Three-Level Concavity Apical Pediculectomy During Intraoperative Neuromonitoring Loss: Following the Checklist Resulted in an Ambulatory Patient
Danner W Butler, Tyler C McDonald, Sudhir Suggala, Richard Menger

TL;DR
This paper discusses a surgical case where intraoperative neuromonitoring was lost but successfully recovered using checklist-guided procedures in a scoliosis patient.
Contribution
The paper presents a case study demonstrating the successful application of operative guidelines to recover neuromonitoring signals during scoliosis surgery.
Findings
Loss of TcMEPs and SSEPs during surgery was managed using consensus guidelines.
Post-operative recovery of neuromonitoring signals was achieved.
The patient remained ambulatory following the procedure.
Abstract
Adolescent idiopathic scoliosis is the most common form of scoliosis, with severe cases leading to a decline in patients with worsening angulation of deformity. Technical nuances of spinal flexibility and cord type based on the extent of the deformity may impact operating safety and outcome, with risks including neurological loss during and after surgical intervention. Here we present a case of posterior osteotomy and correction of a patient with adolescent idiopathic scoliosis with a T2 - L3 fusion in which transcranial motor evoked potentials (TcMEPs) and somatosensory evoked potentials (SSEPs) were lost intraoperatively, thus requiring application of operative consensus guidelines for the loss of neuromonitoring data. Particularly, the discussion focuses on the decision-making process that resulted in the complete recovery of TcMEPs and SSEPs post-operatively.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
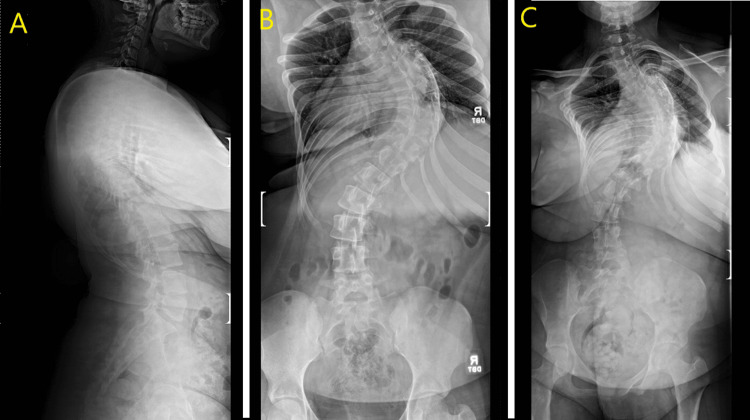 Figure 1
Figure 1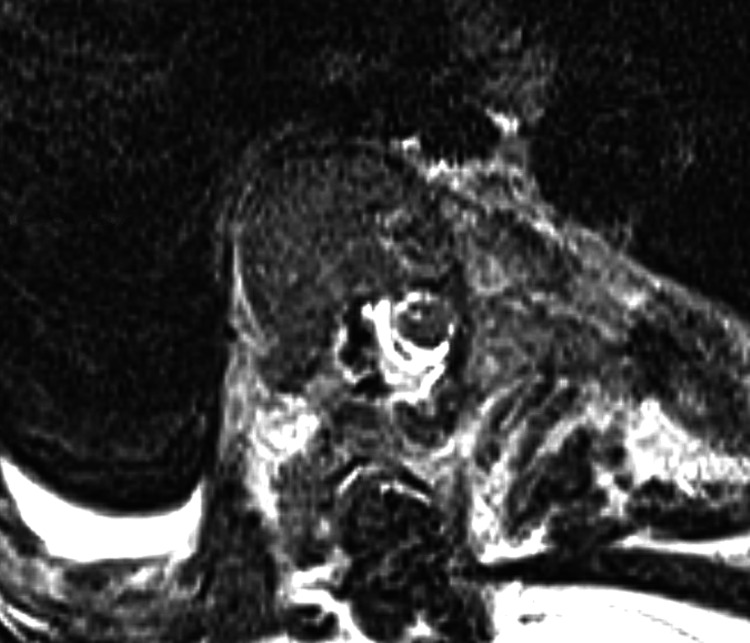 Figure 2
Figure 2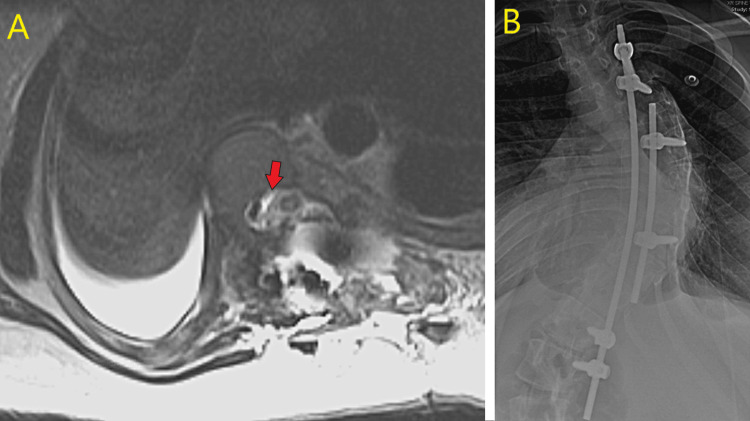 Figure 3
Figure 3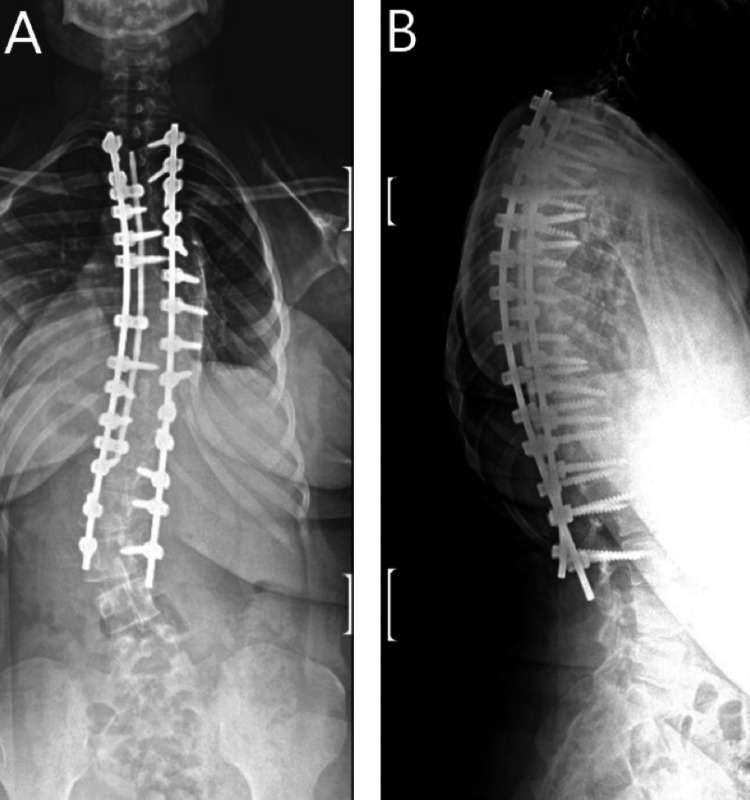 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraoperative Neuromonitoring and Anesthetic Effects · Scoliosis diagnosis and treatment · Spinal Fractures and Fixation Techniques
Introduction
Adolescent idiopathic scoliosis (AIS) is the most common form of scoliosis, affecting between 1-3% of the population [1]. Defined as a spinal curvature of greater than 10 degrees, AIS consists of a coronal, sagittal, and rotational plane deviation [1]. Beyond 50 degrees of curvature, AIS defects can result in major adverse health conditions such as debilitating back pain and body dysmorphia and may even progress to decreased pulmonary function once curvature has reached 90 degrees [2-4]. While orthotic management may suffice between 25-50-degree deficits, surgical intervention is recommended once curvature has increased beyond a 50-degree angle. Technical nuances of flexibility, spinal cord type, and lung or cardiac function may impact operating safety and overall outcome [2-5]. Complications, including neurological loss, must additionally be considered, both pre-operatively and intraoperatively during the decision-making process [6-7].
Additionally, increasing deformity angle ratios (DAR), or curve magnitude per level of spinal deformity, increases risks of intraoperative neuromonitoring loss, thus necessitating further pre-operative consideration for higher DARs [4]. Recent guidelines established by Vitale et al. and more recently, Lenke et al, have provided algorithmic methodology in the surgical management of both unstable and stable complex spine cases [8, 9]. Such guidelines were established by groups of expert spine surgeons, with a focus on creating a team approach to crisis situations. While guidelines are established, clinical case reports of the effectiveness of such decision-making processes remain limited.
Here we present a case of posterior osteotomy and correction of a patient with AIS in which transcranial motor evoked potentials (TcMEPs) and somatosensory evoked potentials (SSEPs) were lost intraoperatively. Discussion focuses on the stepwise decision-making process and application of consensus guidelines for surgeon decisions during neuromonitoring changes, as established by Vitale et al. and more recently, Lenke et al [8, 9]. The patient had complete recovery of TcMEPs and SSEPs post-operatively. We explore the technical lessons learned from this experience.
Case presentation
A 13-year-old female originally presented in 2019 with evidence of scoliosis showing approximately 100 degrees of curvature, improving to 90 degrees with traction film. The patient re-presented in 2023 with worsening back pain. Physical exam revealed bilateral strength 5/5 in the upper and lower extremities, as well as sensation intact to bilateral lower extremities globally (Figure 1).
Pre-operative standing X-ray showing A) sagittal view, B) anteroposterior (AP) view, and C) posteroanterior (PA) view of spinal deformity
However, MRI revealed a type 3 spinal cord as well as a small right pleural effusion, concerning for a diagnosis of AIS affecting pulmonary status (Figure 2) [7].
Axial MRI T2 imaging showing a Type 3 spinal cord at the apex.
Her deformity angular ratio (DAR) was 12.25 in the coronal plane, 8.875 in the sagittal plane, and 21.125 overall [4]. Subsequently, she was indicated for complex spine reconstruction through the pediatric spine complex care pathway. This is a two-attending model with orthopedic surgery and neurosurgery. Patient consent was obtained. IRB approval was not required for this single-patient case report.
A T2 - L3 incision was performed under 15 lb traction. Upon completion of facetectomy, posterior column osteotomies were planned. The T10 - T11 osteotomy was performed without any unexpected events. Subsequently, during the T9 - T10 osteotomy, left lower extremity TcMEPs met alert criteria to complete loss furthered by unilateral complete loss of left-sided SSEPs.
The best-practices guidelines were applied for the loss of neuromonitoring [9]. An immediate increase of mean arterial pressure (MAP) was performed via closed-loop communication with the senior anesthesia provider. Upon releasing traction, we looked to shorten the spinal cord and protect against any drift against the medial pedicle. We elected to place a rod on the right side of the periapical levels to enact compression on the convex (right) side. We then placed pedicle screws at T7 and T10 via the freehand method on the convex side before connecting a titanium rod between the two and compressing these levels. This afforded some slight improvement in neuromonitoring signals, but signals were still concerning with no large improvement. After a half hour, with proper MAP maintenance showing no improvement, we made the decision to give Solumedrol at 30 mg/kg for the next hour.
According to the guidelines, an outside surgeon, in this case a third surgeon, was called for finite decision-making. This confirmed our decision matrix of either contusion from PCO (posterior column osteotomy) or spinal cord shift. The wake-up test would not change immediate management and a pedilectomy was indicated.
The T7, T8, and T9 periapical pedicles on the concave side were removed before the lamina on the left side. The pedicles were carefully resected while protecting the underlying spinal cord and nerve root. The left/ventral aspect of the pedicles/ventral wall was removed as well. There was visual kinking at T7 - T9, and upon release, the spinal cord was seen to show pulsations. The SSEPs returned to above alert level, and the left psoas and abdomen/foot TcMEP signal returned as well. At this point, we decided to place a provisional fixation and end the case. We placed pedicle screws at T4, T5, L1, and L2 on the right side before a 5.5mm titanium rod was cut and bent to match the in-situ positioning and placed into these pedicle screws. The immediate post-operative wake-up test was full strength.
The patient was monitored inpatient for one week with no neuromuscular deficits noted. MRI was performed post-operatively showing a T2 hyperintensity at the apex of the spinal cord at T8 (Figure 3).
(A) Axial T2 hyperintensity at the cord apex status post pediculectomy; (B) Intraoperative temporary fixation.
With reassurance of stable neurological function, in consultation with other colleagues, the surgical wound was reopened, and proper instrumentation was placed for T2 - L3 fusion. At three month follow-up, the patient reported markedly reduced back pain with 5/5 strength bilaterally. Imaging revealed stable instrumentation with alignment well maintained (Figure 4).
Anteroposterior (A) and lateral (B) post-operative X-ray showing T2 - L3 fusion.
Discussion
Observations
There were several preoperative warning criteria in this case that resulted in a high risk of complication. The first is the high deformity angular ratio (DAR), as the patient had a curve over 100 degrees. A combined DAR of over 20 has a substantially higher risk of neuro-monitoring loss [4]. Additionally, the patient had a type 3 cord compression, defined as when no cerebrospinal fluid (CSF) is any longer visible around the spinal cord on MRI [10]. This contrasts with a type 1 cord, which only involves an epidural extension, and type 2, in which CSF is still visible around the cord 7. A type-3 compression has a 28 times higher risk of having an intraoperative neuromonitoring loss [5]. Lastly, unlike typical AIS, there was also a kyphotic component to the deformity, of which surgical correction may stretch the anterior-based watershed vasculature.
Application of best practice guidelines
Recent clinical guidelines have established the necessity of organized, team-based thinking in cases of intraoperative neuromonitoring loss (IONM) in both the stable and unstable spine. Vitale et al established a step-by-step process in IONM changes in the stable spine, highlighting the need to (1) gain control of the room as the surgeon, (2) address anesthetics (optimize MAP, hematocrit, pH and partial pressure of carbon dioxide (pCO2), consider wake-up test), (3) assure proper technical/neuro-physiological setup, and (4) address surgical needs going forward [8]. Furthermore, and more specifically in our case, Lenke et al. expanded on the unstable spine, addressing the need for similar stepwise, team-based thinking [9]. Our specific case qualified as a Stage 2a alert, as destabilization occurred after posterior column osteotomy. Subsequently, we followed the outlines defined by Lenke et al., opting to 1) remove traction, 2) stabilize with temporary rods, and 3) assess for dural compression and perform necessary pediculectomy for relief [9]. Descending neurogenic-evoked potentials were not available to assess further levels of dysfunction in our case. This “stepwise” level of thinking was consistently followed, eventually leading to a full recovery for our patient.
Lessons
Instrumentation should be placed before posterior column osteotomies on the convexity side above and below the main apex prior to osteotomy. A temporary rod can be placed to stabilize as any type of compression will shorten the spine. This may reduce the technical difficulty of a concavity PCO as well as protect against any shift migration. These are the two most likely causes of intraoperative neuromonitoring loss.
Conclusions
In the operating room, cases may not go as planned, leading to the need for stepwise decision-making to ensure further crisis is averted. This case report highlights such an instance, providing evidence of the effectiveness of adhering to the suggested guidelines established to handle complex spinal deformity cases with a level mind. In addition, the case is an example of the team-based practices that are necessary to handle crisis situations within the operating room. Timing of instrumentation and posterior column osteotomies are an additional surgical lesson of the reported case. Continued reflection upon such difficult cases allows for the betterment of patient care and surgical performance in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Scoliosis: review of diagnosis and treatment Paediatr Child Health Janicki JA Alman B 7717761220071903046310.1093/pch/12.9.771PMC 2532872 · doi ↗ · pubmed ↗
- 2Screening for adolescent idiopathic scoliosis: evidence report and systematic review for the US Preventive Services Task Force JAMA Dunn J Henrikson NB Morrison CC Blasi PR Nguyen M Lin JS 17318731920182931828310.1001/jama.2017.11669 · doi ↗ · pubmed ↗
- 3Deformity angular ratio is associated with neuromonitoring changes without a vertebral column resection: spinal deformity is more influential than type of surgery Spine Deform Illingworth KD Siddiqui AA Skaggs DL Andras LM 9519561120233693044010.1007/s 43390-023-00669-y PMC 10261247 · doi ↗ · pubmed ↗
- 4Total deformity angular ratio as a risk factor for complications after posterior vertebral column resection surgery J Korean Neurosurg Soc Lee BH Hyun SJ Han S Jeon SI Kim KJ Jahng TA Kim HJ 7237306120183039624510.3340/jkns.2018.0125 PMC 6280056 · doi ↗ · pubmed ↗
- 5Adolescent idiopathic scoliosis: risk factors for complications and the effect of hospital volume on outcomes Neurosurg Focus Menger RP Kalakoti P Pugely AJ Nanda A Sin A 043201710.3171/2017.6.FOCUS 1730028965456 · doi ↗ · pubmed ↗
- 6Adolescent idiopathic scoliosis and mental health disorders: a narrative review of the literature Children (Basel) Mitsiaki I Thirios A Panagouli E 9202210.3390/children 9050597 PMC 913926235626775 · doi ↗ · pubmed ↗
- 7A novel MRI-based classification of spinal cord shape and CSF presence at the curve apex to assess risk of intraoperative neuromonitoring data loss with thoracic spinal deformity correction Spine Deform Sielatycki JA Cerpa M Baum G Pham M Thuet E Lehman RA Lenke LG 655661820203220705810.1007/s 43390-020-00101-9 · doi ↗ · pubmed ↗
- 8Best practices in intraoperative neuromonitoring in spine deformity surgery: development of an intraoperative checklist to optimize response Spine Deform Vitale MG Skaggs DL Pace GI 333339220142792733010.1016/j.jspd.2014.05.003 · doi ↗ · pubmed ↗