Relationship Between Ankylosing Spondylitis and Cerebrovascular Disorders: A Systematic Review
Mohammad Mahdi Heidari, Azad Khaledi, Amir Mohammad Taravati, Ali Rastegar-Kashkouli, Farzaneh Moammer, Iman Saffari

TL;DR
People with ankylosing spondylitis face a higher risk of cerebrovascular diseases, likely due to inflammation and atherosclerosis.
Contribution
This systematic review provides a comprehensive analysis of the link between ankylosing spondylitis and cerebrovascular disorders.
Findings
Most studies found higher cerebrovascular risk in ankylosing spondylitis patients compared to the general population.
The risk of ischemic stroke was elevated in young ankylosing spondylitis patients in some studies.
Cardiovascular risk increased with age in both sexes across all subgroups.
Abstract
Cerebrovascular events are linked to ankylosing spondylitis. Accelerated atherosclerosis and endothelial dysfunction against a backdrop of inflammation have been widely blamed for the increased cerebrovascular risk in ankylosing spondylitis. The absence of a comprehensive review encouraged us to consider the link between ankylosing spondylitis and cerebrovascular diseases. Web of Science, PubMed, Medline, Scopus, and EMBASE were searched to identify studies published from 2000 to June 10, 2023. All observational and cohort studies reporting myocardial infarction or stroke and considering classic cerebrovascular risk in ankylosing spondylitis patients and healthy controls were included. Most of the included studies reported that the risk of cerebrovascular disorders was greater in ankylosing spondylitis than in the general population. Also, most studies showed that for both sexes, the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1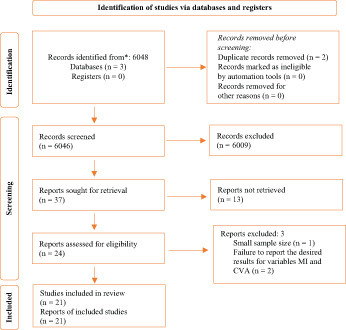 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpondyloarthritis Studies and Treatments · Rheumatoid Arthritis Research and Therapies · Sarcoidosis and Beryllium Toxicity Research
Introduction
Cardiovascular diseases (CVD) include a wide range of diseases related to blood vessels and heart.^1,2^ Cardiovascular diseases kill many patients in the world.^3^ Cardiovascular illnesses kill more than 60 million years of life in European countries yearly, including early deaths in those under 70, and men have greater age-standardized rates of morbidity and mortality from CVD than women, especially in those under 70.^4^ Cardiovascular diseases in recent years have been increasing.^5^ It is well known that people with inflammatory rheumatic sicknesses have a higher chance of rising CVD.^6^
A lot of research showed that chronic systemic inflammation makes atherosclerosis more likely to happen and makes people more likely to get blood clots by interfering with normal blood clotting and causing a state of coagulation dysfunction.^7^ In this situation, inflammatory diseases like rheumatoid arthritis (RA) and ankylosing spondylitis (AS) have been connected to cerebral events.^8^ Augmented cardiovascular risk in AS has been connected to inflammation and its effects on atherosclerosis and endothelial function.^9^ Hypertension^9,10^ and metabolic syndrome^11,12^ as 2 cerebrovascular event (CVE) risk factors have a high prevalence in AS.
The 3E Initiative in Rheumatology states that AS is present if many of the following characteristics are present, in addition to persistent back pain of at least 3 months’ duration: sacroiliitis/spondylitis by imaging, alternating buttock pain, response to non-steroidal anti-inflammatory drugs (NSAIDs), inflammatory back pain, symptom onset before age 45, presence of confirmed acute anterior uveitis, presence of peripheral disease manifestations (arthritis, dactylitis, or enthesitis), presence of HLA-B27 positivity, and positive family history of disease.^13,14^
Nonsteroidal anti-inflammatory drugs are suggested as the first treatment.^15 16^ In contrast to their usage in other kinds of inflammatory arthritis, when they are taken just during flares, NSAIDs are commonly used long-term and continuously in AS. Furthermore, it is well recognized that various forms of NSAIDs have a varying risk of CVE.^17 18^ Cox-2 inhibition is responsible for the anti-inflammatory and analgesic benefits of NSAIDs, but it also increases hypertension and platelet activation in response to thromboxane, creating a net prothrombotic impact. It has been demonstrated via research on RA that TNFi is linked to a lower chance of CVE risk, most likely as a result of a less inflammatory load.^19^
Evidence in axial spondyloarthritis (SpA) patients is largely restricted to individuals with radiographic disease symptoms, i.e., AS, also known as radiographic axial spondyloarthritis (r-axSpA). Psoriatic arthritis (PsA) is also a source of proof in peripheral SpA cases.^20^
It is well-established that RA patients have a greater risk of cardiovascular death compared to the general population,^21^ but statistics for PsA are less clear. Nonetheless, an analysis conducted by Jamnitski et al^22^ reported higher rates of hypertension prevalence in patients with AS compared to those without AS. In the face of this, there was no rise in the occurrence of cerebrovascular disease/stroke in patients with AS compared to people without AS.^23^ A higher risk of ischemic heart disease has also been linked to AS, according to studies conducted previously.^11^
Although the findings of these studies are crucial, the authors’ attention was primarily directed toward the diagnosis of AS, and little is recognized around the connection between AS and cerebrovascular disorders. Since no recent systematic review has addressed this gap in knowledge, it encouraged us to consider the link between AS and cerebrovascular.
Material and Methods
Search Strategy
PubMed, and EMBASE was explored to recognize studies published from 2000 to June 10, 2023. All observational studies monitoring MI or stroke and all cohort studies seeing classic (blood glucose, blood pressure, lipid summary, metabolic syndrome, and body mass index (BMI)), and newer CV risk factors in AS people and healthy people were involved.
Eligibility Criteria
Inclusion Criteria
The studies published in English up to December 2022, case–control and observational studies reported the population of AS patients agreeing to the reliable standards,^24^ data containing the number of MIs or strokes, or the CV risk factor profile included.
Exclusion Criteria
The article that we did not include in our study were case reports, commentary or discussion, and studies comprising >5 patients, no AS patients, no information around CV risk factors or CV illnesses, no full text, no visible data (no standard deviation (SD) or no interquartile range)
Risk of Bias
To avoid reporting and database bias in systematic reviews, we also evaluated unpublished reports and materials through manual search. Due to limiting the search of this study to a database such as Medline, the language bias has also been removed. In order to remove the multiple publication bias in this study, after detailed investigations, only 2 studies were found that examined the same population. Due to the different reporting of the results in them (Park et al^25^ stated the results in the field of MI and Lee et al^26^ in the field of CVA), both studies remained in the final evaluation. In order to carry out this study, the review of the sources included in related articles was not accepted, so citation bias will not have a place in this study. Considering that in some of the reviewed articles, the reports were limited to only one aspect and the researchers only reported outcomes with significant results, there was a possibility of outcome reporting bias in this study. A case that is less studied will be safe from having this bias. In this study, a manual search was also done, so the researchers chose the existence of gray literature bias at the cost of eliminating the language bias. Regarding time lag bias and media attention bias, these 2 biases are not evaluated in this review.
Quality Assessment of Studies
As shown in Supplementary 1, based on the Critical Appraisal Tool for Systematic Reviews (CASP) checklist,^27^ we assessed the quality of the reports included. The questions in this checklist are specific for each type of study method; questions 1 and 2 help to quickly determine the quality of the study. If the first 2 questions are positive, the other questions are also checked. There are 3 options for each question. There is that “YES,” “NO,” or “can’t say” was recorded depending on the opinion of each of the authors. At the end the responsible author gave the final opinion about each question after discussing it with the author for each question.
Synthesis of Results
Stroke incidence rates in our study are the number of strokes as a function of a follow-up period, and stroke rate ratios as the ratio of stroke incidence rate in the observed group (e.g., AS) over in the normal people.
Some studies did not provide the number of patient years observed for the control group and the number of strokes, but instead only provided the rate ratio together with a confidence interval (CI). As per the Cochrane Handbook,^28^ CI can be converted to the natural logarithms of rate ratios and standard errors may be combined across studies using the generic inverse variance method. We used this method to combine stroke risk for the age category pooled analysis and for stroke.
Results
Figure 1 shows the studies that were finally retrieved and identified by the literature search. Of 6048 studies, 19 qualified studies were included after evaluations, and 2 via hand searching, for a total of 122 036 AS patients and 2 818 985 controls.
Features of Studies
Of 21 publications, 1 was an observational study and 20 were cohort studies. Seventeen searches considered the prevalence of MI, and 14 studies judged stroke in AS patients. Ten of those considered both MI and stroke. Sixteen studies discussed covariates (diabetes, hypertension, hyperlipidemia, hypercholesterolemia, etc.) and presented data regarding the CV risk factors.
Cardiovascular Events
Myocardial Infarction
Of 16 studies, 6402 (n = 122 036) MIs were described. As presented in Table 1, 15 showed the MIs in the control groups (64 588 in 2 818 985). Szabo et al^29^ reported a high number of MI among the general population (GP) and AS patients; 19 113 in GP vs. 4127 MI in AS patients, in CV Definition 1, and in CV Definition 2; 8111 in GP vs. 2748 in AS. Their study was based on 2 definitions of cerebrovascular disease (when using CV Definition 1, the diagnosis of cardiovascular or cerebrovascular disease must be made using at least 1 applicable International Classification of Diseases, Ninth Revision (ICD-9) diagnostic code during the time period in question. When using CV Definition 2, the diagnosis must be made using at least 2 such codes). Most of the included studies showed that the prevalence of CVDs increased with increasing age for all CVD subgroups, and was similar for individuals of both sexes, but Essers et al^30^ expressed that in women, the risk of developing IHD was increased (hazard ratio (HR) 1.88, 95% CI 1.22-2.90), while the incidence rates were overall lower for women than men in the study conducted by Bengtsson et al.^31^ Although, in a study conducted by Walsh et al^32^ men have an increased risk of developing CVD compared to women, in contrast, Brophy et al^23^ indicated that there was no rise in MI in AS group compared to those without AS, in spite of the upper rate of hypertension.
Cerebrovascular Accident
In 14 studies (n = 12,853 patients), strokes were reported in AS patients. Twelve studies reported 44 021 strokes in control groups (Table 2). Except for Chou et al,^33^ other studies stated that the rate of CVA in AS patients was greater than control groups. In researches directed by Zöller et al,^34^ and Derakhshan et al,^35^ they only reported the incidence of CVA in AS patients and did not report it in control groups. In a study conducted by Zöller et al.^34^ 3477 patients (2416 men and 1061 women) had CVA, they concluded that admission to hospital, for many IMDs was related to increased risk of stroke. Also, Brophy et al.^23^ concluded that there was no increase in CVA rate in patients with AS compared to those without AS (40 in AS vs. 20 215 in control group). Similar to Essers et al,^30^ Bengtsson et al,^31^ Dong Hyun et al,^26^ Walsh et al,^32^ Trömmer et al,^36^ and Exarchou et al^10^ reported the same.
In a study conducted by Lin et al,^37^ the crude HR of ischemic stroke for AS group was 1.98 (95% CI, 1.20-3.29; P = .0079); age and sex were not included in the multiple regression analysis and of the 21 AS patients who developed stroke, 15 (71.4%) were male. The mean age of these 21 AS patients was 38.0 years (SD = 6.9), elder than that (31.3 years, SD = 7.6) of the remaining 4541 AS patients who did not develop stroke (*P *= .0001); they reported that the risk of developing ischemic stroke was higher in young patients with AS. Eriksson et al^38^ stated that there are 65 CVA in AS group vs. 148 CVA in the control group, also for stroke, the relative risks were 1.5 (1.1 to 2.0) in AS compared to the control group.
Comparison of Hazard Ratio or Risk Ratio (95% Confidence Interval) for Myocardial Infarction
Based on data reported in Table 3, 6 studies reported HR or risk ratio (RR) (95% CI) for MI. The lowest HR was reported by Essers et al (HR: 0.90 (0.64-1.26) that adjusted to 0.76 (0.53-1.09). Other studies that reported HR for MI with 95% CI had similar values to the mentioned number. It should be noted that in the studies conducted by Szabo et al,^29^ values of standardized prevalence ratios (95% confidence intervals) were listed instead of HR and RR (1.25 (1.15-1.35). Additionally, Eriksson et al reported RR for MI, RR: 1.42 (1.08-1.86), adjusted RR: 1.3 (1.0-1.7).
Comparison of Hazard Ratio or Risk Ratio or Odds Ratio (95% CI) for Cerebrovascular Accidents
As presented in Table 3, in 11 studies, authors reported HR or RR (95% CI) for CVA. The lowest HR was reported by Bengtsson et al, HR: 0.76 (0.64-0.89) that adjusted to 1.25 (1.06-1.48). Others reported HR for MI with 95% CI had similar values to the mentioned number, except for Keller et al, who reported a different and higher value than the others [2.3 (1.9–2.8)]. It should be noted that in Zoller et al’s study, values of standardized incidence ratio were reported instead of HR and RR (1.23 (1.01 - 1.48). It is noteworthy that Szabo et al^29^ reported OR in their study based on the age groups of the considered patients; in <50 years 1.45 (0.7-3.2), in 50-65 years 1.17 (0.91-1.50), and 65 years <1.12 (0.95-1.33). Hung et al also reported their results based on the follow-up periods of the patients; HR: 1.19 (0.89-1.58) and adjusted HR: 1.26 (0.94-1.68), in 3-year f/u HR: 1.16 (0.95-1.41) and adjusted HR: 1.14 (0.93-1.40), and 5-year f/u HR: 1.24 (1.05-1.46) and adjusted HR: 1.20 (1.02-1.42).
Discussion
Cardiovascular disease is the key reason for mortality in many industrialized nations.^39^ Inflammatory rheumatic disorders are known to enhance CVD burden and risk^6^; As the report of previous studies in recent years showed this fact, but Bremander et al,^40^ Zoller et al,^34^ Buschiazzo et al,^41^ and Ahmed et al^42^ did not report it. First, these studies were mostly conducted before 2012, and until then the effective role of these factors in the mortality of patients with AS had not been proven. Since AS itself is chronic,^43^ all included studies have taken into account the necessity of conducting surveys over a prolonged period of time to accurately consider the effects on the mortality rate and the risk of MI and CVA.
Regarding the relationship between AS and the chance of MI, the RR or HR were analyzed in the studies we included. The data obtained from this study showed that the occurrence of MI in patients with AS increased compared to the control group, and this rate is at least 1.25 times.^29^ However, contrary to this fact, a study conducted by Essers et al^30^ reported this rate as HR: 0.90 (0.64-1.26), which they considered covariates such as adjusted for gender, age, CVD, renal failure, hypertension, BMI, alcohol use, smoking history, NSAIDs, antiplatelet, antihypertensive, antidiabetics, statin use, in the analysis with the multivariate Cox model method and adjusted hazard ratio expression, this rate was reported as adjusted HR: 0.76 (0.53-1.09) for MI. In their study, a large and statistically valid sample was used, but in contrast to prior studies which included both prevalent and incident patients, they only included those who had recently been diagnosed with AS. Misdiagnosis is a further problem due to the study’s wide definition of IHD which included various ischemic heart diseases and symptoms, including angina pectoris. Since many different medical issues may result in chest discomfort^44^ so, it’s conceivable to misdiagnose it. This should be noted, researchers looked at acute myocardial infarction as a more “reliable” marker for IHD, since it is identified with electrocardiogram and blood abnormalities. Also, Essers et al^30^ did not note the way to minimize of possible bias that may have happened every study.
Szabo et al^29^ reported a high number of MI among the GP and AS patients. However, Essers et al found that the occurrence of cardiovascular disorders did not increase with age for any subset of CVDs or between sexes,^30^ and expressed that in female patients, the risk of growing IHD was augmented (HR 1.88, 95%CI, 1.22-2.90), while the incidence rate was overall lower for women than men in a study carried out by Bengtsson et al^31^ Although, in a study conducted by Walsh et al,^32^ the risk of developing CVDs was higher in men compared to women.
Despite a higher prevalence of hypertension in patients with AS compared to those without AS, a finding that Brophy et al^23^ attribute to the use of NSAIDs, the risk of MI was not increased in the former group.
Young patients with a fresh diagnosis of AS have an increased chance of acquiring IHD, as shown by Huang et al.^45^ On the contrary, despite a historically high incidence rate of MI, this rate has reduced in recent years, as a trend seen by Eriksson et al,^38^ and Szabo et al^29^ showed that the point estimates were the uppermost in the earliest age. Although the incidence rate of MI was high in the past years, this rate declined from 2018 onward, but in a study conducted by Derakhshan et al^35^ from Iran, this rate was still high.
There is the same thing to investigate the relationship of CVA in AS patients, with the difference that Bengtsson et al^31^ considered other covariates, and they reported hazard ratio (HR) from 0.76 to 1.25. They also surveyed only patients diagnosed with incidental AS, although they covered a larger percentage of patients based on age groups (18-99 years); but for judging the reliability of their results, conducting a similar study in AS patients with the same age group in diagnostic subgroups (prevalent, incidental, etc.) is needed.
According to research conducted by Zöller et al,^34^ they determined that there was an elevated risk of ischemic or hemorrhagic stroke among those who had been hospitalized for several IMDs. Also, Brophy et al^23^ concluded that there was no increase in CVA in patients with AS compared to those without AS. Similar to Essers et al,^30^ Bengtsson et al,^31^ Dong Hyun et al,^26^ Walsh et al,^32^ Trömmer et al,^36^ and Exarchou et al^10^ reported the same. In a study conducted by Lin et al,^37^ of the 21 AS patients who had a stroke, 15 (71.4%) were men; however, neither sex nor age were included. They finally concluded that the risk of developing a stroke was higher in young patients with AS. Eriksson et al^38^ showed that the relative risks were 1.5 (1.1 to 2.0) for stroke in AS related to the control group. Generally, there was not enough data to support the idea that sex and age are effective in the frequency of CVA.
In the context of investigating the mortality of CVDs in rheumatological diseases; despite the fact that it is clear that RA patients have a higher CV mortality rate than the overall population,^21^ but the data for PsA are inconsistent where in 2013, Jamnitski et al^22^ performed a comprehensive study and found that patients with PsA had a higher death rate. Two studies included^46,47^ in our review revealed an increased standardized mortality ratio (SMR) of 1.4-1.6 for all mortality cases. On the contrary, a comprehensive perspective PsA cohort study carried out by Buckley et al^51^ from the UK, did not find a significant mortality increase [SMR 0.81 (95% CI 0.57-1.12)], although they reported that CV accounted for 38% of deaths,^48^ but what arose from the studies reviewed in this systematic review was that the comparison of mortality in patients with AS still requires more studies in this field, although the 2 studies^10,41^ which did this comparison definitely showed that the mortality rate is high in patients with AS.
Compared to age-matched healthy controls,^49^ individuals with AS have been shown to be more likely to be smokers and have a higher BMI. C-reactive protein, interleukin 6, and fibrinogen levels were all considerably higher in these individuals after controlling for smoking and body mass index.^50^ Although there was an increased incidence of conditions such hypertension, dyslipidemia, diabetes, obesity, and metabolic syndrome, these conditions alone cannot fully explain the higher risk shown in this cohort. Several noninvasive methods may be used to assess the extent to which chronic, systemic inflammation has contributed to the development of accelerated atherosclerosis (41). More studies are required to determine the impact of anti-inflammatory medication, particularly NSAIDs and biologics like TNFi, on the prevalence of CVD. Because risk factors are still underdiagnosed and undertreated, it is imperative that recommendations for care begin by emphasizing the elevated CV risk in AS and PsA. Then we can determine how to prevent these risk factors in the best possible way in such individuals.^51^
But, in the current studies, covariates such as diabetes, hypertension, hyperlipidemia, and hypercholesterolemia were considered, but the smoking status or paraclinical indicators were not evaluated. Considering the above, it is better to investigate the contradictory effect of covariates on the chance of MI and CVA in a study with a longer period and evaluate these covariates one by one to determine the reason for this discrepancy in the studies.
The main limitations of our review are: we only considered studies that were published in the English language, and the data may be contradictory to what is in reality. Also, in some cases, we encountered studies that required payment for downloading which we could not access due to our socioeconomic situation, although the authors of the studies were contacted in various ways (e-mail, ResearchGate, etc.), but we did not receive a response. Of course, it is necessary to state that first of its kind, the current research, we considered the correlation between MI and CVA in patients with AS.
Most studies included in the current review show that people with AS have a higher risk of cerebrovascular disorders than people in the general population. Nonetheless, this risk is influenced by diverse sources like smoking or non-clinical indicators, which need further investigation.
Limitations
We only included the articles that we found online in the aforementioned databases, and we were not aware of unpublished studies and that only articles that were published in English were enrolled in this review.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Joseph P Leong D Mc Kee M , et al. Reducing the global burden of cardiovascular disease, part 1: the epidemiology and risk factors. Circ Res. 2017;121(6):677 694. (10.1161/CIRCRESAHA.117.308903)28860318 · doi ↗ · pubmed ↗
- 2Deaton C Froelicher ES Wu LH Ho C Shishani K Jaarsma T . The global burden of cardiovascular disease. Eur J Cardiovasc Nurs. 2011;10(2):S 5 S 13.21762852 10.1016/S 1474-5151(11)00111-3 · doi ↗ · pubmed ↗
- 3Townsend N Kazakiewicz D Lucy Wright F , et al. Epidemiology of cardiovascular disease in Europe. Nat Rev Cardiol. 2022;19(2):133 143. (10.1038/s 41569-021-00607-3)34497402 · doi ↗ · pubmed ↗
- 4Kim HC . Epidemiology of cardiovascular disease and its risk factors in Korea. Glob Health Med. 2021;3(3):134 141. (10.35772/ghm.2021.01008)34250288 PMC 8239378 · doi ↗ · pubmed ↗
- 5Ding X Wang X Wu J Zhang M Cui M . Triglyceride–glucose index and the incidence of atherosclerotic cardiovascular diseases: a meta-analysis of cohort studies. Cardiovasc Diabetol. 2021;20(1):76. (10.1186/s 12933-021-01268-9)33812373 PMC 8019501 · doi ↗ · pubmed ↗
- 6Buleu F Sirbu E Caraba A Dragan S . Heart involvement in inflammatory rheumatic diseases: a systematic literature review. Medicina (Kaunas). 2019;55(6):249. (10.3390/medicina 55060249)31174287 PMC 6632037 · doi ↗ · pubmed ↗
- 7Aksu K Donmez A Keser G . Inflammation-induced thrombosis: mechanisms, disease associations and management. Curr Pharm Des. 2012;18(11):1478 1493. (10.2174/138161212799504731)22364132 · doi ↗ · pubmed ↗
- 8Tiosano S Yavne Y Gendelman O , et al. Stroke among rheumatoid arthritis patients: does age matter? A real-life study. Neuroepidemiology. 2017;49(3-4):99 105. (10.1159/000481992)29136635 · doi ↗ · pubmed ↗