Lower Back Pain Beyond Routine Causes: Sacral Spinal Epidural Arteriovenous Fistula (SEDAVF)
Hari Deep Yellamilli, Srikanth Muni, Rajasekhar Rekapalli, Vemula Anjanipriya, Anuvindha JS

TL;DR
A rare case of severe lower back pain in a young man was caused by a sacral spinal epidural arteriovenous fistula, successfully treated with endovascular embolization.
Contribution
This paper presents a rare and complex case of SEDAVF as an unusual cause of lower back pain in a young patient.
Findings
A 32-year-old man presented with severe backache, urinary retention, and constipation due to SEDAVF.
Contrast-enhanced MRI and digital subtraction angiography confirmed the rare diagnosis of SEDAVF.
Endovascular embolization successfully treated the patient's condition.
Abstract
Lower back pain (LBP) is a frequent complaint, even among young people. The most common cause is attributed to slipped discs or vertebral fractures. Less common etiologies should also be considered when presenting with typical symptoms of severe backache. Here, we are presenting one such uncommon case. A 32-year-old man with a history of meningocele repair in neonates presented with severe backache, urinary retention, and constipation in an emergency. Initially, the patient was treated elsewhere, but symptoms persisted. A contrast-enhanced MRI done in the emergency revealed a rare sacral spinal epidural arteriovenous fistula (SEDAVF) with cord congestion. The patient was taken up for digital subtraction angiography, which confirmed the diagnosis, and was treated successfully with endovascular embolization. This case highlights the complex presentation of SEDAVF and the importance of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
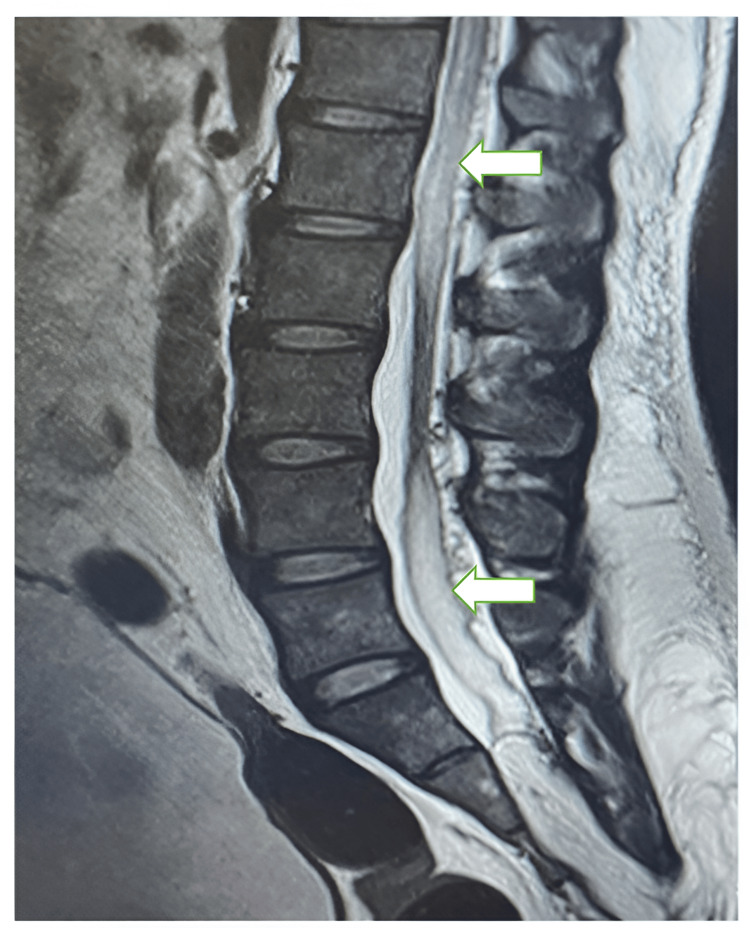 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Vascular Malformations Diagnosis and Treatment · Spinal Fractures and Fixation Techniques
Introduction
Back pain is a frequent complaint. The lower back pain (LBP) prevalence in young adults aged between 18 and 35 years was 42.4% per year and 22.8% per week [1]. Andersson estimated the annual worldwide LBP incidence in adults to be 15% and the point prevalence to be 30% [2]. The etiology of back pain is classified into traumatic, degenerative, oncologic, infectious, inflammatory, metabolic, referred pain, postural, congenital, and psychiatric [3]. Epidural arteriovenous fistulas comprise a major proportion of spine vascular lesions, with an annual incidence of 5-10 per million. At least 80% of patients are male, and more than 66% of patients are in the sixth and seventh decades of life, indicating a preponderance of gender and age [4]. We report a case of a 32-year-old man with severe backache and progressive lower limb sensory deficits, ultimately diagnosed with a sacral spinal epidural arteriovenous fistula (SEDAVF). Spinal arteriovenous malformations (AVMs) are rare pathologies, representing 3-4% of all space-occupying lesions affecting the spinal cord [5].
Case presentation
A 32-year-old male with a history of meningocele repair at 10 days old presented with complaints of severe backache for 10 days, associated with an inability to pass urine and constipation. He had no history of fever, falls, trauma, or other complaints. He received treatment at another hospital a week prior with no improvement in symptoms. He has had a history of bladder incontinence since childhood and uses a self-catheter.
Examination
On arrival, the vitals were normal. A neurological examination revealed bilateral lower limb power (5/5), and he was able to walk. The straight leg-raising test was positive at 50 degrees. Sensory examination revealed diminished sensation in the lower limbs compared to the upper limbs. Local examination revealed tenderness over the L3-S1 vertebrae, normal sphincter tone, and a vertical scar on the right side of the sacrum.
Imaging
The patient was taken for an emergency MRI spine with contrast, which showed sacral SEDAVF with associated posterior peri-medullary venous congestion, intermittent cord expansion, lipomyelocele, and bilateral hydroureteronephrosis. Figure 1 shows spinal cord edema with intermittent cord normal.
Spinal cord edema (block arrows)
Figure 2 shows the peri-medullary congestion adjacent to the spinal cord and lipomyelocele entering the spinal canal.
Peri-medullary congestion (small arrows) and lipomyelocele (block arrow)
The patient was followed up with digital subtraction angiography (DSA), which confirmed the diagnosis and helped in the localization of the vessel. The patient underwent successful embolization of vessels with the resolution of symptoms post-procedure.
Discussion
SEDAVFs are rare, complex lesions, often presenting with clinical manifestations secondary to compressive symptoms or congestive myelopathy. SEDAVFs are usually located in the ventral epidural space and are fed mainly by the anteriorly coursing epidural arteries [6]. The shunt flow drains first into the epidural venous sac and then to the paravertebral vein [7]. In the systematic review by Huang et al., 10% of SEDAVF patients had spine surgery prior, leading to a history of spine surgery as a risk factor for SEDAVF [8].
Clinical manifestations can vary depending on the location and size of the fistula, ranging from vague back pain and radiculopathy to progressive myelopathy and even paraplegia. DSA is regarded as a basic diagnostic tool for the angiomorphologic, pretherapeutic evaluation of spinal arteriovenous fistulas and malformations [9]. Very few indications remain for neuroangiography due to advances in CT and MRI imaging, such as intracranial aneurysms, AVMs, and dural arteriovenous shunts (both intracranially as well as in the spine), for which angiography is still necessary [10].
SEDAVFs are characterized by an epidural venous sac, usually located in the ventral epidural space, multiple bilateral feeders feeding it, and the absence of a horizontal T-sign. The T-sign is a typical sign seen in SDAVF. Kiyosue et al. found that SEAVFs frequently involve the lumbar spine (83%) [11].
Current treatment options include endovascular embolization with liquid embolic agents or coils, surgical resection of the fistula, or both. Endovascular treatment is the favored method of treatment, with about two-thirds of studies and case reports using the method. Onyx is the preferred embolic material over glue, as it is a non-thrombogenic embolic material that allows for better packing of the epidural venous sac without the risk of thrombus formation [12]. Al-Abdulwahhab et al. observed that in all 12 SEAVF patients, an epidural venous sac drains into both intradural and extradural. Spinal cord edema improved in all patients for a mean of 18 months after treatment [13]. Among the microsurgical, endovascular, and combined treatment groups of SEDAVFs, the treatment failure rate was significantly higher in the endovascular treatment group (7.5%, 31%, and 0%, respectively), according to Takai et al.'s study conducted in Japan [14]. The vast majority of SEDAVFs remain idiopathic [15].
Conclusions
This case report highlights the typical presentation of SEDAVF with back pain and neurologic deficits. Early diagnosis and prompt intervention with endovascular embolization can significantly improve outcomes and prevent potential neurological complications in patients with spinal AVMs. Microsurgery has a lower chance of failure in treating SEDAVF.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prevalence and risk factors for low back pain in 1,355 young adults: a cross-sectional study Asian Spine J Ganesan S Acharya AS Chauhan R Acharya S 6106171120172887498010.4184/asj.2017.11.4.610PMC 5573856 · doi ↗ · pubmed ↗
- 2Epidemiological features of chronic low-back pain Lancet Andersson GB 58158535419991047071610.1016/S 0140-6736(99)01312-4 · doi ↗ · pubmed ↗
- 3Acute and chronic low back pain Med Clin North Am Patrick N Emanski E Knaub MA 7777899820142499405110.1016/j.mcna.2014.03.005 · doi ↗ · pubmed ↗
- 4Spinal dural arteriovenous fistula Curr Opin Neurol Koch C 69751920061641568010.1097/01.wco.0000200547.22292.11 · doi ↗ · pubmed ↗
- 5Classification and therapeutic modalities of spinal vascular malformations in 80 patients Neurosurgery Bao YH Ling F 7581401997897182710.1097/00006123-199701000-00017 · doi ↗ · pubmed ↗
- 6Spinal epidural arteriovenous fistula with perimedullary venous reflux: clinical and Neuroradiologic features of an underestimated vascular disorder AJNR Am J Neuroradiol Mull M Othman A Dafotakis M Hans FJ Schubert GA Jablawi F 209521023920183033743410.3174/ajnr.A 5854 PMC 7655362 · doi ↗ · pubmed ↗
- 7Comparative analysis of spinal extradural arteriovenous fistulas with or without intradural venous drainage: a systematic literature review Neurosurg Focus Takai K Taniguchi M 81032201210.3171/2012.2.FOCUS 121622537134 · doi ↗ · pubmed ↗
- 8Spinal extradural arteriovenous fistulas: clinical article J Neurosurg Spine Huang W Gross BA Du R 5825901920132403330510.3171/2013.8.SPINE 13186 · doi ↗ · pubmed ↗