Sharpnel splinter in the common bile duct
Ahmad Abbas, Faiz Al-theab

TL;DR
A 59-year-old man developed jaundice due to a shrapnel splinter in his bile duct, 7 years after a combat injury.
Contribution
This is the first documented case of a shrapnel splinter causing obstructive jaundice in a combat-injured patient from Syria.
Findings
A shrapnel splinter in the common bile duct caused obstructive jaundice 7 years after a combat injury.
This case highlights the need to consider foreign bodies as a cause of jaundice in post-combat injury patients.
Abstract
Foreign bodies are a rare cause of obstructive jaundice. In this case report, we present the case of a 59-year-old male who presented with abdominal pain and obstructive jaundice, which was later found out to be caused by an impacted shrapnel splinter in the common bile duct 7 years after a combat injury. To our knowledge, this is the first documented case from Syria. This case report is a reminder that impacted foreign bodies should be considered as a potential cause of obstructive jaundice in patients with previous combat injury.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
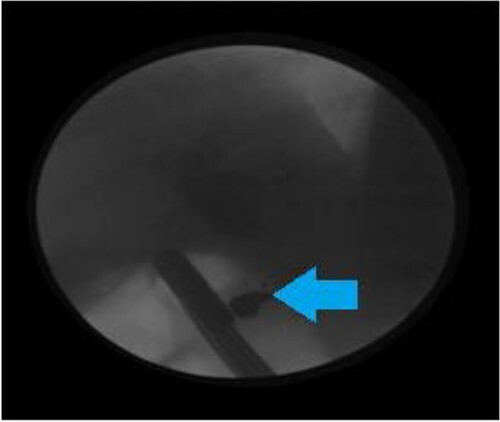 Figure 1
Figure 1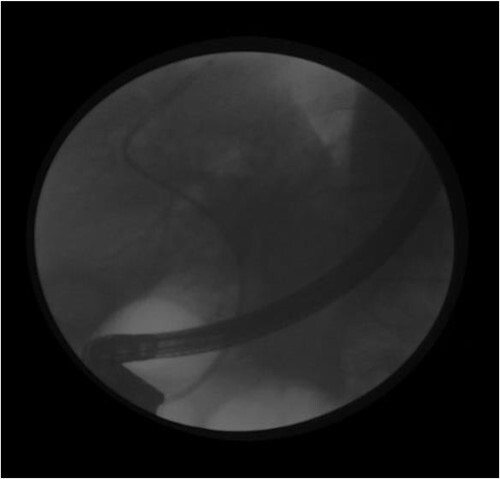 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4|
|
|
|
|
|
|---|---|---|---|---|
| WBC | 6500 | 9800 | 4500–10 500 | /mm3 |
| Hemoglobin | 13.4 | 14 | 12–16 | g/dl |
| Platelets | 132 | 254 | 150–450 | X 1000 |
| Serum Amylase | 1042 | 290 | U/L | |
| Urea | 20 | 15–54 | mg/dl | |
| Creatinine | 0.6 | 0.5–1.3 | mg/dl | |
| ALT | 90 | 5–45 | U/L | |
| AST | 53 | 8–40 | U/L | |
| Total Bilirubin | 6.8 | 0.5–1.2 | mg/dl | |
| Direct Bilirubin | 5.9 | 0–0.3 | mg/dl | |
| Alp | 389 | UP TO 290 | U/L | |
| Ggt | 551 | 0–50 | U/L | |
| Pt/INR | 49%/1.5 | 60%/1.3 | 70% | |
| Glucose | 100 | 105 | 74–106 | mg/dl |
| Crp | 71.3 | 6 | ||
| Na | 132 | 138 | 132–138 | |
| K | 3.3 | 4.1 | 3.5–5 | |
| Ca19-9 | 632 | U/milliliter |
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|
| Eghuchi [ | Icterus, pruritus | Shrapnel splinter | 60/M | Right thoracic cavity | 36 yr |
|
| Kamona [ | Abdominal pain | Bullet | 14/M | Liver parenchyma | 4 mo |
|
| Silvermann [ | Icterus, fever, abdominal pain | Shrapnel | 75/M | RUQ | Initial injury in World War 2 |
|
| Mitchell [ | Fever, weight loss, nausea, vomiting, abdominal pain icteric sclera | Shrapnel splinter | 64/M | RUQ | 44 yr |
|
| Hussain [ | Jaundice, right hypochondrial pain, vomiting, fever, weakness, fatigue and weight loss | Bullet | 26/M | Right lobe of the liver | 9 yr |
|
| Klein [ | Jaundice, abdominal pain | Shell splinter | 44/M | Foramen of winslow | 9 yr |
|
| Rescorla [ | Abdominal pain in RUQ2, Scleral icterus | Bullet | 8/F | Left lobe of the liver | 22 mo |
|
| Krontiris [ | Fever, jaundice, acholic stool, anorexia, malaise, and weakness, abdominal pain in RUQ | Cap of a bullet | 36/M | Right lower thorax | 13 yr |
|
| Gottschalk [ | Abdominal pain and tenderness in RUQ, jaundice | Shell splinter | 69/M | - | 49 yr |
|
| Somi MH [ | Jaundice, abdominal pain in RUQ | Shrapnel splinter | 42/M | RUQ and right thorax | 23 yr |
|
| Present case | Jaundice, pain in the RUQ (right upper quadrant) of the abdomen and epigastrum | Shrapnel splinter | 59/M | Abdomen | 7 yr |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDrug Transport and Resistance Mechanisms · Gallbladder and Bile Duct Disorders · Trace Elements in Health
Introduction
Foreign bodies in the biliary tract are a rare cause of obstructive jaundice. Therefore, they usually do not receive much attention. Such foreign bodies include: T- tubes, vessel clips, fish bones, bullets and sharpnel splinters. This report describes the case of a 59-year-old male who presented with obstructive jaundice caused by an impacted shrapnel in the common bile duct 7 years after the initial injury. To our best knowledge, this is the first documented case from syria. We also report on the findings on Endoscopic Retrograde Cholangiopancreatography (ERCP), discuss the management plan and point out to the idea that shrapnel splinters in the common bile duct should be taken into consideration as a differential diagnosis in patients who present with symptoms suggestive of obstructive jaundice and who have a history of combat injury.
Case presentation
A 59-year-old male presented with a two-week history of jaundice and tenderness in the right upper quadrant (RUQ) of the abdomen and epigastrum, with radiation to the back. He did not suffer from fever or diarrhea, He sustained an abdominal injury during the conflict in Syria, and several sharpnel splinters settled in his abdomen, He has no medical history, and his surgical history extracting a military shrapnel from abdominal cavity, and no history of medication.
On physical examination, the patient had icterus, jaundice, and tenderness in the RUQ. A scar on the abdominal midline was also noted. Lab work was as shown on Table 1.
On abdominal ultrasonography, the gallbladder was normal, and the diameter of the intrahepatic ducts was within normal limits. However, the common bile duct was dilated (diameter = 100 millimeters). Based on the laboratory and radiological findings. Cholangiocarcinoma was suspected.
This dilation was presumed to be the probable cause of the patient’s symptoms. Therefore, we decided to perform a diagnostic (ERCP).
During the ERCP, we noted a filling defect in the proximal portion of the common bile duct (CBD) that was caused by an obstructive object.
The obstructive object roughly measured (6 × 7 millimeters) (Fig. 1).
Endoscopic retrograde cholangiopancreatography showing a foreign body (The arrow) in the CBD before sphincterotomy.
Endoscopic retrograde cholangiopancreatiography after extraction of the foreign body following sphincterotomy and placement of a plastic stent is shown in (Fig. 2).
Endoscopic retrograde cholangiopancreatiography after extraction of the foreign body following sphincterotomy and placement of a plastic stent.
We performed a sphincterotomy and extracted the obstructive object with a post-dilation balloon as shown in (Fig. 3).
The shell splinter as a foreign body (black arrow) in the common bile duct as seen on endoscopic retrograde cholangiopancreatography.
A stone extraction basket was inserted using Esophagogastroduodenoscopy (EGD) as shown in (Fig. 4).
Splinter after extraction by upper Esophagogastroduodenoscopy (EGD).
Discussion
Biliary stones are not the only cause of obstructive jaundice. There are a variety of predisposing factors, such as narrowing of the anastomoses between the biliary tract and the duodenum after surgical interventions, malignant and benign strictures. Foreign bodies in the CBD are a rare cause. However, it should be considered as a cause, especially in people with a history of a combat injury, regardless of the initial entry point of the sharpnel splinters. The entrance point of the shrapnel splinters is not limited to the abdomen. There have been cases where the entry point was the thoracic cavity [1].
Although, obstructive jaundice is the most common symptom of foreign bodies in the CBD, symptoms may be limited to abdominal pain [2].
Chronic obstruction of the biliary tract may be complicated by sclerosing cholangitis [3].
We note from the cases shown in Table 2 that symptoms caused by foreign bodies in the CBD has a latency period ranging from months to years before they appear.
Foreign bodies in the CBD may sometimes present with symptoms indicative of malignancy such as weight loss [4, 5]. In our case, the patient had elevated CA 19-9 levels.
Summary
Foreign bodies in the biliary tract that cause of obstructive jaundice miscellaneous, that a missed gauze in the abdominal cavity after surgery on abdominal cavity, Therefore, it is important to take the patient’s medical history carefully to determine the cause of obstructive jaundice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Eguchi S , Matsuo S, Hidaka M. et al. Impaction of a shrapnel splinter in the common bile duct after migrating from the right thoracic cavity: report of a case. Surg Today 2002;32:383–5.12027209 10.1007/s 005950200058 · doi ↗ · pubmed ↗
- 2Kamona A , Mansour A, Qandeel M. et al. Biliary obstruction secondary to combat-related foreign bodies: report of two cases. Abdom Imaging 2005;30:748–9.16252146 10.1007/s 00261-005-0325-5 · doi ↗ · pubmed ↗
- 3Silverman WB . Sclerosing cholangitis caused by old shrapnel injury. Gastrointest Endosc 2003;58:420.14528222 10.1067/s 0016-5107(03)00022-1 · doi ↗ · pubmed ↗
- 4Mitchell R, Kerr R, Barton J, Schmidt A . Biliary obstruction secondary to shrapnel. American Journal of Gastroenterology (Springer Nature). 1991;86.1928051 · pubmed ↗
- 5Hussain SM , Zulqurnain S, Saleem O. Delayed obstructive jaundice secondary to bullet in common hepatic duct. J Coll Physicians Surg Pak 2007;17:232–3.17462186 · pubmed ↗
- 6Klein E , Schneebaum S, Feuchtwanger MM. et al. Shell splinter in the common bile duct: a rare cause of obstructive jaundice. Am J Surg 1981;141:376–7.7011079 10.1016/0002-9610(81)90200-2 · doi ↗ · pubmed ↗
- 7Rescorla FJ , Schlatter M, Hawes RH. et al. Delayed presentation of a penetrating biliary tract injury in a child. J Trauma Acute Care Surg 1996;40:157–8.10.1097/00005373-199601000-000358576986 · doi ↗ · pubmed ↗
- 8Krontiris A , Tsironis A. Common duct obstruction by a bullet compression cap: a rare case. Ann Surg 1962;156:303–6.14459844 10.1097/00000658-196208000-00017 PMC 1466345 · doi ↗ · pubmed ↗