A Rare Case of Small Intestinal Cancer With Uterine Metastasis After Surgery for Ovarian Metastasis, Diagnosed Using Immunostaining
Sachiko Nagao, Motoki Matsuura, Shoko Kurokawa, Masato Tamate, Taishi Akimoto, Tsuyoshi Saito

TL;DR
A woman with small intestinal cancer later developed metastases in her ovary and uterus, diagnosed through histopathology and immunostaining.
Contribution
Highlights the importance of immunohistochemistry in distinguishing metastatic cancer from primary tumors in rare cases.
Findings
Uterine metastasis from small intestinal cancer was confirmed via immunostaining markers CK7, CK20, SATB2, and PAX2.
Histopathology and immunohistochemistry are critical for accurate diagnosis and treatment planning in metastatic cancer cases.
Abstract
Uterine metastases from extragenital sites are rare. We present a case of a woman who had undergone surgery for small intestinal cancer and subsequently developed metastases in her left ovary and uterus. A nulliparous woman in her 50s underwent laparoscopic partial small bowel resection with lymph node dissection for small intestinal cancer. Five months later, computed tomography (CT) revealed a left ovarian tumor and ascites. She underwent bilateral adnexectomy and adjuvant chemotherapy, and the ovarian tumor was diagnosed as a small intestinal cancer metastasis. Two years after the small intestinal cancer surgery, a positron emission tomography (PET)-CT scan revealed a uterine accumulation. Cervical cytology was negative for intraepithelial lesion or malignancy. Endometrial histology showed an adenocarcinoma of the uterus. The patient underwent total abdominal hysterectomy followed by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
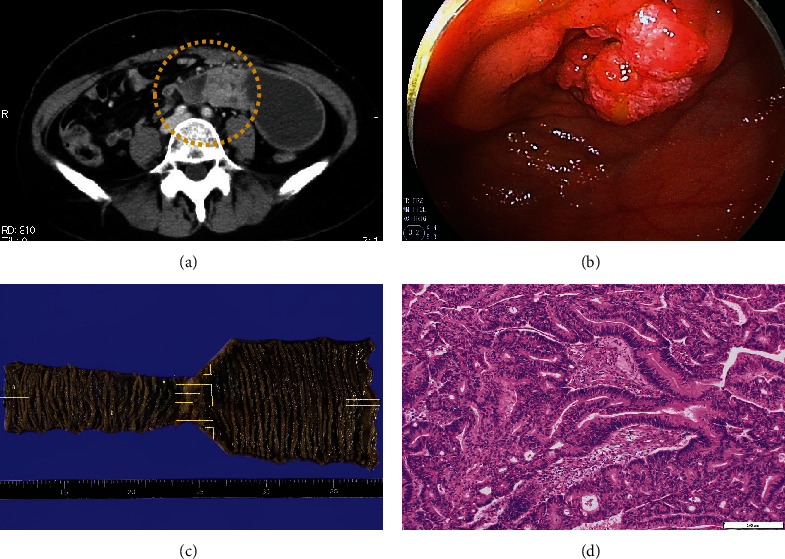 Figure 1
Figure 1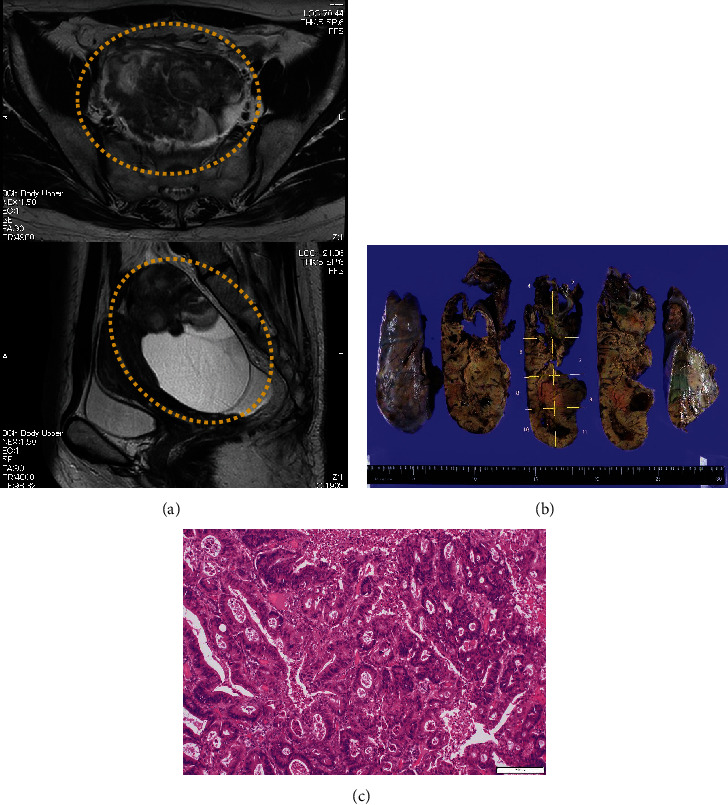 Figure 2
Figure 2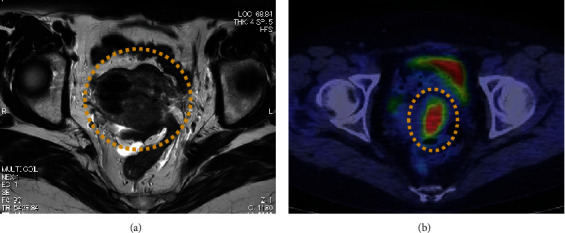 Figure 3
Figure 3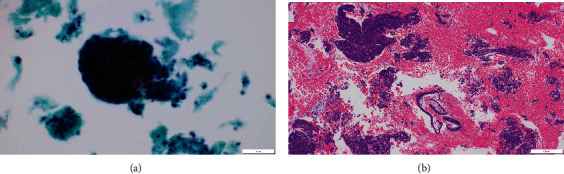 Figure 4
Figure 4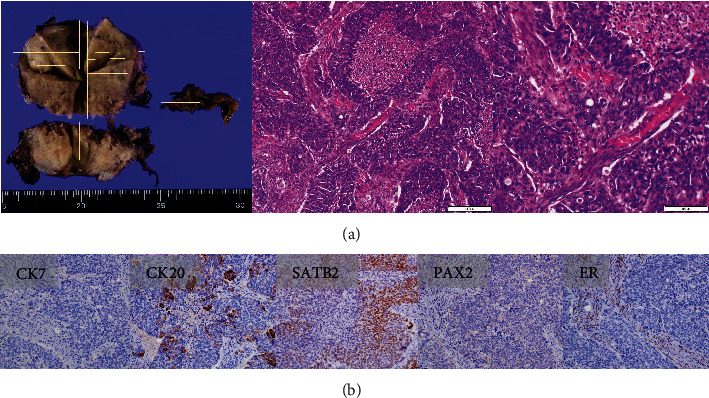 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUterine Myomas and Treatments · Ovarian cancer diagnosis and treatment · Endometrial and Cervical Cancer Treatments
1. Introduction
Compared with metastatic ovarian tumors, metastatic uterine tumors are rare. A study by Karpathiou et al. [1] found that metastatic tumors to gynecological organs involve the ovary in 50% of cases, whereas the endometrium and myometrium are involved in only 3.6% and 10.7% of cases, respectively. The primary sites reported for metastatic uterine tumors include the colon, stomach, breast, malignant melanoma, and lungs [2, 3]. Small bowel cancer is rare, accounting for less than 0.5% of all malignant tumors and 5% of all gastrointestinal malignant tumors.
This report describes a rare case of small bowel cancer metastasizing to the ovary and uterus in a patient who had undergone surgery for small bowel cancer.
2. Case Presentation
The patient was a nulliparous woman in her 50s who had undergone menopause at the age of 49 years old. Her father had colon cancer. She underwent laparoscopic partial small bowel resection and regional lymph node dissection for small bowel cancer in our gastroenterological surgery department. Histopathological examination revealed a Type 2 tumor measuring 25 × 10 mm with high columnar cell growth forming fused, cribriform, and papillary ducts on histopathology. The tumor was diagnosed as a moderately differentiated adenocarcinoma, pT4, pN2, cM0, and Stage IIIB (Figure 1). Five months after the surgery, a follow-up contrast-enhanced computed tomography (CT) scan revealed a left ovarian tumor and ascites, and the patient was referred to our department. A magnetic resonance imaging (MRI) scan revealed a left ovarian tumor with heterogenous enhancement, measuring 107 × 57 mm (Figure 2). No obvious lesions were noted in the uterus. The enhanced portion showed a diffusion abnormality in the left ovary suggestive of malignancy. A bilateral abdominal adnexectomy was performed, and histopathological examination revealed the same histopathology as the previous small bowel cancer (Figure 2). Immunostaining was negative for Cytokeratin 7 (CK7), positive for Cytokeratin 20 (CK20) and Special AT-Rich Sequence-Binding Protein 2 (SATB2), and negative for estrogen receptor (ER) and Paired Box Gene 2 (PAX2), leading to a diagnosis of metastatic recurrence of small bowel cancer. The patient received 12 cycles of mFOLFOX as postoperative chemotherapy. A positron emission tomography (PET)/CT scan 24 months after the small bowel cancer surgery revealed accumulation in the uterus and obturator lymph nodes (Figure 3), and the patient was referred back to our department with suspected uterine metastasis of the small bowel cancer. Her symptoms included a small amount of genital bleeding. Tests of tumor markers showed elevated levels of CA19-9, carcinoembryonic antigen (CEA), and CA125. Cervical cytology was negative for intraepithelial lesion or malignancy, but endometrial cytology revealed clusters of atypical cells with enlarged nuclei, an irregular karyotype, and distinct nuclei on a hematogenous background, with prominent irregular stacking and disarrangement of nuclei, leading to a diagnosis of adenocarcinoma. Endometrial histology revealed atypical cells proliferating solidly within the stromal tissue, a finding that suggested poorly differentiated carcinoma (Figure 4). Immunostaining of the atypical cells was negative for CK7, partially positive for CK20, and negative for ER, indicating metastatic small bowel cancer rather than a primary malignant uterine tumor. Although pelvic and para-aortic lymph node dissection is generally performed in primary malignant uterine tumors, considering the long duration of the surgery and the high risk of perioperative complications such as lymphedema, a total abdominal hysterectomy and pelvic lymph node biopsy were performed without lymph node dissection. Macroscopically, the tumor had grown to replace the myometrium and was also exposed on the serosal surface. Histopathological examination revealed moderate to poorly differentiated adenocarcinoma with extensive spread throughout the uterus and lymphatic invasion. The ascites cytology was negative. Immunostaining was negative for CK7, positive for CK20 and SATB2, and negative for ER and PAX2; therefore, the patient was diagnosed with a uterine metastasis of small bowel cancer (Figure 5 and Table 1). The patient is currently undergoing FOLFIRI+BEV therapy.
3. Discussion
Small bowel cancer is rare, accounting for less than 0.5% of all malignant tumors and 5% of all gastrointestinal malignant tumors. There is no standard treatment, but primary tumor resection is commonly performed for Stages I–III, and systemic chemotherapy is commonly administered for Stage IV or postoperative recurrence. In Japan, FOLFOX therapy for Stage IV or postoperative recurrence has been covered by insurance since September 2018.
Uterine metastases due to extragenital primary tumors are rare [1]. Primary sites reported include the colon, stomach, breast, malignant melanoma, and lungs [2, 3]. In Japan, several cases of metastasis of gastric cancer to the uterus have been reported [4–6]. In recent years, the number of cases of uterine metastasis is thought to have been increasing as the incidence of colon and breast cancer increased. The most common symptom of uterine metastasis is irregular bleeding, but it is sometimes asymptomatic [7], and this case was discovered during follow-up imaging examination of the patient after treatment for small bowel cancer. The reasons for the rarity of uterine metastasis include that lymph flows away from the uterus and because fibromuscular tissue is unfavorable for metastatic tumors [8].
Cytology and histology tend to be negative because metastatic tumors often invade the uterine stroma and myometrium and are rarely exposed to the mucosal surface. Cases with invasion of the cervix should be distinguished from cervical adenocarcinoma.
In the case of this patient, pathology specimens from the primary lesion in the small bowel showed a moderately differentiated adenocarcinoma, but the metastatic lesion in the uterus showed a moderate to poorly differentiated adenocarcinoma. Histologic changes in metastatic lesions, especially dedifferentiation to poorly differentiated carcinoma, are common after chemotherapy. This is hypothesized to be because only resistant cancer cells remain after chemotherapy [9].
4. Conclusion
In this patient, because the tumor was exposed on the endometrium, endometrial cytology revealed malignant cells, and immunostaining on endometrial histology enabled the determination of the primary site. The high possibility of a metastatic tumor was taken into consideration in planning the surgery, and the patient was able to smoothly transition to treatment for recurrent small bowel cancer. A careful examination taking the possibility of metastatic tumors originating from other organs into account is useful for making policy decisions and treatment choices regarding patient management. In addition, uterine metastasis from small bowel cancer is an extremely rare condition, so in the initial surgery, bilateral adnexectomy was performed because no signs of uterine involvement were present at the time and the risk of uterine metastasis was considered to be low; however, a uterine metastasis developed subsequently. Although bilateral adnexectomy alone is often performed when ovarian metastasis is diagnosed, some surgeons perform a prophylactic hysterectomy based on the possibility that a uterine metastasis may be found later, as in this case.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Karpathiou G. Chauleur C. Hathroubi S. Peoc’h M. Secondary tumors of the gynecologic tract: a clinicopathologic analysis International Journal of Gynecological Pathology 201938436337010.1097/PGP.00000000000005162-s 2.0-8506730839029750707 · doi ↗ · pubmed ↗
- 2Tsoi D. Buck M. Hammond I. White J. Gastric adenocarcinoma presenting as uterine metastasis-a case report Gynecologic Oncology 200597393293410.1016/j.ygyno.2005.01.0552-s 2.0-2044445494115943994 · doi ↗ · pubmed ↗
- 3Kumar A. Schneider V. Metastases to the uterus from extrapelvic primary tumors International Journal of Gynecological Pathology 19832213414010.1097/00004347-198302000-000042-s 2.0-00210601176313532 · doi ↗ · pubmed ↗
- 4Imachi M. Tsukamoto N. Amagase H. Shigematsu T. Amada S. Nakano H. Metastatic adenocarcinoma to the uterine cervix from gastric cancer. A clinicopathologic analysis of 16 cases Cancer 199371113472347710.1002/1097-0142(19930601)71:11<3472::aid-cncr 2820711103>3.0.co;2-v 8387879 · doi ↗ · pubmed ↗
- 5Matsuura Y. Saito R. Kawagoe T. Toki N. Sugihara K. Kashimura M. Cytologic analysis of primary stomach adenocarcinoma metastatic to the uterine cervix Acta Cytologica 199741229129410.1159/0003325142-s 2.0-00309890139100756 · doi ↗ · pubmed ↗
- 6Yokoyama Y. Sato S. Futagami M. Saito Y. Solitary metastasis to the uterine cervix from the early gastric cancer: a case report European Journal of Gynaecological Oncology 200021546947111198034 · pubmed ↗
- 7Piura B. Yanai-Inbar I. Rabinovich A. Zalmanov S. Goldstein J. Abnormal uterine bleeding as a presenting sign of metastases to the uterine corpus, cervix and vagina in a breast cancer patient on tamoxifen therapy European Journal of Obstetrics, Gynecology, and Reproductive Biology 1999831576110.1016/s 0301-2115(98)00268-12-s 2.0-003303892610221611 · doi ↗ · pubmed ↗
- 8Zhang Y. C. Zhang P. F. Wei Y. H. Metastatic carcinoma of the cervix uteri from the gastrointestinal tract Gynecologic Oncology 198315228729010.1016/0090-8258(83)90084-72-s 2.0-00205816536832638 · doi ↗ · pubmed ↗