focused on preoperative factors related to non-home discharge destinations (such as transfers to rehabilitation hospitals or other facilities). Factors unrelated to patients such as hospital functions, size, and regional differences were excluded from the study. The preoperative factors considered included inherent factors such as age and gender, as well as physical functionality, economic factors, and family presence. Observational studies were employed for the included papers. Studies using large databases were also employed. Case reports, interventional studies, systematic reviews, meta-analyses, and narrative reviews were excluded.
Search Method
Database searches were conducted using MEDLINE, Embase, PEDro, and Google Scholar in English. Additionally, to conduct a search for grey literature, OpenGrey was used. To further examine preoperative factors specific to Japan, a hand search of major Japanese journals was performed. The searches in each database were conducted using search formulas based on the terms "total knee arthroplasty," "preoperative factors," "outcomes," "predictive factors," and "preoperative factors." The literature search was conducted on April 1, 2023, and included papers published up to March 2023. (Table 1).
Article Selection Method
After completing the database searches, results were uploaded to Rayyan, and duplicates were removed. Two authors (TN, JY) independently selected articles, consulting another author when opinions diverged. Initially, about 10 articles were excluded based on titles and abstracts during a pilot screening using pre-established eligibility criteria. For articles whose full texts were not accessible, authors were contacted via ResearchGate to obtain the documents. Subsequently, a secondary screening was conducted to verify full texts, and only those meeting the eligibility criteria were included in the study.
Data Extraction
The items for data extraction were developed based on the PCC framework. Two authors (TN, JY) independently conducted data extraction from the eligible articles. Disagreements were resolved through discussion, and if no agreement could be reached, a third author was consulted to resolve the issue. Data extracted included the objectives of the studies, demographic information (age, gender) of the participants, discharge destinations, average length of stay, and preoperative factors related to outcomes.
Integration of Results
A PRISMA flowchart was created to summarize the search results and literature selection. The extracted data were organized into tables using Excel, presenting information on age, gender, number of subjects, length of hospital stay, and preoperative factors.
Results
Study Selection
From the database search, 3,255 articles were identified, and ultimately 28 met the eligibility criteria and were included [18-45]. A flowchart is shown in Figure 1. The selected studies involved observational research on patients undergoing TKA due to osteoarthritis, focusing on preoperative factors and discharge destinations. Studies ranged from single-site investigations to those utilizing large-scale databases. Of the selected articles, 23 were from the United States, 3 from Japan, 1 from Singapore, and 1 from Canada.
PRISMA flowchart for paper selectionPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Characteristics of Selected Studies
The studies selected examined preoperative factors related to non-home discharge destinations. Most studies targeted older adults, with an average age over 65, and tended to involve more female participants. Reports from the United States indicated nearly all patients were discharged within five days post-operation, identifying 26 preoperative factors, including patient-specific and environmental factors (Tables 2-3).
Primary Characteristics (Preoperative Factors)
Among the 26 identified factors, 9 were frequently reported across multiple studies.
Age: Thirteen studies identified age as a factor influencing non-home discharges. Older patients were more likely to be discharged to destinations other than home compared to those who were discharged home. Studies categorizing age showed an increased likelihood of non-home discharges with increasing age.
Gender: Ten studies found that females were more likely than males to be discharged to non-home destinations.
Comorbidities: Nine studies cited comorbidities as influencing discharge destinations, using indices like the Charlson Comorbidity Index (CCI) and the American Society of Anesthesiologists Physical Status (ASA-PS). Higher scores and classifications on these indices were associated with an increased likelihood of non-home discharges.
Obesity: Body mass index (BMI) over 30 kg/m^2^ was associated with an increased likelihood of non-home discharges in nine studies, with even higher probabilities for BMIs over 40 kg/m^2^.
Other: Other factors identified in at least two studies that increased the likelihood of non-home discharges included race (Black), insurance type (Medicare), anemia, low preoperative functional independence, and cognitive impairment.
Discussion
The study showed that preoperative factors such as age, gender, comorbidities (CCI, ASA-PS), and obesity are associated with non-home discharge destinations after TKA. From the selected articles, 26 preoperative factors were extracted, with nine being commonly reported in at least two articles. Moreover, it was evident that not just one, but multiple preoperative factors are interconnected and influence the discharge destination. The selected studies were predominantly from the United States, where nearly all patients were discharged within five days. In contrast, Japanese studies reported hospital stays exceeding two weeks, highlighting significant differences in length of stay. When comparing preoperative factors, U.S. studies frequently selected patient-specific factors, whereas Japanese studies extracted factors related to physical function and performance, such as lower limb strength and walking speed. This indicates the need to adapt preoperative factors considering the healthcare systems and hospital stay durations specific to each country or region.
Age has been reported in prior studies to influence longer hospital stays and transfers [46-47], and this study supports these findings with age being highlighted in 13 papers. Generally, as age increases, so does the number of comorbidities [48], which can prolong the time needed for postoperative functional recovery [49]. Additionally, reports suggest that females may require more time to regain daily living activities, extending their hospital stays [46]. The most common comorbidities in TKA patients are reported to be hypertension (67.74%), obesity (21.73%), and diabetes (19.83%), indicating that many TKA patients have multiple comorbidities [50]. These patient-specific factors - age, gender, and comorbidities - are commonly selected for these reasons. However, while obesity is known to increase the risk of postoperative complications [51]; studies in Asian populations have shown no significant differences in short-term clinical outcomes, suggesting a lack of consensus [52]. Reports on the relationship between obesity and TKA are prevalent in Western literature, but are scarce in Asia, necessitating further examination before using obesity as a predictive factor in Japan.
Sattler et al. [15], conducted a systematic review and meta-analysis identifying predictors for the need for inpatient rehabilitation after TKA, which included age, obesity, comorbidities, and gender as predictive factors. This study found similar factors, reflecting those results. Additionally, although excluded from this study, tools like the Risk Assessment and Prediction Tool, which predicts using multiple factors, have been validated in various countries [13,53], including questions about age and gender, indicating that multiple patient-specific factors are interrelated.
In Japan, factors related to the prediction of hospital stay duration and independent walking have been examined, including the timing of cane walking initiation and physical function [54-55]. However, studies reporting factors related to discharge destinations are scarce, and it is unclear if appropriate destinations are being selected. In cases of extended stays over two weeks, like in Japan, factors other than patient-specific ones, such as postoperative physical function recovery and higher independence in daily and instrumental activities (outdoor walking, stair climbing), are considered.
Limitation
The limitations of this review are threefold. First, the majority of the studies selected are from the USA, with other regions such as Europe under-represented. In Europe, many studies consider joint replacement in general, making it difficult to isolate factors specific to TKA. In addition, there are few reports on preoperative factors associated with discharge destination in Japan, with a limited number of studies and participants for comparison. Second, the effects of surgical factors and osteoarthritis severity, which are associated with postoperative recovery of physical function and discharge destination [56], have not been investigated. Third, in Japan, acute hospital admissions may be influenced by social factors, meaning that patient-specific factors and functionality alone do not determine the length of hospital stay, suggesting that factors beyond those studied may also influence outcomes. To further explore these limitations, it would be necessary to examine factors including social factors preoperatively.
Conclusions
This study suggests that advanced age, female gender, comorbidities, and obesity are associated with the discharge destinations of patients following TKA. Predicting postoperative outcomes from preoperative factors can facilitate the selection of appropriate discharge destinations, thereby enabling efficient utilization of healthcare resources. Future research should consider preoperative factors in light of Japan's healthcare system, duration of hospital stays, as well as racial and social backgrounds.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Knee replacement Lancet Price AJ Alvand A Troelsen A 1672168239220183049608210.1016/S 0140-6736(18)32344-4 · doi ↗ · pubmed ↗
- 2Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030 J Bone Joint Surg Am Kurtz S Ong K Lau E Mowat F Halpern M 7807858920071740380010.2106/JBJS.F.00222 · doi ↗ · pubmed ↗
- 3Japanese arthroplasty Association/Japanese arthroplasty registry Secretariat tha/TKA/UKA/PFA/TSA registry case statistics for the fiscal year 2021 4 2023 https://jsra.info/data/pdf/report-2021.pdf
- 4Projected numbers of knee and hip arthroplasties up to the year 2030 in Japan J Orthop Sci Matsuoka H Nanmo H Nojiri S Nagao M Nishizaki Y 1611662820233459328510.1016/j.jos.2021.09.002 · doi ↗ · pubmed ↗
- 5Difference in recovery of motor function after total knee arthroplasty between the early discharge program and the standard hospitalization program -in a non-inferiority trial Phys Ther Res Hiyama Y Taniguchi M Kamitani T Wada O Mizuno K 263271442017
- 6The projected burden of primary total knee and hip replacement for osteoarthritis in Australia to the year 2030 BMC Musculoskelet Disord Ackerman IN Bohensky MA Zomer E Tacey M Gorelik A Brand CA de Steiger R 902020193079722810.1186/s 12891-019-2411-9PMC 6387488 · doi ↗ · pubmed ↗
- 7Usefulness of a national hospital database to evaluate the burden of primary joint replacement for coxarthrosis and gonarthrosis in patients aged over 40 years Osteoarthritis Cartilage Maravic M Landais P 6126151420061647655610.1016/j.joca.2005.12.009 · doi ↗ · pubmed ↗
- 8Patient selection in outpatient and short-stay total knee arthroplasty J Surg Orthop Adv Lovald S Ong K Lau E Joshi G Kurtz S Malkani A 282320142464189110.3113/jsoa.2014.0002 · doi ↗ · pubmed ↗