Levofloxacin-Induced Arthralgia in Multidrug-Resistant Tuberculosis Patients: A Case Series Spanning Three Age Groups
Shaily KP, Manosri Mandadi

TL;DR
This paper reports three cases of joint pain caused by levofloxacin in multidrug-resistant tuberculosis patients across different age groups in India.
Contribution
The study adds to the limited Indian literature on levofloxacin-induced arthralgia in MDR-TB patients.
Findings
Three MDR-TB patients experienced arthralgia while on levofloxacin treatment.
Patients were managed by rechallenging or switching to alternative drugs based on weight bands.
Arthralgia is a rare but notable adverse effect of levofloxacin in MDR-TB treatment.
Abstract
Multidrug-resistant TB (MDR-TB) is a form of tubercular disease caused by a strain of Mycobacterium tuberculosis complex that is resistant to rifampicin and isoniazid. Microbiologically diagnosed patients are started on an all-oral longer regimen or shorter regimen based on the Guidelines on Programmatic Management of Drug Resistant TB (PMDT) in India. Fluoroquinolones (FQs), being the cornerstone in the treatment of MDR-TB, are categorized as class A drugs. Levofloxacin (Lfx) administered at a dose of 11-14 mg/kg/day holds a strong bactericidal activity against Mycobacterium tuberculosis. FQs are associated with a wide range of adverse drug reactions, such as nausea, bloating, headache, dizziness, and insomnia. Tendon rupture, arthralgia though rare, can also occur due to Lfx. Even though arthralgia is commonly seen in patients on Lfx-associated treatment, only a few cases have been…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
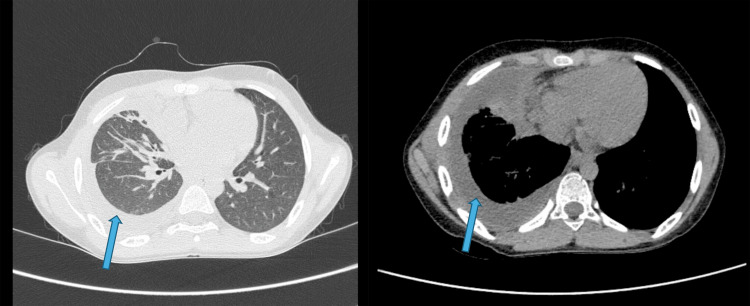 Figure 1
Figure 1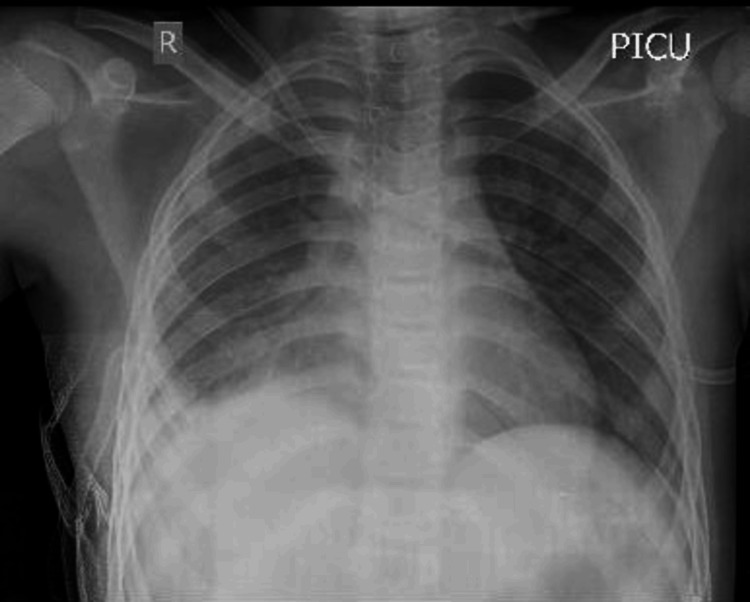 Figure 2
Figure 2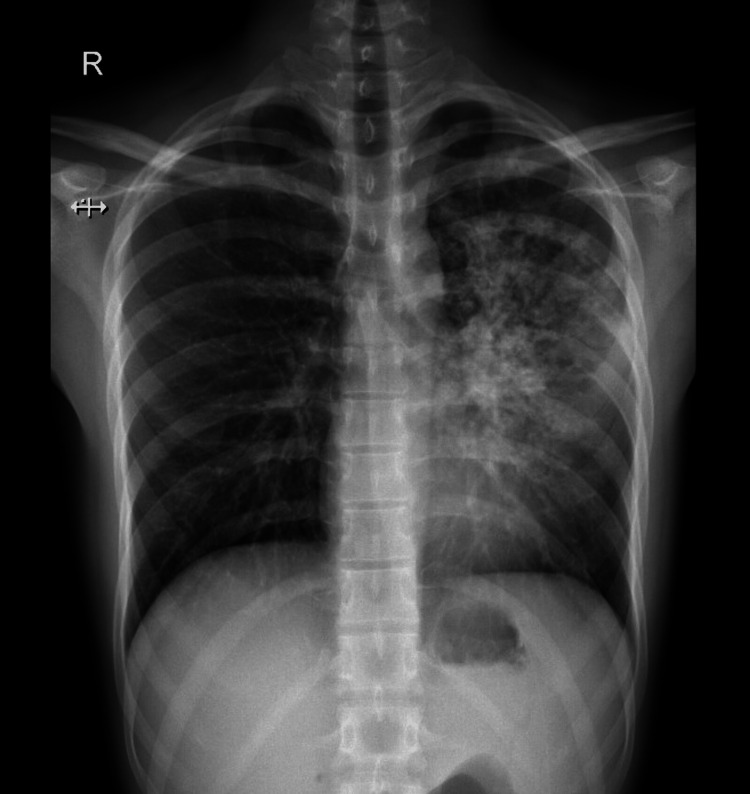 Figure 3
Figure 3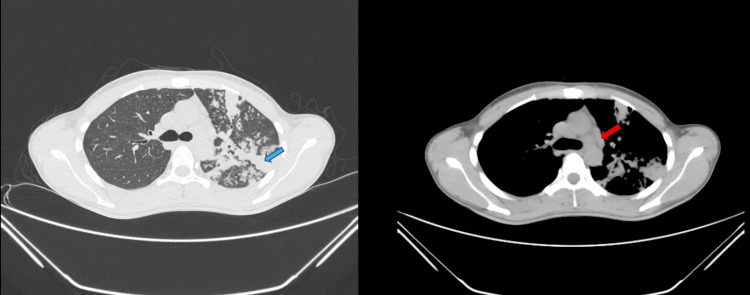 Figure 4
Figure 4 Figure 5
Figure 5| Variable | Result | Biological reference interval |
| Physical | ||
| Color | Reddish, turbid | - |
| Cobweb/coagulum | Absent | Absent |
| Deposits | Present | Absent |
| Chemical | ||
| Proteins, by biuret method | 1.30 | Upto 3gm% |
| Glucose | 10 | >60 mg/dl |
| Microscopy | ||
| RBCs | Many | Absent |
| Total leucocyte count | 350 | 0-150 per cmm |
| Polymorphs/neutrophils | 10 | % |
| Lymphocytes | 85 | % |
| Mesothelial/macrophages | 5 | % |
| Pleomorphic cells | 0 | % |
| LDH | 667 U/L | |
| ADA | 6.03 U/L |
| Sample | Result |
| Pleural fluid culture (aerobic) | No acid-fast bacilli seen; no growth of microorganisms |
| Pleural fluid CBNAAT | MTB – not detected |
| Histopathological examination of lung tissue | Section showed fibro-collagenous tissue, granulation tissue, and many epithelioid granulomas mixed with lymphocytes and foreign body and langhans giant cells. Few granulomas showed central caseous necrosis – suggestive of likely tubercular lesion |
| Lung biopsy - molecular TB/DST result (line probe assay) | MTB complex detected in PCR resistant to rifampicin and isoniazid |
| Lung biopsy - CBNAAT | MTB high detected with rifampicin resistance |
| Sputum CBNAAT | MTB - not detected |
| Sample | Result |
| Sputum CBNAAT | MTB high detected with rifampicin resistance |
| Sputum AFB - samples A and B | Positive for AFB (2+) |
| Sputum culture | AFB seen; no growth of microorganisms |
| Sample | Result |
| Sputum AFB - samples A and B | Positive for AFB (3+) |
| Sputum CBNAAT | MTB high detected with rifampicin resistance |
| Sputum culture | No growth of microorganisms |
| Normal reference interval | Case 1 | Case 2 | Case 3 | |
| Uric acid | 3.70-8 mg/dL | 2.1 | 3.4 | 3 |
| ESR | 0-22 mm/hr for males; 0-29 mm/hr for females | 21 | 10 | 18 |
| CRP | <0.9 mg/dL | 0.2 | 0.3 | 0.2 |
| Anti-CCP | <5 U/mL: negative; ≥5 U/mL: positive | - | Negative (0.5) | Negative (0.6) |
| RA factor | <15 IU/mL | - | Negative (9.25) | Negative (9.0) |
| Age, years | Gender | Presenting symptoms | The onset of symptoms after initiation of the regimen | Pain score (on a scale of 0-10) | Peak of symptom | Previous use of Lfx | Duration of NSAID use | Management steps taken | Reoccurrence of symptoms (after rechallenging the drug) | Outcome |
| 10 (young) | Male | Severe knee pains, difficulty standing from sitting position | 1 month | 7 | 10 days | No | 4 days | Withheld Lfx, joint rest, NSAIDs, rechallenged with Lfx | Yes | Switched to pyrazinamide |
| 33 (middle-aged) | Male | Joint pain in multiple small and large joints, stiffness | 1.5 months | 6 | 15 days | No | 4 days | Withheld Lfx, joint rest, NSAIDs, rechallenged with Lfx | No | Continued levofloxacin |
| 63 (elderly) | Female | Joint pains, inability to carry out daily activities | 1 month | 6 | 20 days | No | 4 days | Withheld Lfx, joint rest, NSAIDs, rechallenged with Lfx | Yes | Switched to pyrazinamide |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Infectious Diseases and Tuberculosis · Antibiotics Pharmacokinetics and Efficacy
Introduction
Multidrug-resistant TB (MDR-TB) is a form of tuberculosis (TB) disease caused by a strain of the Mycobacterium tuberculosis complex that is resistant to rifampicin and isoniazid [1]. Impacting nearly 410,000 people worldwide in 2022, MDR-TB poses a significant and escalating global health threat [1]. TB is curable if diagnosed and treated promptly, making accurate and rapid detection crucial for reducing disease transmission within communities [2]. Cartridge-based nucleic acid amplification test (CBNAAT) plays a vital role in diagnosing MDR-TB [2]. This test, based on reverse transcription-polymerase chain reaction (RT-PCR), can detect both TB and rifampicin resistance (RR) within two hours [2]. Since over 90% of RR bacteria are also resistant to isoniazid, RR serves as a surrogate marker for MDR-TB [2].
Patients with no bacteriological evidence of TB but with clinical symptoms suggestive of the disease can be started on antitubercular treatment based on radiological evidence [3]. High-resolution CT (HRCT) of the thorax plays an important role in the radiological diagnosis of TB [3]. The common radiological findings of pulmonary tuberculosis include centrilobular nodules, branching linear and nodular opacities (tree-in-bud appearance), patchy or lobular areas of consolidation, and thick-walled multiple cavities [3]. Individuals diagnosed with rifampicin-resistant TB (RR-TB), isoniazid-resistant TB, and MDR-TB require regimens that include drugs such as fluoroquinolones (FQs), bedaquiline, linezolid, cycloserine, and clofazimine [4]. The regimens for MDR-TB are more expensive and cause more side effects when compared to the first-line regimens for drug-susceptible TB [4].
Accounting for a crucial component in the treatment of MDR-TB, FQs such as levofloxacin (Lfx) and moxifloxacin are categorized as class A drugs [5]. Lfx is typically administered for tuberculosis at doses of 11-14 mg/kg/day and has been well tolerated up to a dose of 20 mg/kg [5]. It holds strong bactericidal activity and involves inhibition of deoxyribonucleic acid gyrase [6]. FQs demonstrate a wide range of adverse reactions, such as nausea, bloating, headache, dizziness, insomnia, and tremors [6,7]. Though rare, musculoskeletal complications such as tendon rupture and arthralgia can occur due to Lfx; the latter is frequently treatable with symptomatic therapy [7]. Only a small number of cases of arthritis and arthralgia have been documented to date in India [8]. In this case series, we highlight a neglected adverse drug reaction (ADR) of levofloxacin-arthralgia in patients from different age groups who were started on an all-oral longer regimen for MDR-TB.
Case presentation
Case 1
A 10-year-old male presented with complaints of fever and breathlessness for two months. Chest X-ray and HRCT thorax showed right-sided moderate pleural effusion with pleural thickening and underlying atelectasis (Figure 1). Pleural fluid analysis proved to be exudative lymphocytic-predominant (Table 1). The patient underwent right-sided decortication under video-assisted thoracoscopic surgery given his empyema (Figure 2). He was microbiologically diagnosed as MDR-TB through CBNAAT and the line probe assay of the lung biopsy sample (Table 2). Based on the inclusion and exclusion criteria, he was started on an all-oral longer regimen (bedaquiline, levofloxacin, clofazimine, cycloserine, linezolid, and pyridoxine) based on his weight of 30 kg.
HRCT thorax - case 1The images show moderate right-sided pleural effusion (blue arrows) with thickening of pleura and atelectatic changes in the right lower lobe and anterior segment of the right upper lobe suggestive of empyemaHRCT: high-resolution computed tomography
Post-decortication chest X-ray anteroposterior view - case 1The image shows the right intercostal drainage tube in situ
One month after the initiation of the regimen, the patient reported complaints of difficulty standing from a sitting position due to severe knee pains. Further evaluation revealed normal uric acid, C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR). The child was prescribed non-steroidal anti-inflammatory drugs and advised to withhold Lfx. After the resolution of symptoms, the tablet Lfx was restarted. Initially, a low dose of 500 mg Lfx was given for three days, followed by a full dose of 750 mg. During follow-up in the outpatient unit, the patient experienced a recurrence of symptoms, confirming our diagnosis of levofloxacin-induced arthralgia. Consequently, the child was switched to the next drug in the replacement sequence, pyrazinamide, based on their weight band.
Case 2
A 33-year-old male, treated for drug-sensitive pulmonary tuberculosis one year ago, presented with complaints of fever, and cough associated with weight loss of 8 kgs in the previous two months. On further investigation, the patient’s sputum CBNAAT revealed MTB high detected with rifampicin resistance (Table 3); imaging of the chest showed large dense consolidation with air-bronchogram with multiple centrilobular nodules in the superior segment of the left lower lobe and upper lobe (Figures 3-4).
Chest X-ray posteroanterior view - case 2The image shows diffuse heterogeneous opacities noted in the left upper and lingular lobe
HRCT thorax - case 2The images show a large dense consolidation with an air bronchogram in the left upper lobe (blue arrow). Mediastinal lymphadenopathy was noted (red arrow)HRCT: high-resolution computed tomography
Upon diagnosis, the patient was started on an all-oral longer regimen; 1.5 months later, he presented to our outpatient unit with joint pain involving small and large joints. During a detailed history, the patient reported stiffness in multiple joints for varying durations with no postural or diurnal variation, which was associated with restrictions to work since the last 15-20 days post-initiation of the drug-resistant TB regimen. He was admitted and worked up for arthritis - rheumatoid arthritis (RA), anti-cyclic citrullinated peptide (anti-CCP), uric acid levels, and inflammatory markers (ESR and CRP) - which were found to be normal. Meanwhile, due to high suspicion, tablet Lfx was stopped while other drugs in the regimen were continued. During this period, the patient was given a non-steroidal anti-inflammatory drug (NSAID). After a significant reduction in the symptoms, the patient was gradually rechallenged on a low dose of levofloxacin, followed by the full dose of levofloxacin reintroduced on day four of desensitization. The patient was closely monitored, and on follow-up, no resurfacing of symptoms related to arthralgia was reported.
Case 3
A 63-year-old female presented with initial symptoms of cough with expectoration and fever of one month's duration. Chest radiography of the patient showed, diffuse homogenous opacification noted in the left upper lobe obscuring the left heart border (Figure 5). Through sputum sample analysis, she was diagnosed with MDR-TB (CBNAAT - MTB high detected with rifampicin resistance) (Table 4). She was started on an all-oral longer regimen based on inclusion and exclusion criteria. She presented to us after one month of treatment initiation with a 10-day history of joint pains and complained that she was unable to carry out her daily activities.
Chest X-ray posteroanterior view - case 3The image shows diffuse homogenous opacification noted in the left upper lobe obscuring the left heart border
The patient was evaluated for other causes of arthritis and was asked to withhold levofloxacin as per guidelines. After one week, she was restarted on a low dose of levofloxacin of 500 mg, followed by the full dose. The patient reported a reemergence of symptoms after restarting the drug. Subsequently, a collective decision was made to switch levofloxacin to the next drug in the replacement sequence, pyrazinamide. Amikacin and delamanid were not chosen given the age and the financial factors of the patient as well as feasibility. The patient was comfortable with the new regimen and is currently being closely monitored for any new side effects.
Table 5 presents the biochemical marker tests done to rule out arthritis in all cases, while Table 6 provides a summary of all cases and their management.
Discussion
In this case series, we discussed the cases of three MDR-TB patients of different age groups (young, middle-aged, and older) who were started on an all-oral longer regimen. In a descriptive study, Huruba et al. reported that the most common ADRs associated with FQs were arthralgia, most commonly seen with Lfx [9]. These ADRs were mostly reported between one and seven days, extending up to 30 days, and no recurrence of the symptoms was observed in the majority of the cases who were rechallenged with the drug [9].
Desensitization refers to the idea of building tolerance to a sensitized drug by administering slow increments of the drug, starting with a very small amount and gradually progressing to a full therapeutic dose [10]. Desensitization can be classified into two categories; slow drug desensitization(SDD) and rapid drug desensitization (RDD) [10]. SDD is recommended for type IV delayed hypersensitivity reaction and has shown better success rates [10]. Whereas, our patients after nearly four weeks of treatment, developed new-onset symptoms such as multiple joint pains, significantly hindering their daily activities. There were no identified alternative exposures, including other medications, to which the changes were attributable. To rule out other causes of arthralgia, these patients were worked up, and all the radiological and laboratory parameters were found to be within normal limits.
As per the Guidelines for Programmatic Management of Drug-Resistant Tuberculosis in India-2021 [11], due to the high suspicion of levofloxacin being the culprit drug, it was withheld for three to seven days. During this period, the patients were advised to have adequate joint rest and started on NSAIDs with sufficient hydration [11]. Significant symptom relief was noted by all the patients after discontinuing levofloxacin. After a symptom-free period, levofloxacin was gradually reintroduced at a low dose for three days, followed by the full dose at 11-14 mg/kg. Patients were monitored over the next month. Two of the three patients experienced the same symptoms upon rechallenging with the drug, confirming levofloxacin as the cause of arthralgia. Hence, these patients were switched to pyrazinamide according to the replacement sequence protocol.
Conclusions
This case series discussed the occurrence of Lfx-induced arthralgia in MDR-TB patients across various age groups (pediatric, adult, and geriatric) following the initiation of an all-oral longer regimen. Lfx, a fluoroquinolone, is pivotal in MDR-TB treatment due to its potent bactericidal activity but can cause significant adverse effects, including arthralgia. The temporal relationship between drug administration and symptom onset, along with symptom recurrence upon rechallenge, confirmed the adverse reaction to the drug. These findings highlight the importance of providing comprehensive counseling to patients about the potential adverse effects of their prescribed medication regimen. Prompt decisions regarding the continuation of levofloxacin or its replacement with other drugs should be taken. Additionally, vigilant monitoring for Lfx-induced arthralgia is crucial, regardless of patient age, to enhance treatment adherence and efficacy in MDR-TB therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tuberculosis: multidrug-resistant (MDR-TB) or rifampicin-resistant TB (RR-TB) 6 2024 2024 https://www.who.int/news-room/questions-and-answers/item/tuberculosis-multidrug-resistant-tuberculosis-(mdr-tb)
- 2Role of Gene Xpert or CBNAAT in diagnosing tuberculosis: present scenario Med J DY Patil Univ Garg A; Agarwal L Rishab M 1419152022 https://journals.lww.com/mjdy/fulltext/2022/15010/role_of_genexpert_or_cbnaat_in_diagnosing.6.aspx
- 3Radiological findings of extensively drug-resistant pulmonary tuberculosis in non-AIDS adults: comparisons with findings of multidrug-resistant and drug-sensitive tuberculosis Korean J Radiol Cha J Lee HY Lee KS 2072161020091941250810.3348/kjr.2009.10.3.207PMC 2672175 · doi ↗ · pubmed ↗
- 4Drug-resistant TB: treatment 6 2024 2021 https://www.who.int/publications/digital/global-tuberculosis-report-2021/tb-diagnosis-treatment/drug-resistant-treatment
- 5Levofloxacin pharmacokinetics, pharmacodynamics and outcome in multidrug-resistant tuberculosis patients Eur Respir J Ghimire S Maharjan B Jongedijk EM 262853201910.1183/13993003.02107-201830655280 · doi ↗ · pubmed ↗
- 6Review article levofloxacin: a potent antibiotic introduction Journal of Baqai Medical University. 6 2024 Bano Bano Rahila &Arsalan Adeel &Shahnavi Iqbal &Shad Zufi.Zufi. 2011 https://www.researchgate.net/publication/259707126_REVIEW_ARTICLE_LEVOFLOXACIN_A_POTENT_ANTIBIOTIC_INTRODUCTION
- 7World Health Organization: Companion handbook to the WHO guidelines for the programmatic management of drug-resistant tuberculosis World Health Organization 7 2024 World Health Organization 452Global Tuberculosis Programme (GTB)2014 https://www.who.int/publications/i/item/978924154880925320836 · pubmed ↗
- 8Rheumatological side-effects of quinolones Baillieres Clin Rheumatol Ribard P Kahn MF 17519151991164900910.1016/s 0950-3579(05)80301-2 · doi ↗ · pubmed ↗