New-Onset Occipital Lobe Epilepsy in an Elderly Patient With Visual Hallucinations and Hemianopia
Katarina Milosavljevic, Yong Eun, Pooja Roy, Salama Fawzy

TL;DR
An elderly man with visual hallucinations and hemianopia was diagnosed with occipital lobe epilepsy, highlighting the need for careful evaluation to avoid misdiagnosis.
Contribution
This case study emphasizes the diagnostic challenges of OLE and its distinction from similar neurological conditions.
Findings
The patient exhibited visual hallucinations and hemianopia consistent with occipital lobe epilepsy.
MRI and MRA ruled out stroke but showed cerebral atrophy and microvascular changes.
Treatment with levetiracetam and lorazepam reduced seizure frequency.
Abstract
Occipital lobe epilepsies (OLEs) are a subset of epileptic disorders manifesting predominantly with visual and oculomotor abnormalities that are often misdiagnosed due to similarities with migraines with visual aura and other central nervous system (CNS) pathologies. This case study describes an 88-year-old male with a three-week history of intermittent kaleidoscopic visual phenomena, accompanied by blurring of vision and altered level of consciousness. Neurological examination revealed right homonymous hemianopsia and focal neurological deficits, including forced right gaze preference and nystagmus. Diagnostic modalities, MRI and MRA, ruled out ischemic stroke but indicated mild to moderate cerebral atrophy and chronic microvascular ischemic changes. The patient exhibited a seizure episode characterized by right-sided gaze preference and altered consciousness. Postictally, transient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
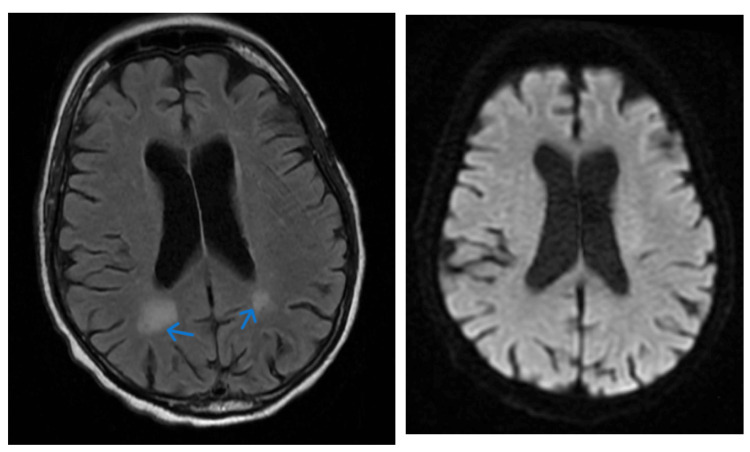 Figure 1
Figure 1| Component ref. range and units | |
| WBC (white blood cell) 4.80 - 10.80 x10(3)/mcL | 11.55 |
| RBC (red blood cell) 4.70 - 6.10 x10(6)/mcL | 3.05 |
| HGB (hemoglobin) 14.0 - 18.0 g/dL | 9.3 |
| HCT (hematocrit) 42.0-52.0% | 27.1 |
| Sodium 136-145 mmol/L | 139 |
| Potassium 3.5-5.1 mmol/L | 4.3 |
| Chloride 98-107 mmol/L | 100 |
| CO2 (bicarbonate) 22-29 mmol/L | 27 |
| BUN (blood urea nitrogen) 7-18 mg/dL | 14 |
| Creatinine 0.7-1.2 mg/dL | 1.2 |
| Ophthalmology exam finding | Right | Left |
| Pupils | PERLA, no APD | PERLA, no APD |
| Visual Acuity (Snellen-Linear) | ||
| Near CC (with correction) | J1 | J1 |
| Tonometry Pressure (Tonopen Avia) | 19 | 20 |
| Visual Field restriction | Total superior nasal, inferior nasal deficiencies | Total superior nasal, inferior nasal deficiencies |
| Slit Lamp Examination | ||
| Lids/Lashes | Normal | Normal |
| Conjunctiva/Sclera | White and quiet | White and quiet |
| Cornea | Clear | Clear |
| Anterior Chamber | Deep and quiet | Deep and quiet |
| Iris | Round and reactive | Round and reactive |
| Lens | Clear | Clear |
| Vitreous | Normal | Normal |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigraine and Headache Studies · Epilepsy research and treatment · Ophthalmology and Eye Disorders
Introduction
Occipital lobe epilepsies (OLEs) represent a relatively uncommon subgroup of epileptic disorders, accounting for an estimated 5% to 10% of epilepsies. These conditions are characterized by distinctive visual manifestations that can often be confused with other central nervous system (CNS) pathologies, such as migraines with visual aura, or even ophthalmological disorders [1]. This potential for misdiagnosis underscores the necessity for a thorough diagnostic approach to ensure timely and appropriate patient care. Patients with OLEs typically do not have a medical history of migraines, either with or without aura [2,3]. The visual hallucinations associated with OLEs frequently involve vivid, multicolored, circular, or spherical patterns that evolve dynamically [4]. These complex visual phenomena are more indicative of CNS involvement rather than ophthalmologic conditions. Another distinguishing feature of OLEs is the possible altered level of consciousness during episodes, a contrast to the preserved awareness observed in migraine sufferers. The duration of visual symptoms in OLEs typically spans from a few seconds up to three minutes [2]. These seizures often manifest in multiple daily or weekly clusters and may include preceding or subsequent blurring of vision [2-4]. In contrast, the visual auras of migraines tend to persist for 15 to 30 minutes and generally have a static quality. With a high index of clinical suspicion, the diagnosis of OLEs can be corroborated by diagnostic modalities such as electroencephalography (EEG), and neuroimaging with computed tomography (CT) or magnetic resonance imaging (MRI) [5].
Case presentation
An 88-year-old male with a medical background significant for hypertension, hyperlipidemia, and diabetes mellitus (not on any medications) presented with a three-week history of unusual visual disturbances. His home medications were Amlodipine 10 mg once daily and Atorvastatin 40 mg nightly. The patient described intermittent, kaleidoscopic visual phenomena, predominantly featuring red, blue, and yellow hues, manifesting as mushroom shapes and twirling floors that evolved into flowers with various petals. These symptoms were noted on the right side of his visual field, each lasting one to three minutes, and were often accompanied by a blurring of vision persisting for approximately 15 minutes before normalization. Neurological assessment revealed no focal deficits and a normal gait. His laboratory findings on presentation were within normal limits (Table 1). Ophthalmological evaluation, while the patient was experiencing visual deficit, identified a right homonymous hemianopsia; extraocular movements were intact (Table 2).
The patient was unaware of his visual deficits, and a point-of-care ocular ultrasound ruled out retinal detachment or vitreous hemorrhage. During our examination in the emergency department, the patient experienced a total of six episodes characterized by a forced right gaze preference with concomitant right-beating nystagmus on the left lateral gaze, which resolved on upward gaze. The episodes, lasting one to two minutes, were also accompanied by an altered level of consciousness with sluggish responsiveness. Post-episode, the patient reported transient right homonymous hemianopia. These episodes were repeated multiple times during his stay. Initial computed tomography (CT) head showed no evidence of acute intracranial hemorrhage or fracture, mild of moderate cerebral volume loss with no evidence of mass, hydrocephalus or cortical infarct. Electroencephalogram (EEG) showed no epileptiform activity. An MRI indicated hyperintensity in the periatrial white matter area, mild to moderate cerebral atrophy and chronic microvascular ischemic changes (Figure 1).
MRI T2 FLAIR images (blue arrow left) demonstrate areas of hyperintensity in the periatrial white matter bilaterally. There is no signal abnormality within the corpus callosum or along the callosal septal interface. DWI image (right) demonstrates no evidence of enhancing parenchymal lesion or abnormal leptomeningeal enhancement and shows mild to moderate cerebral atrophy and chronic microvascular ischemic changes.MRI: Magnetic resonance imaging, T2 FLAIR: T2 and fluid-attenuated inversion recovery
MRA showed no significant large vessel occlusions and carotid duplex ultrasonography found no notable stenosis. Given the recurrent episodes, the patient was loaded with levetiracetam 2000 mg and maintained with intravenous levetiracetam 750 mg twice daily. Lorazepam 2 g as needed was used for seizure cessation. Following a progressive improvement over four days, with a noted reduction in the frequency of episodes, the patient was discharged with Levetiracetam 1000 mg twice daily and scheduled for outpatient neurological follow-up in four weeks.
To assist in the identification and management of similar cases, it is important to note the sequence of symptom presentation and diagnostic findings. Initially, the patient experienced visual disturbances characterized by kaleidoscopic visuals predominantly in red, blue, and yellow, appearing as mushroom shapes and evolving floral patterns. These episodes were brief, lasting one to three minutes, but the visual blurring persisted for about 15 minutes. A timeline of symptoms alongside corresponding diagnostic findings, such as the right homonymous hemianopsia detected during the ophthalmological evaluation, can aid in distinguishing OLE from similar presentations. Understanding the typical progression and response to treatment can also guide management in new cases. Therefore, we recommend a systematic approach to documenting symptom onset, progression, and response to interventions in clinical practice.
Discussion
In this case, our differential diagnoses included left occipital lobe ischemia, focal seizure with altered level of consciousness, and migraine with visual aura. The final diagnosis was determined to be an OLE with an altered level of consciousness accompanied by postictal visual impairment. The absence of a migraine history, coupled with the unlikely presentation of homonymous hemianopsia as a migraine symptom, decreased the probability of migraine with visual aura. Typically, patients with migraines can recognize visual deficits, which was not the case here [3]. The patient's communication difficulties, where he could only articulate in brief phrases with notable pauses, suggested an altered level of consciousness consistent with seizure activity. The MRI did not reveal any signs of ischemia; thus, the persistent right homonymous hemianopsia was attributed to a postictal state - commonly known as Todd’s phenomenon - rather than ischemic events [6]. This phenomenon can be explained by the temporary stunning of neurons, which fail to maintain ion gradients necessary for light detection after intense electrical activity and ATP depletion. The diagnosis hinged on the observed seizure episode: the patient was initially speaking fluently but then exhibited a marked reduction in speech fluency and developed a right-sided gaze preference. Additionally, the fluctuating nature of the patient's right homonymous hemianopsia, which improved during seizure-free intervals and worsened postictally, further supported the seizure diagnosis.
Conclusions
This case represents a unique instance of occipital seizures that can be easily mistaken for visual migraines without headache, also known as acephalgic migraine visual aura. However, the distinguishing feature in this patient was the extended duration of the visual deficits, which is atypical for migraines. The ophthalmologic examination findings, combined with the patient's presentation of Todd's phenomena, contributed to the clear diagnosis for our case.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Elementary visual hallucinations in migraine and epilepsy J Neurol Neurosurg Psychiatry Panayiotopoulos CP 13711374571994796481410.1136/jnnp.57.11.1371 PMC 1073189 · doi ↗ · pubmed ↗
- 2Elementary visual hallucinations, blindness, and headache in idiopathic occipital epilepsy: differentiation from migraine J Neurol Neurosurg Psychiatry Panayiotopoulos CP 5365406619991020143310.1136/jnnp.66.4.536PMC 1736305 · doi ↗ · pubmed ↗
- 3Presentation, etiology, outcome, and differentiation of visual semiology of adult occipital epilepsy from visual aura of migraine headache: a prospective study in a tertiary care center in Bangladesh Cureus Mahmud R Sina H 014202210.7759/cureus.24186 PMC 910970535592185 · doi ↗ · pubmed ↗
- 4Visual phenomena and headache in occipital epilepsy: a review, a systematic study and differentiation from migraine Epileptic Disord Panayiotopoulos CP 20521611999 https://pubmed.ncbi.nlm.nih.gov/10937155/10937155 · pubmed ↗
- 5Occipital epilepsies: identification of specific and newly recognized syndromes Brain Taylor I Scheffer IE Berkovic SF 75376912620031261563610.1093/brain/awg 080 · doi ↗ · pubmed ↗
- 6Todd Paresis Mastriana J Pay JL De Jesus O Treasure Island, FL Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 532238/30335271 · pubmed ↗