Drug-Induced Acute Eosinophilic Pneumonia With Pneumomediastinum: An Unusual Presentation
Vasu Agarwal, Sidhaant Nangia, Shaily Prasenan, Siri Vineeth A Ganta

TL;DR
A woman developed a rare lung condition after taking an alternative medication, which was successfully treated with steroids.
Contribution
This case report highlights drug-induced eosinophilic pneumonia with pneumomediastinum linked to non-conventional medication.
Findings
The patient showed bilateral ground-glass opacities and pneumomediastinum on CT scans.
Eosinophilia was confirmed via bronchoalveolar lavage, leading to a diagnosis of drug-induced lung disease.
Symptoms and radiographic findings resolved after discontinuing the medication and starting corticosteroids.
Abstract
A 27-year-old female, with no significant past medical history, presented to the casualty department with a two-week history of progressive dyspnea, cough, and fever. She reported that she had recently started taking a non-conventional alternative medication for her irregular menstrual cycles. Chest radiography demonstrated bilateral alveolar opacities, and computed tomography (CT) of the chest revealed bilateral ground-glass opacities and pneumomediastinum. Laboratory testing showed peripheral blood eosinophilia, and bronchoscopy with bronchoalveolar lavage confirmed an elevated eosinophil count. Based on the clinical presentation, radiographic and laboratory findings, and exclusion of other etiologies, a diagnosis of drug-induced eosinophilic lung disease with pneumomediastinum was made. The alternative non-conventional drug was immediately discontinued and the patient was treated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
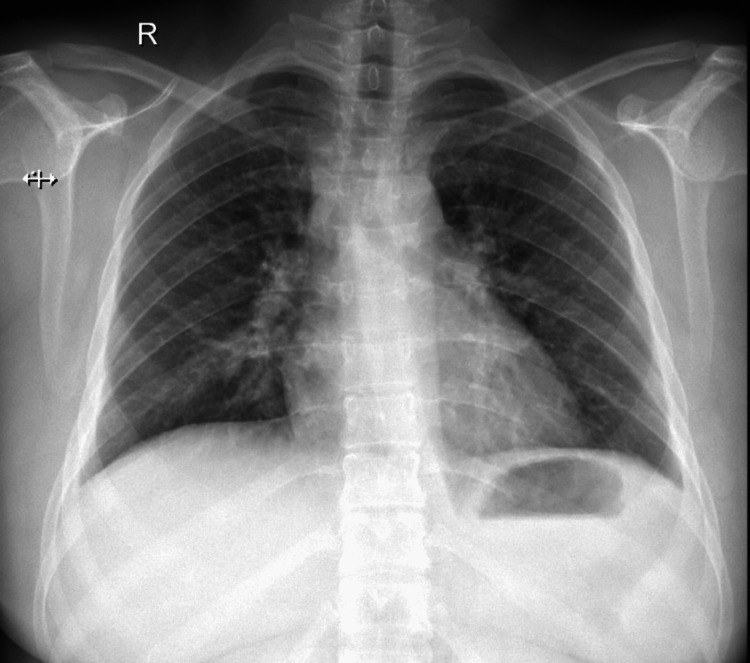 Figure 1
Figure 1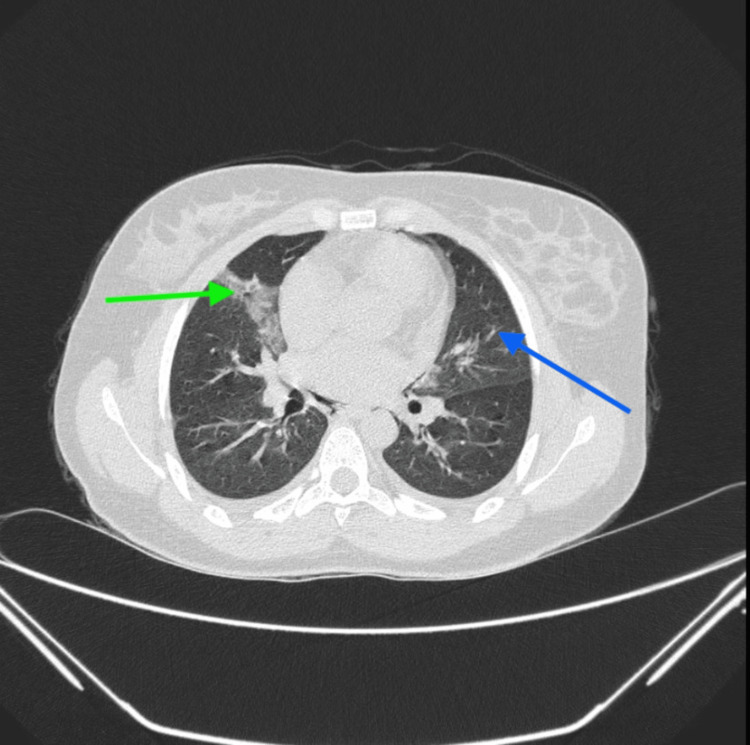 Figure 2
Figure 2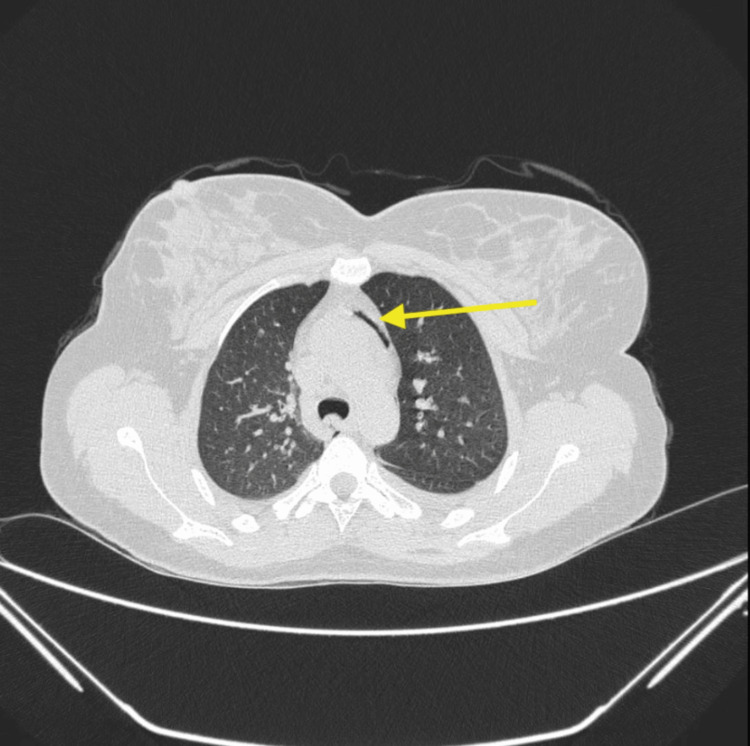 Figure 3
Figure 3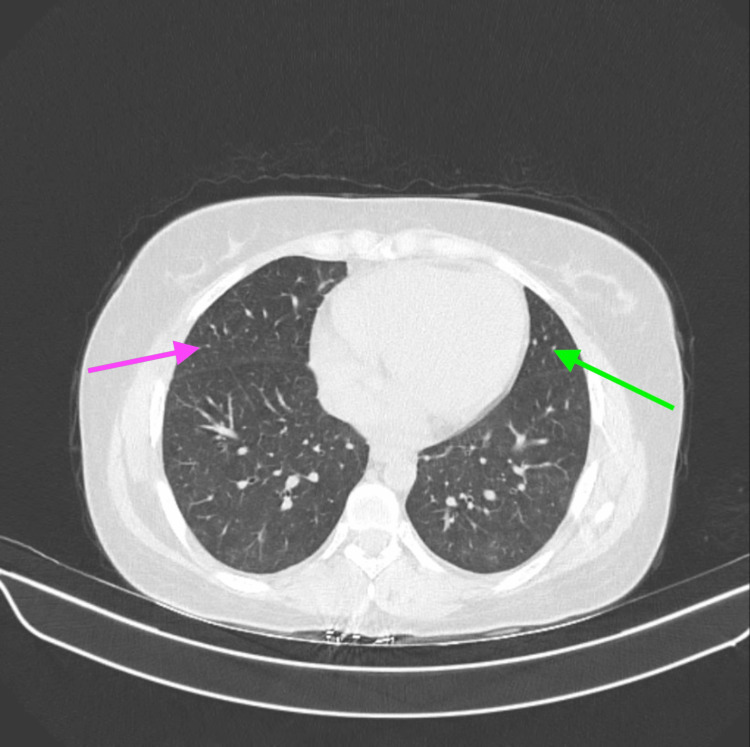 Figure 4
Figure 4| Complete Blood Count (EDTA Whole Blood) | Result | Biological Reference Interval |
| Hemoglobin (Hb) | 11.90 | 11.6 - 15.0 g/dL |
| Total leucocyte (WBC) count | 14,100 | 4000-10000/µL |
| Platelet count | 171,000 | 150000 - 410000 /µL |
| Red blood cell (RBC) count | 4.55 | 3.92 - 5.13 x 10^6 /µL |
| Neutrophils | 51 | 40 - 80 % |
| Absolute neutrophils | 7,191 | 2000 - 7000 /µL |
| Eosinophils | 11 | 1 – 6 % |
| Absolute eosinophils | 1,551 | 20 - 500 /µL |
| Basophils | 0 | 0 – 2 % |
| Absolute basophils | 0 | 0 - 100 /µL |
| Lymphocytes | 30 | 20 – 40 % |
| Absolute lymphocytes | 4,230 | 1000 - 3000 /µL |
| Monocytes | 8 | 2 - 10 % |
| Absolute monocytes | 1,128 | 200 - 1000 /µL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumothorax, Barotrauma, Emphysema · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Eosinophilic Disorders and Syndromes
Introduction
Eosinophilic pneumonia is a rare disease caused by smoking [1], hypersensitivity reaction to drugs like antibiotics and non-steroidal anti-inflammatory drugs (NSAIDs) [2], parasitic infestations [3], and viral illnesses [4]. Drug-induced eosinophilic pneumonia manifests as acute or chronic pneumonia, accompanied by a history of drug intake and clinical improvement upon drug cessation. This is believed to be caused by a hypersensitivity reaction to the drug, leading to an eosinophilic lung infiltration with alveolar lung infection [1]. In our case, the patient had consumed non-conventional alternative medicine a few days before her presentation to the hospital with both acute eosinophilic pneumonia (AEP) and pneumomediastinum. There is insufficient literature to show a causal link between AEP and pneumomediastinum. The uniqueness of the case lies in the fact that soon after the drug consumption, the patient presented with both clinical disorders simultaneously. The drug-induced hypersensitivity reaction may have led to bronchial constriction and alveolar damage, causing an air leak from the alveoli into the mediastinum. Since the symptoms are vague, AEP diagnosis necessitates peripheral blood eosinophilia, bronchoalveolar lavage (BAL) eosinophilia, or a lung biopsy showing eosinophilic infiltration in the lung [5-8]. Pneumomediastinum, on the other hand, is mostly diagnosed radiologically [9]. The treatment revolves around corticosteroids for AEP [7] and symptomatic management for pneumomediastinum [10].
Case presentation
A 27-year-old female with no significant past medical history presented to our casualty with complaints of progressive breathlessness, dry cough, and fever for the last two weeks. The patient was tachycardic and tachypnoeic and had bilateral polyphonic rhonchi on lung auscultation. A subcutaneous emphysema in the neck was also detected, which was a surprising presentation because she had no history of any trauma, surgical procedures, mechanical ventilation, tracheostomy, or central venous catheter insertion, which might have caused the subcutaneous emphysema. The initial working diagnosis was of an acute infective exacerbation of bronchial asthma along with pneumomediastinum. She was subsequently admitted to the general ward and initiated on intravenous broad-spectrum antibiotics, nebulization with bronchodilators for the bronchoconstriction, inhaled corticosteroids along with intravenous systemic corticosteroids, and highly concentrated oxygen for the subcutaneous emphysema. The chest radiograph had no apparent lung parenchymal involvement (Figure 1).
Plain chest radiograph with no apparent abnormalities
A high-resolution computed tomography (HRCT) scan of the thorax showed mild bilateral pleural effusion with bilateral ground-glass opacities and a pneumomediastinum (Figures 2, 3).
High-resolution computed tomography (HRCT) thorax with ground-glass opacities in the anterior and medial basal segments of the right lower lobe (green arrow) and the anteromedial segment of the left lower lobe (blue arrow)
High-resolution computed tomography (HRCT) thorax with pneumomediastinum in the neck (yellow arrow)
A routine blood test showed a raised total leukocyte count suggestive of infection and peripheral blood eosinophilia, around 11%, with an absolute eosinophilic count of 1551 cells/microliter above the normal limits (Table 1).
Eosinophilia was unexplained, as the patient had no history of atopy, had not eaten any food from outside the home, had not traveled recently, and had no exposure that might have caused a parasitic infestation leading to eosinophilia. On thorough history-taking, the patient reported recent consumption of a non-conventional alternative medicine for her irregular menstrual cycles. Because the medication was a non-conventional drug therapy, it was impossible to determine its contents. We sent a serum immunoglobulin E assay, which came back significantly elevated above the normal limits. Suspecting a diagnosis of acute eosinophilic pneumonia, possibly due to drug consumption, we performed a bronchoscopy, and significant eosinophilia (more than 5%) was detected in the bronchoalveolar lavage (BAL). BAL cultures, as well as blood and urine cultures, were negative for microbial growth; ruling out an alternative explanation to her underlying pneumonia. We continued the patient on broad-spectrum intravenous antibiotics as prophylaxis, nebulized bronchodilators for her bronchoconstriction, and intravenous corticosteroids for AEP. We stopped the non-conventional alternative medication immediately and after a few days, the patient showed clinical improvement in symptoms and resolution of subcutaneous emphysema. The patient was successfully discharged and later on in the follow-up, the repeat HRCT thorax showed significant resolution of ground-glass opacities and a complete resolution of pneumomediastinum (Figure 4).
High-resolution computed tomography (HRCT) thorax showing a resolution of ground-glass opacities in the right lung parenchyma (pink arrow) and left lung parenchyma (green arrow)
Discussion
Acute eosinophilic pneumonia (AEP) is a rare disease, most commonly affecting younger men with a history of smoking [1]. Other causative factors include drug-induced eosinophilia [2], recreational use of inhalation drugs like cocaine [11] and marijuana [12], parasitic [3], fungal [13], and viral [4] infections. The development of eosinophilic lung disease in this patient was likely a consequence of the alternative non-conventional medicine she had recently started taking. Eosinophilic lung disease has been reported as an adverse effect of various conventional medications, including antibiotics, antidepressants, and nonsteroidal anti-inflammatory drugs [2]. However, it is an uncommon complication of complementary and alternative medicines. Although the pathogenesis remains incompletely understood, it could potentially involve a hypersensitive immune response by alveolar macrophages to the drug constituents [1]. The offending agent interacts directly with bronchial and alveolar cells, which then release T helper-2 (Th2) cytokines, interleukin-5,8,33 (IL-5, IL-8, IL-33), and eosinophils [14-16]. Drugs known to cause eosinophilic pneumonia accumulate in the alveoli leading to epithelial injury and inflammation [2]. Solomon and Schwarz proposed five criteria for the diagnosis of AEP; these include the presence of acute, simple, or chronic eosinophilic pneumonia, the presence of a potential drug, ruling out of other causes, a clinical improvement on the cessation of the drug, recurrence of the disease on the drug being reintroduced [1]. Our patient fulfilled the criteria. The clinical features of AEP include an acute disease characterized by nonproductive cough, dyspnea, fever, malaise, and night sweats, along with peripheral blood eosinophilia, BAL eosinophilia, or eosinophilic infiltration of the lung tissue, as observed on a biopsy [5-8]. Additionally, the patient presented with bilateral patchy areas of ground-glass opacities, interlobular septal thickening, centrilobular nodules [17,18], and bilateral pleural effusion. These infiltrates usually resolve within days of starting corticosteroid treatment [7]. A diagnosis of pneumomediastinum is mainly based on radiology. On a chest radiograph, the presence of subcutaneous emphysema, air around the pulmonary vein, and a continuous diaphragm sign indicated pneumomediastinum [10]. There is not enough literature on any causal association between pneumomediastinum and acute eosinophilic pneumonia. Maybe a drug-induced hypersensitivity reaction is causing bronchial constriction, airway injury, and increased alveolar pressures, ultimately leading to alveolar rupture and pneumomediastinum [9]. Treatment of pneumomediastinum is mostly supportive, focusing on the removal of subcutaneous emphysema with high-flow oxygen delivery and pain management, possibly from the air under the skin [9]. The patient's presentation was suggestive of acute infective exacerbation of bronchial asthma leading to pneumomediastinum. Only a thorough and accurate medical history could exclude asthma and disclose the history of drug consumption. Unfortunately, due to the drug's association with a non-conventional alternative medical regime, it was not possible to definitively identify the causative agent or chemical. The case's rarity lies in its short exposure history, resulting in two separate clinical conditions appearing simultaneously and rapidly resolving with appropriate treatments.
Conclusions
This case highlights the potential dangers of consuming non-conventional alternative medicines where the chemical contents of the medicine are unknown. The patient received these medicines, from a local practitioner, in a packet with no label mentioning the contents of the medicine. Since non-conventional alternative medicine is a mix of herbal medicines, they rarely mention the chemical components of their drugs, it is thus difficult to ascertain the exact nature of the medicine taken. After ruling out all other possible differential diagnoses and as the patient had not taken any other medicine apart from the non-conventional alternative medicine, it was concluded that the patient experienced acute eosinophilic pneumonia as a result of a hypersensitivity reaction to the non-conventional alternative medicine. Pneumomediastinum represents a very unusual complication of this presentation, and the patient has had no other underlying lung condition, on presentation or in the past, to give rise to the same. To our knowledge, this is the first case report of a spontaneous pneumomediastinum associated with drug-induced acute eosinophilic lung disease. Acute eosinophilic pneumonia could thus be an important differential in patients presenting with pneumomediastinum. Early diagnosis and prompt withdrawal of the offending agent, along with corticosteroid therapy, led to a rapid resolution of symptoms and radiographic abnormalities. This case emphasizes the importance of taking a thorough history, especially when inquiring about drug history. Since most non-conventional alternative treatment regimes rarely disclose the chemicals present in their drugs, the risk of adulteration of such medications increases, which can then lead to serious health risks, as we have seen in our patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute eosinophilic pneumonia. Causes, diagnosis, and management Am J Respir Crit Care Med De Giacomi F Vassallo R Yi ES Ryu JH 72873619720182920647710.1164/rccm.201710-1967 CI · doi ↗ · pubmed ↗
- 2The drug-induced respiratory disease website. Pneumotox Camus P https://www.pneumotox.com/drug/index/
- 3Eosinophilic pneumonia due to visceral larva migrans possibly caused by Ascaris suum: a case report and review of recent literatures Jpn J Infect Dis Izumikawa K Kohno Y Izumikawa K Hara K Hayashi H Maruyama H Kohno S 428432642011 https://pubmed.ncbi.nlm.nih.gov/21937827/21937827 · pubmed ↗
- 4A case of acute eosinophilic pneumonia triggered by the SARS-Co V-2 virus Cureus De Albuquerque Monteiro I Fernandes Moura P Fernandes D Carneiro JC Teixeira S 015202310.7759/cureus.38111 PMC 1021139837252582 · doi ↗ · pubmed ↗
- 5Idiopathic acute eosinophilic pneumonia: a study of 22 patients Am J Respir Crit Care Med Philit F Etienne-Mastroïanni B Parrot A Guérin C Robert D Cordier JF 1235123916620021240369310.1164/rccm.2112056 · doi ↗ · pubmed ↗
- 6A clinical study of idiopathic eosinophilic pneumonia Chest Hayakawa H Sato A Toyoshima M Imokawa S Taniguchi M 146214661051994 http://10.1378818133810.1378/chest.105.5.1462 · doi ↗ · pubmed ↗
- 7Clinical characteristics and corticosteroid treatment of acute eosinophilic pneumonia Eur Respir J Rhee CK Min KH Yim NY Lee JE Lee NR Chung MP Jeon K 4024094120132259935910.1183/09031936.00221811 · doi ↗ · pubmed ↗
- 8Acute eosinophilic pneumonia. A summary of 15 cases and review of the literature Medicine (Baltimore) Pope-Harman AL Davis WB Allen ED Christoforidis AJ Allen JN 334342751996898215010.1097/00005792-199611000-00004 · doi ↗ · pubmed ↗