Drug reaction with eosinophilia and systemic symptoms secondary to minocycline complicated by posterior reversible encephalopathy syndrome
Cheney Jianlin Wong, Angelyn Chen Yin Lua, Yong-Kwang Tay, Sze Hwa Tan, Ratna Rajaratnam

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
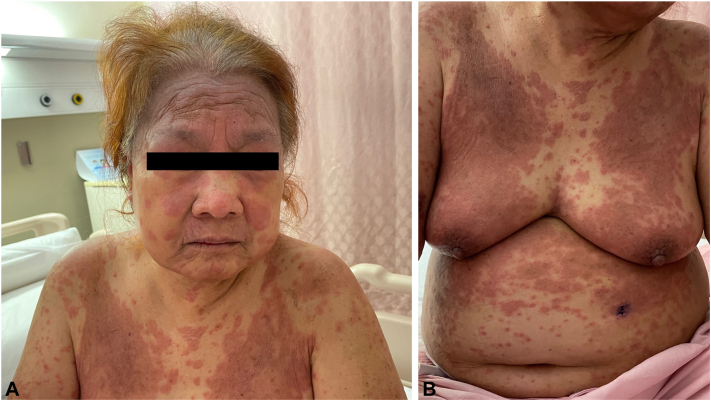 Figure 1
Figure 1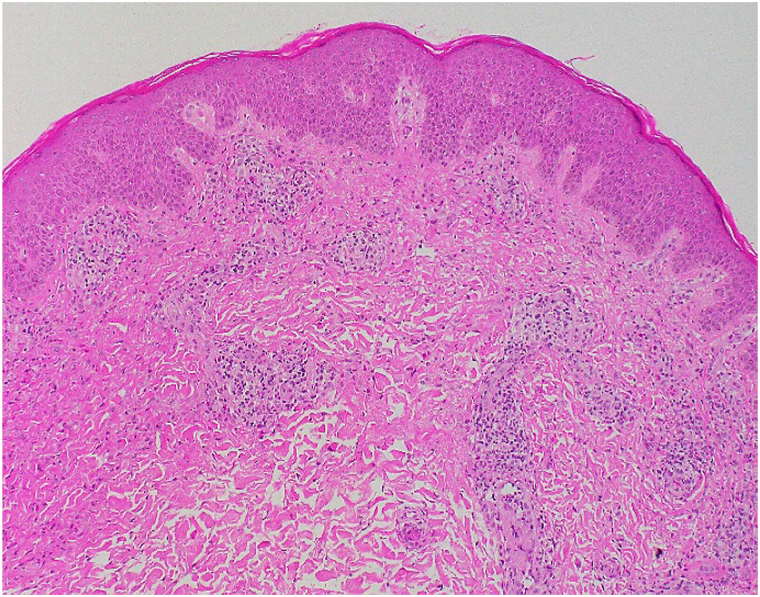 Figure 2
Figure 2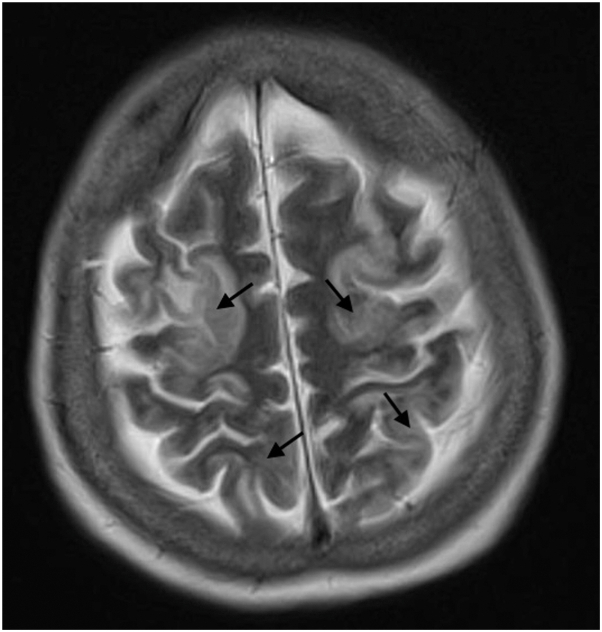 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological Complications and Syndromes · Drug-Induced Adverse Reactions · Methemoglobinemia and Tumor Lysis Syndrome
Introduction
Drug reaction with eosinophilia and systemic symptoms (DRESS) is an uncommon severe cutaneous adverse reaction characterized by fever, eosinophilia, and visceral organ involvement. Neurological involvement is uncommon although manifestations such as meningitis and encephalitis have been described.1
Posterior reversible encephalopathy syndrome (PRES) is a clinicoradiological syndrome characterized by neurological symptoms associated with bilateral white matter edema on neuroimaging. Causes of PRES include hypertensive crises, renal failure, and immunosuppressants.2 In this report, we describe a case of minocycline-associated DRESS complicated by PRES.
Case report
A 71-year-old female presented with a fever of 38.5 °C and generalized pruritic rash of 1 month duration. Examination revealed erythematous urticated papules and plaques on her face, trunk, and limbs (Fig 1). There was mild facial edema but no lymphadenopathy. Blood tests showed acute kidney injury (serum creatinine 331 μmol/L, baseline 87 μmol/L in 2021), eosinophilia (absolute eosinophil count 5.4 × 10^9^/L), an atypical lymphocyte count of 6.0%, and elevated alkaline phosphatase (107U/L). Liver enzymes were otherwise normal.Fig 1A, Confluent urticated plaques on face and chest. B, Confluent urticated plaques on anterior trunk.
Oral minocycline 100 mg daily had been started for chronic lichenified facial dermatitis 34 days prior to admission. She had been taking her other regular medications for at least 1 year. A diagnosis of DRESS was made based on an initial RegiSCAR score of 4 and minocycline was stopped immediately. She was commenced on oral prednisolone 30 mg daily with topical clobetasol propionate 0.05% ointment and mometasone furoate 0.1% ointment to her truncal and facial rashes, respectively.
Autoimmune and viral workup were unremarkable except for a slightly elevated anti-Ro antibody (2.5, normal <1.0) and a positive human herpes virus-6 polymerase chain reaction test (5970 copies/ml). Skin biopsy showed spongiotic and superficial perivascular dermatitis with eosinophilia (Fig 2). Direct immunofluorescence showed granular C3 deposits in the superficial blood vessels.Fig 2. Histopathological exam with hematoxylin and eosin stain (original magnification ×100). The epidermis shows spongiotic changes while the dermis shows perivascular inflammation composed of lymphocytes, histiocytes, and some eosinophils.
She subsequently developed worsening renal function with oliguria and acidaemia, requiring initiation of hemodialysis 5 days after admission. Liver function tests worsened with a cholestatic picture (alkaline phosphatase 247U/L, aspartate aminotransferase 71U/L, alanine aminotransferase 24U/L and gamma-glutamyltransferase 480U/L). She then developed confusion and agitation 1 week into admission which culminated in status epilepticus requiring admission to intensive care. Her blood pressure prior to deterioration was 117/84 mmHg and this increased to 228/116 mmHg at the time of seizure activity. Brain magnetic resonance imaging (MRI) showed extensive T2-hyperintensities involving both cortical and subcortical cerebral regions (Fig 3) and a diagnosis of PRES was made.Fig 3. Brain magnetic resonance imaging (MRI) showing extensive T2-weighted hyperintensities involving both cortical/subcortical cerebral regions (black arrows).
Levetiracetam and phenytoin were started for status epilepticus. Aggressive control of blood pressure was achieved with labetalol, amlodipine, and hydralazine. Her neurological state returned to normal in 1 week and a repeat brain MRI 9 days later showed complete resolution of the widespread T2-hyperintensities. Antiepileptic medications were stopped and she had no further seizures.
Hemodialysis was stopped after 5 weeks due to renal recovery. Liver enzyme abnormalities also resolved completely. Intermittent cutaneous flares were managed with temporary increases of oral prednisolone. She remained well at her 9-month follow-up on a slow taper of oral prednisolone, currently at 10 mg daily.
Discussion
Minocycline is a tetracycline antibiotic used in the treatment of acne vulgaris and dermatitis due to its anti-inflammatory properties.3 Minocycline has been associated with an increased risk of hypersensitivity reactions including DRESS.4 Our patient’s pre-existing dermatitis presented an initial diagnostic dilemma between disease progression and DRESS. However, the temporal relationship with drug initiation, eosinophilia, organ involvement, rash pattern, and skin biopsy findings favored DRESS.
To date, there has been 1 case report describing an association between DRESS and PRES.5 This involved a 68-year-old male patient with stage IV melanoma on treatment with v-raf murine sarcoma viral oncogene homolog B1/mitogen-activated protein kinase inhibitors. He developed headaches, ataxia, blurred vision, and ophthalmalgia 3 weeks after treatment initiation. Brain MRI showed new abnormal T2-hyperintensities in bilateral cerebella supporting a diagnosis of PRES. Four days later, the patient developed fever with a generalized pruritic rash over his trunk and arms. This was associated with acute kidney injury, deranged liver enzymes, and a supportive skin punch biopsy result. A diagnosis of DRESS was made.
There were some differences between our patient and the one described above. Firstly, the onset of DRESS in our patient preceded the development of PRES, whereas DRESS occurred 4 days after the onset of PRES in the other patient. Secondly, v-raf murine sarcoma viral oncogene homolog B1/mitogen-activated protein kinase inhibitors and immunotherapy are known to be independently associated with DRESS and PRES. While minocycline readily crosses the blood-brain barrier and has been reported to cause some neurological side effects such as dizziness and idiopathic intracranial hypertension,6 PRES is not a known adverse reaction. This suggests a likely association with DRESS and its consequential development of acute kidney injury resulting in the symptoms and signs characteristic of PRES.
In conclusion, this case highlights PRES as a possible neurological sequela of DRESS complicated by acute kidney injury. A brain MRI should be considered for patients who develop neurological symptoms in this setting so as to exclude PRES and prevent progression to permanent neurological impairment or death.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shiohara T.Mizukawa Y.Drug-induced hypersensitivity syndrome (Di HS)/drug reaction with eosinophilia and systemic symptoms (DRESS): an update in 2019 Allergol Int 683201930130810.1016/j.alit.2019.03.00631000444 · doi ↗ · pubmed ↗
- 2Shankar J.Banfield J.Posterior reversible encephalopathy syndrome: a review Can Assoc Radiol J 682201714715310.1016/j.carj.2016.08.00528131335 · doi ↗ · pubmed ↗
- 3Garrido-Mesa N.Zarzuelo A.Gálvez J.Minocycline: far beyond an antibiotic Br J Pharmacol 1692201333735210.1111/bph.1213923441623 PMC 3651660 · doi ↗ · pubmed ↗
- 4Ochsendorf F.Minocycline in acne vulgaris Am J Clin Dermatol 115201032734110.2165/11319280-000000000-0000020642295 · doi ↗ · pubmed ↗
- 5Sabile J.M.Grider D.J.Prickett K.A.Li H.Mallidi P.V.Posterior reversible encephalopathy syndrome (PRES) and drug-induced hypersensitivity syndrome (DIHS) following immunotherapy and BRAF/MEK inhibition with continued response in metastatic melanoma Case Rep Oncol Med 202120211510.1155/2021/8845063 PMC 815431134113469 · doi ↗ · pubmed ↗
- 6Chiu A.M.Chuenkongkaew W.L.Cornblath W.T.Minocycline treatment and pseudotumor Cerebri syndrome Am J Opthalmol 1261199811612110.1016/s 0002-9394(98)00063-49683157 · doi ↗ · pubmed ↗