Anogenital Erosive Lichen Sclerosus in a Male With Multiple Autoimmune Conditions
Mohammad I Fardos, Jacqueline Nikakis, Sophia Anagnostis, Summer Moon

TL;DR
This paper reports a rare case of treatment-resistant lichen sclerosus in a male with multiple autoimmune disorders, emphasizing the challenges in managing the condition.
Contribution
The novelty lies in presenting a rare case of LS in an unusual location with a complex autoimmune background.
Findings
Lichen sclerosus occurred in the intergluteal cleft, a rare location for the condition.
The patient had multiple autoimmune disorders, including porphyria cutanea tarda, discoid lupus, and Sjogren's syndrome.
Treatment with corticosteroids and topicals failed, highlighting the need for alternative approaches.
Abstract
Lichen sclerosus (LS) is a chronic inflammatory disorder primarily affecting the anogenital region, with a higher prevalence in females and often linked to autoimmunity. This association is not clearly elucidated in males, with LS commonly presenting in uncircumcised males. The most affected areas include the glans penis, prepuce, and coronal sulcus. In this report, we present an 11-year case of treatment-resistant LS in a male patient with an extensive history of autoimmune disorders, manifesting in the intergluteal cleft as a hypertrophic plaque, a rare location. The patient had a complex autoimmune history, including porphyria cutanea tarda, discoid lupus, and Sjogren's syndrome. Histopathological analysis confirmed a diagnosis of erosive LS. Despite numerous treatments, including intralesional corticosteroids and various topicals, the lesion persisted. This case highlights the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
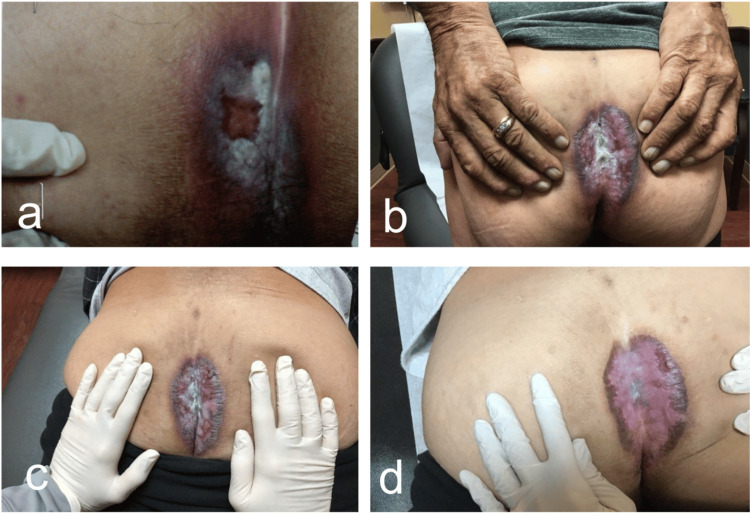 Figure 1
Figure 1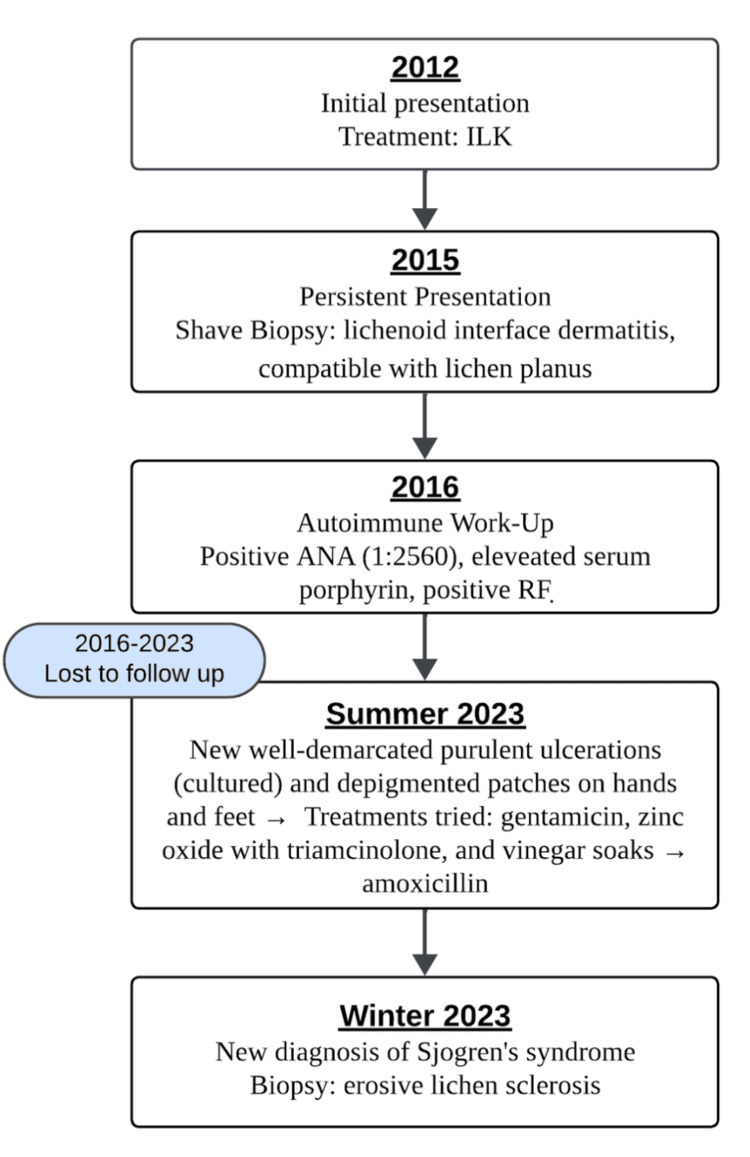 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenital Health and Disease · Urologic and reproductive health conditions · Urological Disorders and Treatments
Introduction
Lichen sclerosus (LS) is a chronic inflammatory condition that typically affects the anogenital region [1]. LS predominantly affects females at a ratio of 5:1 and is associated with autoimmune diseases such as autoimmune thyroid disease, vitiligo, and psoriasis [2]. This association is not clearly elucidated in males, with LS commonly presenting in uncircumcised males. The most commonly affected areas in males include the glans penis, prepuce, and coronal sulcus [2]. Here, we present a case of treatment-refractory LS in a male patient with an extensive autoimmune history, occurring in the intergluteal cleft, a unique location.
Case presentation
A 56-year-old African American man presented in the summer of 2023 with a chief complaint of a rash affecting his intergluteal cleft, which had been present for the past eleven years. His past medical history was significant for porphyria cutanea tarda (PCT) and discoid lupus erythematosus (DLE), both diagnosed in 2012. The patient's DLE was treated with topical corticosteroids, and his PCT was managed with phlebotomy.
Historically, the patient was initially evaluated in the spring of 2012 for an intensely pruritic rash of his intergluteal cleft. A shave biopsy at that time revealed lichen simplex chronicus. He was treated with 5 mg of intralesional Kenalog (ILK), high-potency topical corticosteroids, topical calcineurin inhibitors, and zinc barrier cream, with minimal improvement. Due to persistent symptoms, the patient had a repeat shave biopsy in 2015, which revealed lichenoid interface dermatitis, compatible with lichen planus. Further autoimmune work-up in 2016 revealed a positive antinuclear antibody (ANA) titer, positive rheumatoid factor, and elevated serum porphyrin levels. The patient was further evaluated by rheumatology, and systemic lupus and rheumatoid arthritis were ruled out. The patient was lost to follow-up between 2016 and 2023 before presenting again in the summer of 2023. Systemic treatment with hydroxychloroquine was considered at that time but ultimately not started due to patient preferences.
In the summer of 2023, physical examination revealed a hypertrophic and lichenified plaque on the left gluteal fold, approximately 7 to 8 cm in diameter (Figures 1 and 2). The patient reported associated intense pruritus. A shave biopsy was performed, which revealed parakeratosis with crust overlying the epidermis, along with acanthosis featuring hypergranulosis and necrotic keratinocytes at the base. Furthermore, a dense dermal infiltrate predominantly composed of lymphocytes was noted. The Fite, PAS (periodic acid-Schiff), and GMS (Gomori methenamine-silver) stains were negative. Collectively, these findings were suggestive of erosive LS. The patient had a repeated rheumatology work-up, which revealed a positive ANA titer with a speckled pattern, and was diagnosed with Sjogren’s syndrome. The patient was started on ILK 10 mg with improvement in pruritus in the winter of 2023. However, due to the persistent hypertrophic plaque despite multiple treatments with ILK and various topical therapies, the patient is now being considered for systemic hydroxychloroquine treatment. The patient has not been treated with systemic therapies for any of his autoimmune diseases, including DLE, PCT, and Sjogren's syndrome.
Progression of Perianal Plaque(a) Spring of 2012; (b) summer of 2023 showing a well-demarcated plaque; (c) fall of 2023; (d) winter of 2024: hypertrophic and lichenified plaque on the left gluteal fold, approximately 7 to 8 cm in diameter.
Timeline detailing disease progressionILK: intralesional Kenalog, ANA: antinuclear antibody, RF: rheumatoid factor.
Discussion
Treatment goals in LS aim to alleviate symptoms, improve appearance, and prevent disease progression and complications. Topical therapies play a crucial role in managing anogenital LS. High-potency topical corticosteroids are first-line medications for LS due to their robust anti-inflammatory effects, effectively mitigating pruritus, pain, and inflammation. Alternatively, calcineurin inhibitors, specifically tacrolimus and pimecrolimus, have demonstrated high efficacy in treating LS in instances where corticosteroids are contraindicated [3]. In addition to topical therapies, localized steroid injections may be utilized to manage thicker lichenified plaques.
In cases refractory to topical treatment, systemic modalities may be considered; however, there are no established guidelines. A review of 71 studies encompassing 392 LS patients, including those with anogenital (254), extragenital (36), and both types (73) of LS, found that systemic therapies such as oral retinoids, methotrexate, hydroxychloroquine, and systemic steroids resulted in clinical or symptomatic improvement in a significant proportion of patients [3]. Notably, 76% of patients with anogenital involvement and 81% of patients with both types of LS experienced improvements following systemic treatment [4]. Despite these findings, established guidelines for systemic LS treatment remain lacking.
Hydroxychloroquine may be useful in the treatment of our patient's treatment-resistant anogenital LS as well as other concurrent autoimmune diseases, including DLE, PCT, and Sjogren's syndrome.
Conclusions
This case underscores the rarity of LS manifesting in a male patient with an extensive autoimmune history and occurring in a unique location, the intergluteal cleft. It additionally highlights the challenges posed by treatment-resistant LS. Despite various treatment attempts, including topical corticosteroids and intralesional injections, the plaque persisted. While topical therapies remain the cornerstone of treatment, systemic options such as hydroxychloroquine may offer promise in refractory cases, although clear guidelines are currently lacking. Further investigation is warranted to elucidate optimal management strategies for erosive LS, particularly in patients with complex autoimmune backgrounds like the one presented here.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The clinical spectrum of lichen sclerosus in male patients - a retrospective study Acta Derm Venereol Kantere D Löwhagen GB Alvengren G Månesköld A Gillstedt M Tunbäck P 5425469420142454923910.2340/00015555-1797 · doi ↗ · pubmed ↗
- 2Humoral and cell-mediated autoimmunity in lichen sclerosus Br J Dermatol Gambichler T Belz D Terras S Kreuter A 1831841692013 https://doi.org/10.1111/bjd.122202330178010.1111/bjd.12220 · doi ↗ · pubmed ↗
- 3Evidence-based (S 3) guideline on (anogenital) Lichen sclerosus J Eur Acad Dermatol Venereol Kirtschig G Becker K Günthert A 04329201510.1111/jdv.1313626202852 · doi ↗ · pubmed ↗
- 4Systemic therapy for lichen sclerosus: a systematic review J Low Genit Tract Dis Hargis A Ngo M Kraus CN Mauskar M 84902820243792426010.1097/LGT.0000000000000775 · doi ↗ · pubmed ↗