Diffusion Tensor Imaging in Determining Atypical Peripheral Nerve Neuroma in a Patient with a Painless Mass
Fathinul Fikri Ahmad Saad, Razinul Syamim Fathinul Fikri, Ahmad Danial Ahmad Shahrir

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1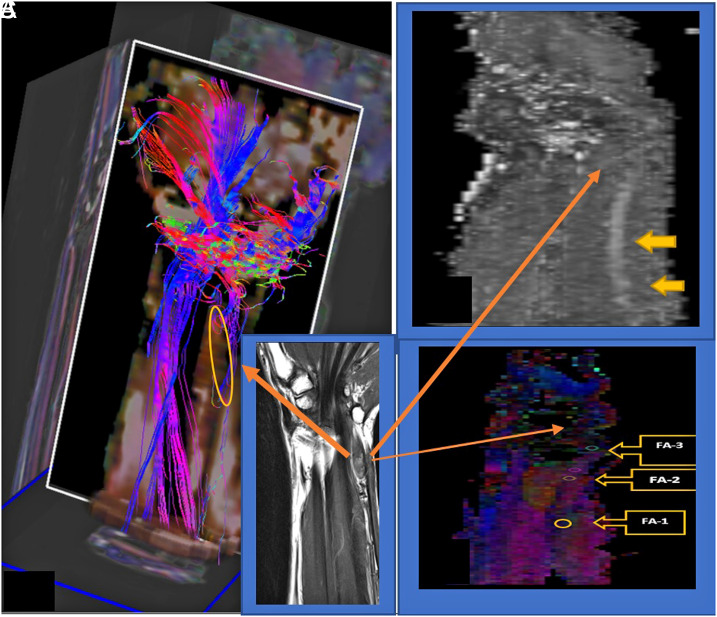 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Neuroimaging Techniques and Applications · Peripheral Nerve Disorders · Elasticity and Material Modeling
To the Editor,
Diffusion tensor imaging (DTI) promises further scrutiny in determining the functional and structural defects of the affected peripheral nerves (PNs) via differences in nerve stiffness and information of early regeneration. The report by Zhang et al^1^ in their study on DTI of axonal and myelin changes in classical trigeminal neuralgia has substantiated that significantly increased fusion anisotropy (FA) is sufficiently sensitive to different pathologic states. In this regard, we emphasize that the reliability of the functional metric of the demyelination in peripheral neuropathy has more favorable credit than conventional diffusion-weighted imaging (DWI) in understanding patients with atypical presentations of the causative factors of peripheral neuropathy. We presented a case of a 71-year-old man who presented with a painless, protracted subcutaneous tissue lump on the medial side of his left forearm, with associated numbness over the first and second web space. The lump was soft and non-tender, with a negative Tinel’s sign on examination. Diffusion tensor imaging scanning protocols were performed on the 3.0 T scanner (Prisma, Siemens Healthineers, Erlangen, Germany), consisting of 13 volumes (45 slices, 128 × 128 voxel, slice thickness 2.2 mm, in-plane voxel size 1.5 mm × 1.5 mm), representing 12 gradient directions and 1 scan with gradient 0 (B0) centered at the left wrist. Echo time (TE) and repetition time (TR) were 93 ms and 8000 ms, respectively. B value was 800 s/mm^2^, 5 scans were k-space averaged online by the Siemens SYNGO operating software. A T1-weighted magnetization-prepared rapid-acquisition gradient echo sequence consisting of 160-200 sagittal partitions depending on head size was used. Written informed consent was obtained from the patient who agreed to take part in the study.
The FA values denoting axonal injury showed reducing values, attributed to the biopsy-proven neuroma tissue (Figure 1).^2-5^ On magnetic resonance imaging, the lesion exhibited an intermediate signal on T1W images and water restriction on the DWI images. The DTI image exhibited a lack of regional nerve ramification and associated functional degeneration on the FA parameter (Table 1). Diffusion tensor imaging enhances the functional characterization of nerve regeneration and tissue microstructure and generates parameters on myelination composite, axonal diameter, fiber density, and organization.^6,7^ There is a limited report on the role of DTI in the atypical presentation of neuroma, for which its utility is deemed essential to ascertain accurate diagnosis and would serve as a potent marker in monitoring neuronal repairs post treatment. Its utility has limitations in standard data acquisition on different scanning models. Motion artifacts and soft tissue edema may affect the accurate delineation of its virtual anatomical mapping for surgical planning. In the future, DTI could constantly improve virtual surgical planning and influence precision in medical therapeutics with progress in artificial intelligence on the mathematical algorithms and savvy use of analytical parameters for researchers on personal computers for end users of varied disciplines.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhang Y Mao Z Cui Z , et al. Diffusion tensor imaging of axonal and myelin changes in classical trigeminal neuralgia. World Neurosurg. 2018;112:e 597 e 607. (10.1016/j.wneu.2018.01.095)29410338 · doi ↗ · pubmed ↗
- 2Naik S Mahanty S Bhoi SK Lahre Y Bag ND Mohakud S. MRI of wrist and diffusion tensor imaging of the median nerve in patients with carpal tunnel syndrome. J Neurosci Rural Pract 2023;14:302. 37181193 10.25259/JNRP_57_2022 PMC 10174157 · doi ↗ · pubmed ↗
- 3Mueller HP Unrath A Sperfeld AD Ludolph AC Riecker A Kassubek J . Diffusion tensor imaging and tractwise fractional anisotropy statistics: quantitative analysis in white matter pathology. Biomed Eng On Line. 2007;6:42. (10.1186/1475-925X-6-42)17996104 PMC 2186341 · doi ↗ · pubmed ↗
- 4Elkholy SF Gadalla AAEH Mohammad ME Mahmoud BE . Diffusion tensor imaging in trigeminal neuralgia: beyond the normal morphology. Egypt J Radiol Nucl Med. 2023;54(1):154. (10.1186/s 43055-023-01102-0) · doi ↗
- 5Wang X Luo L Xing J , et al. Assessment of peripheral neuropathy in type 2 diabetes by diffusion tensor imaging. Quant Imaging Med Surg. 2022;12(1):395 405. (10.21037/qims-21-126)34993088 PMC 8666762 · doi ↗ · pubmed ↗
- 6Heckel A Weiler M Xia A , et al. Peripheral nerve diffusion tensor imaging: assessment of axon and myelin sheath integrity. P Lo S One. 2015;10(6):e 0130833. (10.1371/journal.pone.0130833)26114630 PMC 4482724 · doi ↗ · pubmed ↗
- 7Chhabra A Thakkar RS Andreisek G , et al. Anatomic MR imaging and functional diffusion tensor imaging of peripheral nerve tumors and tumorlike conditions. AJNR Am J Neuroradiol. 2013;34(4):802 807. (10.3174/ajnr.A 3316)23124644 PMC 4629840 · doi ↗ · pubmed ↗