Outcomes and return to sport after osteochondral autograft transplantation for osteochondritis dissecans of the capitellum: a systematic review
Gabriel Lane, Matthew V. Smith, Charles A. Goldfarb, Rogelio A. Coronado, Eric N. Bowman

TL;DR
This study reviews outcomes of a surgical treatment for elbow injuries in athletes, showing high return to sports rates but variable performance levels.
Contribution
The study provides a systematic review of return to sport rates and outcomes after osteochondral autograft transfer for elbow OCD.
Findings
97% of patients returned to sports after OAT for capitellar OCD.
Return to previous performance levels ranged from 10% to 100%.
Postoperative scores were excellent, with better outcomes for centralized lesions.
Abstract
Capitellar osteochondritis dissecans (OCD) lesions are common in athletes. Osteochondral autograft transfer (OAT) is one possible treatment option, though outcomes including return to sport (RTS) data are limited to small series. The purpose of this study was to systematically review RTS following OAT for capitellar OCD lesions. Our secondary objectives were to evaluate patient-reported outcomes (PROs), range of motion (ROM), and complications after OAT. PubMed, Embase, and Cumulative Index to Nursing and Allied Health Literature were searched for peer-reviewed articles on “osteochondral autograft transfer” and related terms for capitellar OCD lesions. Articles were included if they reported an RTS rate and had a follow-up time point of at least 12 months. Data on RTS rates, PRO measures, complications, and ROM were extracted. Articles were assessed for methodological quality using the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
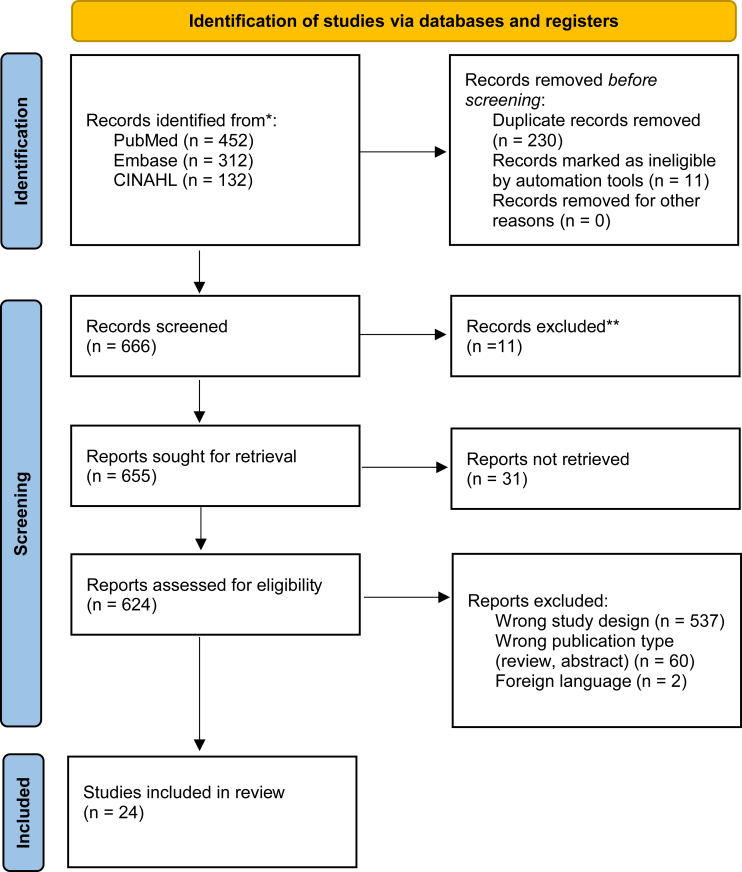 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElbow and Forearm Trauma Treatment · Orthopedic Surgery and Rehabilitation · Shoulder Injury and Treatment
Osteochondritis dissecans (OCD) of the elbow is common among youth baseball players and gymnasts, with an overall incidence of 6.0 per 100,000 in the United States, with a 1.8% cumulative incidence per year among youth baseball players.9^,^17^,^36 Capitellar OCD may present as an incidental finding on imaging with only 35% of patients with capitellar OCD reporting pain.17 Patients presenting with symptoms of pain or mechanical symptoms impairing athletic performance are treated based on patient age and stability of the lesion. The goal of treatment is to restore full, painless range of motion (ROM) in order to return the athlete to his or her previous level of performance. Nonoperative treatment is often successful in stable lesions, particularly those with an open capitellar physis.31 When conservative treatments for all-sized lesions fail and with large or unstable lesions, surgical management may be beneficial.
Surgical options for OCD include removal of loose bodies, drilling, débridement, microfracture, chondrocyte implantation, bone-peg grafting, and osteochondral transplants.30 Osteochondral autograft transfer (OAT) is a cartilage restoration procedure in which a cartilage and bone plug is harvested, often from a non-weight-bearing aspect of the distal femoral condyle, then transferred into the defect.24 While outcomes have generally been described as favorable with limited donor-site morbidity, case series are limited, and several recent studies have been published since previous systematic reviews. The purpose of this study was to systematically evaluate the literature regarding OAT return to sport (RTS), patient-reported outcomes (PROs), and ROM.
Methods
Study design
This study is a systematic review of published peer-reviewed studies reporting RTS, PROs, ROM, and complications after OAT for OCD. The design and conduct of this systematic review followed guidelines from the Cochrane Handbook for Systematic Reviews. Reporting of this review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.23 Meta-analyses were not performed as included articles are level III and IV evidence studies.
Literature search
A comprehensive literature search was conducted in July 2022 to evaluate the literature from inception. Embase and Cumulative Index to Nursing and Allied Health Literature databases were searched using a prespecified search strategy (Fig. 1). Related terms for osteochondral autograft transplantation, grafting, elbow, capitellum, and outcomes were combined and searched (the complete list of Boolean terms is found in Appendix 1). The resulting articles were exported into the EndNote reference management tool (Clarivate, Philadelphia, PA, USA) for records management.32Figure 1PRISMA flow chart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Selection criteria
All articles were independently reviewed by two authors (E.N.B. and G.C.L.) for inclusion, with a third reviewer available to resolve any disagreements. The online software Rayyan was used to review and select articles.20 Peer-reviewed primary research articles in the English language regarding capitellar OCD treatment with OAT or stratified for OAT with follow-up for at least 12 months were included. We required that articles include a quantitative report of (RTS) and at least one PRO measure or ROM measurement.
Articles were excluded if they were not available in the English language, were not primary research articles (including book chapters, systematic reviews, editorial commentaries, narrative reviews, animal, or cadaver studies), were surgical technique papers which did not include outcome measures, or if they were reports that did not include outcomes pertaining to OAT (fixation, débridement, allograft transplantation without OAT data). Twenty-four articles were included.
Data analysis
The following data were extracted: authors and year published, patient demographics (number of elbows, age, sex, skeletal maturity, level of play), patient characteristics (dominant arm involvement, lesion classification, mean follow-up), outcomes (RTS rate, PRO measures, ROM, and number of revision procedures), and complications. The primary outcome measure of this study was the RTS rate regarding OATs. Preoperation and postoperation data were collected for ROM and PROs when available. Two articles were included which did not include preoperative and postoperative PROs, but these were included as information was complete for all other desired data points.1^,^3
Osteochondritis lesions were described predominantly using the International Cartilage Regeneration and Joint Preservation Society grading system.18 Grade 0 lesions are normal cartilage with no magnetic resonance imaging signal changes. Grade 4 lesions are the most severe and contain a loose body within the lesion or joint space. Grade 2, 3, and 4 lesions were reported among the included studies.
Outcome measures were recorded for each study. The Timmerman-Andrews (TA) scoring system33 defines an excellent overall score as 180-200 while a poor score is defined as less than 120. Total scores are a sum of a subjective component (patient’s perception of the following: pain, swelling, locking/catching, and difficulty performing activities) and an objective component (flexion contracture, pronation/supination, and sagittal arc of motion). Outcome measures were also reported using the Broberg and Morrey rating system, Disabilities of the Arm, Shoulder, and Hand (DASH) score, Japanese Orthopedic Association (JOA) score, and Mayo Elbow score. Higher scores are associated with better elbow function except for the DASH score, in which a lower score is associated with better function. RTS was defined as the patient being able to return to any level of competition for their primary sport. The rate at which patients returned to a lower level of sport was also extracted when included.
Methodological quality
Methodological quality was assessed using the Methodological Index for Non-randomized Studies scoring system (Appendix 2).29 The Methodological Index for Non-randomized Studies instrument contains 8 items for noncomparative studies and 12 items for comparative studies to assess the risk of bias. Higher scores are correlated with a lower risk of study bias. Each study was independently reviewed by two authors (E.N.B.) and (G.C.L.) with a third author available to resolve any disagreements.
Results
Study selection, demographics, and lesion characteristics
The initial search yielded 452 results from PubMed, 312 results from Embase, and 132 results from Cumulative Index to Nursing and Allied Health Literature. The reference lists of articles were reviewed for missed articles and one additional article was included. After duplicates were removed, a total of 666 unique articles were identified for review with 24 meeting inclusion criteria. The summary of these studies, demographic, and lesion characteristics are shown in Table I. Included studies were from 2005 to 2021. There were 3 Level III cohort studies16^,^35^,^39 22 Level IV studies. Overall, 470 patients were included. The age of patients ranged from 13 to 22 years of age. Five studies reported the skeletal maturity of patients.6^,^14^,^15^,^26^,^28 All except 3 studies had a patient population strictly composed of athletes.3^,^27^,^37 Eleven studies noted whether the lesion was in the dominant arm1, 2, 3^,^8^,^15^,^16^,^18^,^19^,^26^,^34^,^37; 7 studies reported that only the dominant arm was involved.1^,^8^,^15^,^16^,^18^,^19^,^26^,^34Table IDemographic and lesion characteristics reported in 24 included studies.StudyLevel of evidenceNumber of patientsMean patient ageMale: FemaleProportion skeletally matureAthletes only?Proportion with dominant arm involvementICRS lesion gradeAllagui et al1 (2012)IV1171:0NRYes13Ansah et al2 (2007)IV5174:3∗NRYes0.24Ayzenberg et al3 (2021)IV1513.711:4NRNo0.64Bilsel et al5 (2010)IV1171:0NRYesNR3Funakoshi et al6 (2018)IV2213.522:0NRYesNR2,3,4Iwasaki et al8 (2006)IV8148:0NRYes13,4Iwasaki et al7 (2009)IV1914.219:01YesNR3,4Lyons et al13 (2015)IV1114.510:1NRYesNRNRManiwa et al14 (2017)IV913.79:00.36YesNRNRMaruyama et al15 (2014)IV3313.633:00.88Yes13,4Matsuura et al17 (2017)III8713.286:1NRYes13,4Mihara et al18 (2010)IV713.37:0NRYes13,4Mirzayan et al19 (2016)IV915.39:0NRYes12,3,4Nishinaka et al21 (2014)IV2213.922:0NRYesNR3,4Ovesen et al22 (2011)IV10184:6NRYesNRNRPederzini et al25 (2017)IV922.47:2NRYesNRNRSato et al26 (2018)IV7214.371:10.972Yes13,4Shimada et al27 (2012)IV261626:0NRNoNR3,4Shimada et al28 (2005)IV1014.310:00.5YesNRNRTsuda et al34 (2005)IV312.72:1NAYes1NRUeda et al35 (2021)III291429:0NAYesNRNRWeigelt et al37 (2015)IV14189:5NANo0.573,4Yamagami et al39 (2018)III301430:0NAYesNRNRYamamoto et al40 (2006)IV1813.618:0NAYesNR3,4ICRS, International Cartilage Repair Society; NR, not reported.∗Ratio reports entire study population.
Return to sport
Outcome scores for the included studies are summarized in Table II. RTS was achieved in 454/470 patients (97%). RTS rate ranged from 79% to 100%; all but 5 studies reported a RTS rate of 100%. Seven studies reported a proportion of their study population, 38 patients in total, returning to a reduced level of sport (range: 10%-100%).6^,^8^,^12^,^15^,^21^,^28^,^40 Baseball players, and pitchers specifically, were more likely to RTS at a lower level of play or not able to return at all. Time to RTS among included articles ranged from 4 months to 12 months.Table IISummary findings for return to sport rates and patient outcomes.ArticleMean follow-up (months)RTS rate (%)Return to reduced level of sport (%)Preop patient-reported outcomePostop patient-reported outcomePreop range of motionPostop range of motionNumber of revisions/2nd looksAllagui et al1 201224100NRNRNR−15° extension, 130° flexion, 115° total arcNR0Ansah et al2 200759.3100NRB&M; 76.3B&M; 97.64.7° extension lag, 12.9° flexion lag0 °extension lag, 0° flexion lag0Ayzenberg et al3 202129.5100NRNRNR121.9° (arc), 131.2° (passive flexion), 9.2° flexion contracture139.1° (arc), 142.7° (passive flexion), 2.7° flexion contracture2Bilsel et al5 201040100NRDASH; 12DASH; 15° extension, 120° flexion0 ° extension, 140° flexion0Funakoshi et al6 201827.510090T-A; 125 ± 30.1 (central lesion)T-A; 138.3 ± 34.5 (lateral lesion)T-A; 193.5 ± 11.3 (central lesion)T-A; 186.7 ± 18.1 (lateral lesion)NR132.7° (123°-142.4°) total arc0Iwasaki et al8 20062410025T-A; 134T-A; 183110° (93°-127°) total arc122° (108°-136°) total arc0Iwasaki et al7 200945.1100NRT-A; 131 (IQR 108-154)T-A; 191 (IQR 176-206)112° (IQR 95°-129°) total arc128° (IQR 116°-140°) total arc0Lyons et al13 201522.71000NRDASH; 1.4 (0.6-2.1)126° flexion, 21° extension141° flexion, 5° extension1Maniwa et al14 201721.1100NRJOA; 68 (IQR 51.8-84.2)JOA; 98.7 (IQR 96-101.4)NRNRNRMaruyama et al15 201428.4966T-A; 143T-A; 190116° (IQR 95°-137°) total arc,−13° (IQR -27° to +1°) extension, 130° (IQR 110°-140°) flexion133° (IQR 116°-150°) total arc,−13° (IQR -17° to −11°) extension, 136° (IQR 127°-145°) flexion0Matsuura et al16 201743.493NRT-A; 139.7 ± 38.8 (central lesion)T-A; 136.7 ± 36.8 (lateral lesion)T-A; 193.8 ± 9.5 (central lesion)T-A; 185.3 ± 17.6 (lateral lesion)Central lesion: −7.0° ± 16.8 extension, 132.2° ± 10.8 flexionLateral lesion: −8.43° ± 10.8 extension, 130.7° ± 9.3Central lesion: 2.3° ± 5.4 extension, 138.6° ± 6.9 flexion,Lateral lesion: −3.2° ± 8.7 extension, 135.7° ± 7.0 flexionNRMihara et al18 201037.4100NRT-A; 161.4T-A; 185100.7° (87.17°-127.17°) total arc,−12.5° (−24.5° to −0.5°) extension, 119.6° (106.8°-132.4°) flexion117.9° (100°-135.6°) total arc,−7.3° (−17.7° to 3.1°) extension, 126.2° (116.7° - 135.7°) flexion0Mirzayan et al19 201648.4100NRDASH; 35.2DASH; 5.432° lack of extension6° lack of extension2Nishinaka et al21 20142710041T-A; 121.9T-A; 16999° total arc, 118° flexion, −19° extension113° total arc, 124° flexion, −11° extension4Ovesen et al22 201130100NRMayo Elbow Score; 71 (55-85)Mayo Elbow Score; 93.5 (85-100)128° total arc, 137° (120°-140°) flexion, −9.5° (−25° to 0°) extension136.5° total arc, 138.5° (125°-140°) flexion, −2° (−10° to 0°) extension0Pederzini et al25 201748100NRDASH; 44.5DASH; 2.5019.3° (10°-30°) extension,128° (120°-140°) flexion1.2° (0°-3°) extension,138.6° (130°-145°) flexion0Sato et al26 201857100NRT-A; 101T-A; 190101° total arc, −21° extension, 122° flexion132° total arc, −4° extension, 136° flexion2Shimada et al27 201236100NRT-A; 111T-A; 190110° total arc, 126° flexion,16° extension130° total arc, 133° flexion,−3° extension5Shimada et al28 200525.510038JOA; 80.6JOA; 93.8NRNR6Tsuda et al34 200516.3100NRNRT-A; 193130° total arc, 131.7° flexion,−1.7° extensionNRNRUeda et al35 202184100NRT-A; 126T-A; 175112° total arc, 130° flexion,−18° extension127° total arc, 133° flexion,−6° extensionNRWeigelt et al37 20158479NRNRB&M; 95.1NR133° total arcNRYamagami et al39 20183690NRJOA; 74.5JOA; 99.2Central lesion: 130° flexion, −9° extensionLateral localized lesion: 117° flexion, −17° extensionLateral widespread lesion: 128° flexion, −10° extensionCentral lesion: 140° flexion, −2° extensionLateral localized lesion: 137° flexion, −1° extensionLateral widespread lesion: 133° flexion, −6° extension4Yamamoto et al40 2006458911T-A; 150T-A; 181114° total arc126° total arc1B&M, Broberg-Morrey score; DASH, Disabilities of the Arm, Shoulder, and Hand score; IQR, interquartile range; JOA, Japanese Orthopedic Association; NR; Not Reported; T-A, Timmerman-Andrews score.
Patient-reported outcome measures
The mean measurements of function improved postoperatively in all studies. Thirteen studies utilized the TA scoring system; 87% of patients had excellent outcomes with a mean score of 186.4 (range: 169-193.8). Four studies reported outcomes using the DASH scoring system with a mean score of 2.92 (range: 5.4-1.0). Three studies (37 patients) utilizing the JOA scoring system reported a mean score of 97.6 (range: 93.8-99.2). In studies stratifying for lesion location, Matsuura reported significantly higher TA scores at final follow-up for central lesions (193.8 ± 9.5) vs. lateral lesions (185.3 ± 17.6).16 Yamagami reported a significant increase in JOA scores preoperatively to postoperatively in the central (74.5 to 99.2), lateral localized (63.7 to 95.4), and lateral widespread (75.9 to 90.5) cohorts.39 Funakoshi reported similar results with significant TA improvements preoperatively to postoperatively in both central (125 to 193.5) and lateral (138.3 to 186.7) lesion cohorts.6
Range of motion
ROM was reported in 22 of the 24 articles as degrees of total arc, flexion, extension, extension lag, or flexion lag. Preoperative extension data were available for 406 patients and preoperative flexion data were available for 401 patients. These patients had a respective average of 9.1° lack of full extension and 126.8° of flexion preoperatively. Postoperative extension data were available for 416 patients and postoperative flexion data were available for 411 patients. These patients had a respective average of 3.6° lack of full extension and 135.6° of flexion postoperatively. Two studies stratified for lesion location. Matsuura reported significantly better extension postoperatively in central lesion patients vs lateral lesion patients.16 Yamagami reported a significant improvement in ROM preoperatively to postoperatively in both the central lesion and lateral location lesion cohorts.39
Revisions and second looks
All but five studies reported second looks and revisions. The number of revision and second look procedures ranged from 0 to 6 per study. Ayzenberg et al reported two revision procedures in which a back-fill cyst and the removal of a loose body necessitated a second look. Lyons et al reported a single postoperative complication in which irrigation and débridement of a superficial wound infection were performed. Mirzayan et al noted two second-look procedures: one for a flexion contracture and another for areas of fissuring adjacent to the transplanted cartilage. Nishinaka et al reported four revision procedures; two for loose bodies impairing ROM, one spur impairing ROM, and one for screw deviation which avulsed articular cartilage. Sato et al noted two second-look procedures due to the cartilage layer peeling from the graft. Both patients presented with locking symptoms after returning to sport. Shimada et al (2012) noted additional surgery in five patients due to “minor symptoms or for removal of instrumentation.” Shimada et al (2005) reported six reoperations but did not expand upon why reoperations were necessary. Yamagami et al reported four reoperations: one for resection of a loose body, and three for synovectomy or osteochondral plug transplantation. Yamamoto et al reported a single reoperation for the removal of a loose body.
Complications/donor site morbidity
Donor site morbidity was described in 14 of the included articles and affected 26 patients (Table III). Complications of donor site morbidity varied widely across studies ranging from 0% to 62.5% of subjects. Iwasaka et al reported 5 patients (62.5%) who experienced knee joint effusions which lasted a mean of 5 weeks postoperatively.8 The most common complication of the autograft donor site was anterior knee pain with several participants also reporting knee pain exacerbated by high-impact exercise and heavy lifting. Three articles included in our study utilized costal cartilage as an autograft site. One patient experienced a pneumothorax as a complication of harvesting which resolved following chest tube insertion.Table IIIDonor site morbidity.ArticleDonor siteDiscussed donor site morbidity?Proportion of patients affectedDescription of morbidityAllagui et al1 2012Lateral femoral condyleNoNRNRAnsah et al2 2007Lateral femoral condyleYes20.0% (1)Pain with high-impact loads to kneeAyzenberg et al3 2021Lateral femoral condyleYes0NRBilsel et al5 2010Lateral femoral condyleNoNRNRFunakoshi et al6 2018Lateral femoral condyleYes9.09% (2)Mild swelling that occurred after vigorous activitiesIwasaki et al8 2006Lateral femoral condyleYes62.5% (5)Joint effusionIwasaki et al7 2009Lateral femoral condyleYes5.26% (1)Mild anterior knee pain with stair-climbingLyons et al13 2015Lateral femoral condyleYes0NRManiwa et al14 2017Lateral femoral condyleNoNRNRMaruyama et al15 2014Lateral femoral condyleYes3.03% (1)Mild anterior knee pain during exerciseMatsuura et al16 2017Lateral femoral condyleNoNRNRMihara et al18 2010Lateral femoral condyleNoNRNRMirzayan et al19 2016Lateral femoral condyleNoNRNRNishinaka et al21 2014Costal cartilageNoNRNROvesen et al22 2011Lateral femoral condyleYes0NRPederzini et al25 2017Lateral femoral condyleYes0NRSato et al26 2018Costal cartilageYes0NRShimada et al27 2012Costal cartilageYes3.85% (1)PneumothoraxShimada et al28 2005Lateral femoral condyleNoNRNRTsuda et al34 2005Lateral femoral condyleNoNRNRUeda et al35 2021Lateral femoral condyleNoNRNRWeigelt et al37 2015Lateral femoral condyleYes57.1% (8)Seven patients reported occasional pain during heavy lifting. One patient complained about intermittent locking sensationsYamagami et al39 2018Lateral femoral condyleYes23.3% (7)Seven patients required needle aspiration because of postoperative intra-articular hematomaYamamoto et al40 2006Lateral femoral condyleYes0NRNR, not reported.
Discussion
This systematic review demonstrated that OAT for elbow OCD consistently resulted in an excellent rate of RTS and PRO measures. ROM consistently improved, and PROs were excellent in 80%-90% of patients. The only inconsistent finding was the return to previous level of performance (10%-100%), which may be impacted by sport and position played (pitchers).
PROs improved preoperatively to postoperatively across all studies. All studies, apart from Nishinaka et al and Ueda et al, reported postoperative TA scores in the excellent range. In studies stratifying for the location of the OCD lesion, patients with central lesions reported better postoperative outcomes on the TA scale compared to patients with lateral lesions. These findings are consistent with previous work by Logli et al which also reported more favorable outcomes for patients with central lesions.11
Our study found the RTS range among the represented studies was 79%-100% including 498 patients, with all but 5 included studies reporting a RTS rate of 100%. RTS rates in this study are consistent with prior systematic reviews of OAT for OCD. Westerman et al found a RTS rate of 95% in 164 athletes and a return to previous level of play in 94%.38 Average time to RTS was 6 months. Our study found a time to RTS ranging from 4 months to 12 months. Kirsch et al reported a return to play rate of 94% including patients with a mean time of 5.6 months.10
The majority of studies contained an athlete-only population, predominately baseball players. Systematic review by Logli et al reported a return to previous level of performance ranging from 62% to 100% with a range of return to a reduced level of 7%-41%.11 Pitchers had a lower return to the same level, likely due to a higher lateral compressive force when throwing. Several included studies within this systematic review reported considerable rates of return to a reduced level of sport ranging from 0% to 90%. It is important to note that two studies with RTS rates less than 100% report players leaving sports for reasons unrelated to elbow injury.37^,^40 Weigelt et al report 14% of patients and Yamamoto et al report 6% of patients leaving for reasons unrelated to elbow injury. Potential return to a lower level of sport or the need to change positions should be taken into consideration for athletes.
Complication rates were overall low, but donor site morbidity was reported ranging from 0% to 62.5% of patients across studies. Anterior knee pain was the most frequent reported complication with respect to lateral femoral condyle autograft harvesting. Our rates of donor site complications align with a prior systematic review on donor site morbidity by Bexkens et al.4 They postulated that the size of the autograft may increase the complication rate, as some grafts ranged up to 11 mm in diameter. They also noted that the donor site morbidity rates were similar with respect to knee and costal harvesting. The morbidity of costal autograft harvesting could be argued as more significant given the approximation of costal cartilage to the pleura and the potential for pneumothorax. The surgeon and patient should discuss possible morbidity when autograft harvesting is considered.
Limitations
The primary limitation of this study is that it is comprised of level of evidence III and IV studies. Therefore, bias will be present due to differing practice patterns and possible selection bias. Additionally, surgical indications may vary between studies which can limit comparisons. Another limitation is the variability in reported outcome measures and follow-up. Additional higher level of evidence studies, including comparative treatment studies, are needed to provide more definitive conclusions.
Conclusions
Following OAT for capitellar OCD lesions, RTS rates are high; however, athletes should be counseled on the potential of a return to lower performance or the need to change positions. Lateral lesion location may negatively impact outcomes. PRO scores are typically excellent and postoperative ROM consistently improves. This information helps counsel patients regarding expectations and outcomes of OAT for OCD of the capitellum
Disclaimers:
Funding: Dr. Coronado was supported by a Vanderbilt Clinical and Translational Research Scholars award (NIH/NCATS KL2TR002245) during the time of this manuscript.
Conflicts of interest: The authors, their immediate families, and any research foundation with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Allagui M.Koubaa M.Bellaj Z.Amara K.Aloui I.Hamdi M.F.Osteochondritis dissecans of the capitellum: Autologous osteochondral mosaicplasty. A case report Chir Main 31201220620910.1016/j.main.2012.07.00322980988 · doi ↗ · pubmed ↗
- 2Ansah P.Vogt S.Ueblacker P.Martinek V.Woertler K.Imhoff A.B.Osteochondral transplantation to treat osteochondral lesions in the elbow J Bone Joint Surg Am 8920072188219410.2106/jbjs.F.0029917908895 · doi ↗ · pubmed ↗
- 3Ayzenberg M.Clippinger B.Slate E.L.Kozin S.H.Zlotolow D.A.Outcomes of osteochondral autograft transplantation in pediatric patients with osteochondritis dissecans of the capitellum J Hand Surg Am 4620211028.e 11028.e 1510.1016/j.jhsa.2021.02.02433902975 · doi ↗ · pubmed ↗
- 4Bexkens R.Ogink P.T.Doornberg J.N.Kerkhoffs G.Eygendaal D.Oh L.S.Donor-site morbidity after osteochondral autologous transplantation for osteochondritis dissecans of the capitellum: a systematic review and meta-analysis Knee Surg Sports Traumatol Arthrosc 2520172237224610.1007/s 00167-017-4516-828391550 PMC 5489608 · doi ↗ · pubmed ↗
- 5Bilsel K.Demirhan M.Atalar A.C.Akkaya S.A new surgical technique to facilitate osteochondral autograft transfer in osteochondral defects of the capitellum: a case report Acta Orthop Traumatol Turc 442010828710.3944/AOTT.2010.223520513997 · doi ↗ · pubmed ↗
- 6Funakoshi T.Momma D.Kamishima T.Matsui Y.Kawamura D.Nagano Y.Autologous osteochondral mosaicplasty for centrally and laterally located, advanced capitellar osteochondritis dissecans in teenage athletes: clinical outcomes, radiography, and magnetic resonance imaging findings Am J Sports Med 4620181943195110.1177/036354651876827929738680 · doi ↗ · pubmed ↗
- 7Iwasaki N.Kato H.Ishikawa J.Masuko T.Funakoshi T.Minami A.Autologous osteochondral mosaicplasty for osteochondritis dissecans of the elbow in teenage athletes J Bone Joint Surg Am 9120092359236610.2106/jbjs.H.0126619797570 · doi ↗ · pubmed ↗
- 8Iwasaki N.Kato H.Ishikawa J.Saitoh S.Minami A.Autologous osteochondral mosaicplasty for capitellar osteochondritis dissecans in teenaged patients Am J Sports Med 3420061233123910.1177/036354650628634316567456 · doi ↗ · pubmed ↗