Cholangioscope-assisted evaluation and endoscopic incision of stricture caused by thick mucosal bridge in Crohn’s disease
Xianzong Ma, Lang Yang, Yan Jia, Zilin Kang, Mingjie Zhang, Dongliang Yu, Peng Jin

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1 Fig. 2
Fig. 2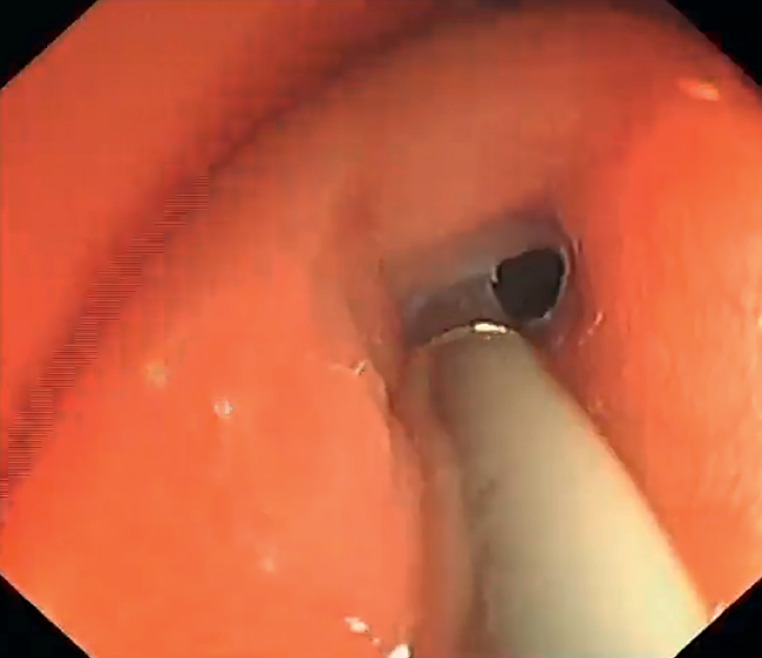 Fig. 3
Fig. 3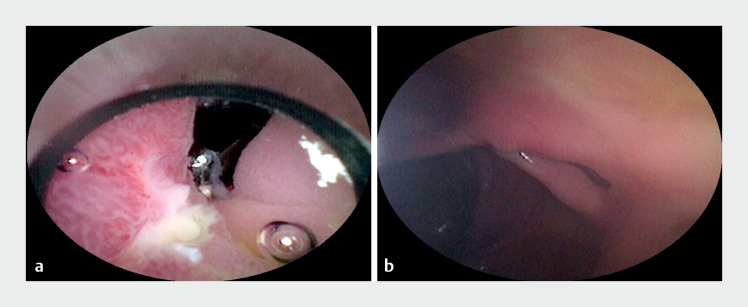 Fig. 4
Fig. 4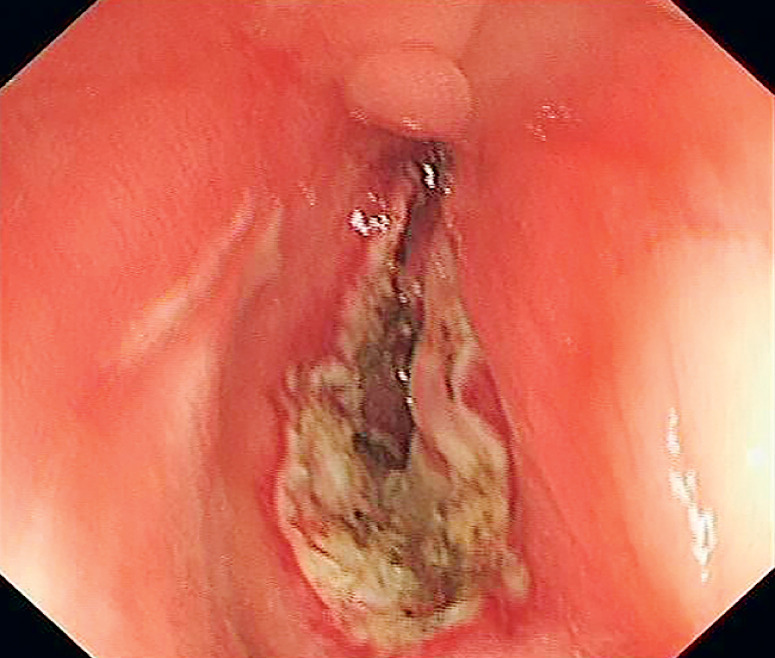 Fig. 5
Fig. 5- —Capital’s Funds for Health Improvement and Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Biliary and Gastrointestinal Fistulas · Diverticular Disease and Complications
A 32-year-old man with an 8-year history of Crohn’s disease (Montreal classification A2, L3, B2p) presented with recurrent abdominal pain. After regular treatment with ustekinumab for 3 years, recent computed tomography revealed severe stricture in the ascending colon ( Fig. 1 ), and colonoscopy showed colorectal mucosal healing. However, two tiny holes were observed and could not be passed by the colonoscope ( Fig. 2 ).
Computed tomography showed severe stricture of the ascending colon in Crohn’s disease.
Two tiny holes in the stricture were observed and could not be passed by the colonoscope.
In order to find out which hole was the real narrow bowel lumen and to exclude a potential fistula, a cholangioscope (eyeMAX, 9 F; Micro-Tech, Nanjing, China) was inserted into the two holes respectively to gain direct views inside and behind the holes ( Fig. 3 ) 1 2 . Amazingly, the ileocecal valve was reached by the cholangioscope through both holes, and superficial ulcer in the inner wall of the holes and multiple scar changes in the ileocecal region were observed simultaneously ( Fig. 4 ). The cholangioscopy result indicated that the stricture was caused by a rare thick mucosal bridge between the two holes. Subsequently, the bridge mucosa and submucosal scar were incised by an ITknife nano (Olympus, Tokyo, Japan) ( Fig. 5 ). No active bleeding or perforation occurred during the procedure. Finally, the colonoscope could pass smoothly through the stricture and reach the ileocecal valve ( Video 1 ).
The cholangioscope was inserted into one hole.
Cholangioscopy showed superficial ulcers in the inner wall of the stricture. The cholangioscope reached the ileocecal valve through both holes.
The stricture was treated after incision of the bridge mucosa and submucosal scar under colonoscopy.
Cholangioscopy-assisted evaluation and targeted treatment for Crohn’s disease-associated stricture.Video 1
Currently, the evaluation of bowel stenosis in Crohn’s disease is mainly based on radiology and ultrasonography 3 . However, neither method can directly reveal the clear presentation of the inner wall of the narrowed intestinal lumen, including ulcers, tiny fistula, and edema near the stricture. To our knowledge, this is the first reported case of cholangioscope-assisted evaluation and management of Crohn’s disease-related stricture, and suggests the feasibility of the procedure in selected Crohn’s disease cases.
Endoscopy_UCTN_Code_TTT_1AQ_2AF
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhang W Chai N Zhai Y Cholangioscopy-assisted extraction of choledocholithiasis and partial sediment-like gallstones through papillary support: a pilot exploration for super minimally invasive surgery Endoscopy 202355 E 274E 27536442588 10.1055/a-1974-8701 PMC 9831755 · doi ↗ · pubmed ↗
- 2Kong LJ Liu D Zhang JY Digital single-operator cholangioscope for endoscopic retrograde appendicitis therapy Endoscopy 20225439640010.1055/a-1490-043433893629 · doi ↗ · pubmed ↗
- 3Shen B Kochhar G Navaneethan U Practical guidelines on endoscopic treatment for Crohn’s disease strictures: a consensus statement from the Global Interventional Inflammatory Bowel Disease Group Lancet Gastroenterol Hepatol 2020539340531954438 10.1016/S 2468-1253(19)30366-8 · doi ↗ · pubmed ↗