Undifferentiated Carcinoma of the Pancreas With Osteoclast-Like Giant Cells: A Grave Oncologic Diagnosis
Clive Jude Miranda, Eric John Dove, Farhan Azad

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
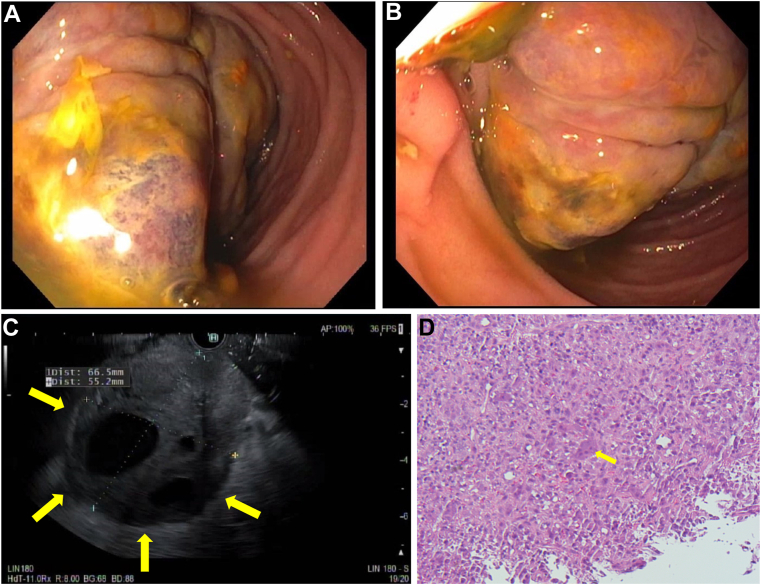 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Bone health and treatments · Cancer Diagnosis and Treatment
A 51-year-old male with no gastrointestinal history presented with a 50lb weight loss, severe abdominal pain, and vomiting. Physical exam revealed a tender, firm epigastric nodule, and bloodwork was grossly normal, including CA-19-9 and carcinoembryonic antigen markers. Computed tomography revealed fat stranding around the pancreatic head and portal vein, superior mesenteric vein thrombosis, and peripancreatic adenopathy. There was a large mass in the third portion of the duodenum encasing branches of the superior mesenteric artery with gastric dilatation. An esophagogastroduodenoscopy with endoscopic ultrasound showed a 67 × 60 mm fungating villous mass with cystic components in D3 extending proximally to the stomach with intrinsic stenosis of the second portion of the duodenum (Figure A–C). Biopsy showed undifferentiated carcinoma of the pancreas with osteoclast-like giant cells (Figure D), which stained negative for CK7/CAM5.2 (seen in pancreatic ductal adenocarcinoma) and positive for CD68/vimentin (seen in osteoclast-like giant cells). Given his poor prognosis, a shared decision was made to transition him to hospice care. Undifferentiated carcinoma of the pancreas with osteoclast-like giant cells accounts for less than 1% of all pancreatic malignancies, is typically diagnosed at advanced stages, and is thereby frequently unresectable. Surgical resection is often first performed; however, optimal management is still consensus.