An uncommon electrocardiogram presentation of bigeminy: ECG Challenge
Avinash Jeewooth, Atul Kaushik, Aparna Jaswal

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
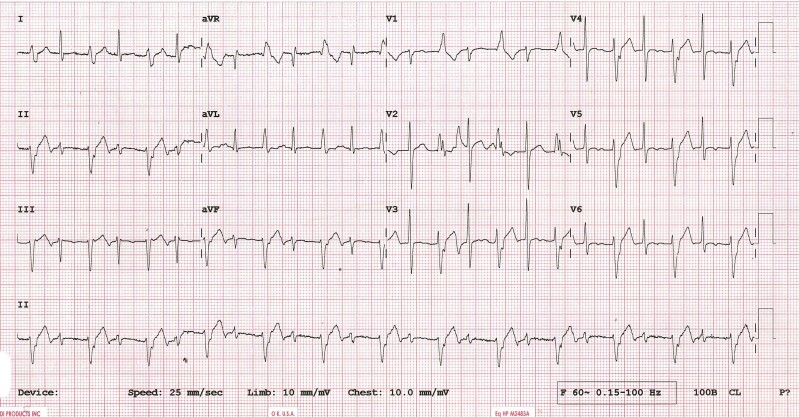 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Cardiomyopathy and Myosin Studies · Cardiac pacing and defibrillation studies
A 52-year-old male with a past history of hypertension, presented with pre-syncope for 15 days. His electrocardiogram is shown in Figure 1. His 2D echocardiogram (ECG), Cardiac-MRI, and coronary angiography were normal.
Question 1
The ECG shows an alternating pattern of narrow QRS complex with wider QRS complex. What is the likely diagnosis?
Ventricular bigeminy.Atrial bigeminy with aberrancy.Ventricular tachycardia with capture beats.Ventricular tachycardia with fusion beats.SVT with aberrancy.
Answer: C.
Discussion and explanation
The heart rate in the ECG is around 120 b.p.m.
The wider QRS complex has a right bundle branch block pattern with a superior axis. The QRS duration of the complex is around 120 msec. The RS interval in the precordial leads is short. The broad complexes were not preceded by P waves. These findings favour a ventricular tachycardia (VT) originating close to the conduction system. The diagnosis is left posterior fascicular VT with alternating capture beats.
The narrower QRS complex is a capture beat. These beats are more commonly seen when the tachycardia rate is slow. The rate of the VT was unchanged.
Kindly refer to Supplementary material online, ImageS1, for details.
Question 2
Which pharmacological drug is most effective against idiopathic fascicular VT?
Lidocaine.Esmolol.Amiodarone.Verapamil.Adenosine.
Answer: D.
Discussion and explanation
Verapamil is the first-line treatment for acute termination of fascicular VT (ESC Guidelines Class IC recommendation).^1^ Fascicular VT is a macro-reentrant tachycardia which incorporates LPF as one limb of the circuit and abnormal Purkinje tissues as the other limb. These abnormal Purkinje tissues are calcium-dependent and hence the name ‘verapamil-sensitive idiopathic LV-VT’.
Question 3
What is the best chronic management option for this patient?
Catheter ablation.Observation.Medical therapy.No follow-up required.Coronary angioplasty.
Answer: A.
Discussion and explanation
Catheter ablation is highly effective with a reported success rate of >85%.^2^
Kindly refer to Supplementary material online, Image S2, for details.
Supplementary Material
ytae392_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zeppenfeld K , Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA, et al 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022;43:3997–4126.36017572 10.1093/eurheartj/ehac 262 · doi ↗ · pubmed ↗
- 2Schneider HE , Kriebel T, Jung K, Gravenhorst VD, Paul T. Catheter ablation of idiopathic left and right ventricular tachycardias in the pediatric population using noncontact mapping. Heart Rhythm 2010;7:731–739.20193776 10.1016/j.hrthm.2010.02.031 · doi ↗ · pubmed ↗