SARS-CoV-2 as a potential trigger for microscopic colitis in a young adult: A case report
A. Alwali, C. Schafmayer, F. Prall, I. Kamaleddine

TL;DR
A young adult developed chronic diarrhea after a SARS-CoV-2 infection, which was later diagnosed as lymphocytic colitis and successfully treated with budesonide.
Contribution
This case report suggests SARS-CoV-2 may trigger microscopic colitis, highlighting a potential post-COVID-19 gastrointestinal complication.
Findings
Chronic diarrhea and abdominal pain persisted for 10 months after SARS-CoV-2 infection.
Colonoscopy biopsies showed moderate lymphocytic infiltration consistent with lymphocytic colitis.
Symptoms resolved completely with budesonide treatment.
Abstract
This case highlights the potential role of SARS-CoV-2 in triggering lymphocytic colitis, emphasizing the need for further research and vigilance in identifying potential post-COVID-19 GI complications. We describe a case of a young adult who experienced chronic diarrhea and abdominal pain for 10 months after a SARS-CoV-2 infection. Extensive laboratory and imaging investigations yielded no significant findings. Despite a preliminary diagnosis of irritable bowel syndrome and symptomatic treatment, symptoms persisted. Colonoscopy with biopsies revealed unremarkable colonic mucosa but confirmed moderate lymphocytic infiltration consistent with lymphocytic colitis. Treatment with budesonide achieved complete symptom resolution. The findings underscore the importance for clinicians to consider triggered microscopic colitis in patients presenting with persistent diarrhea following SARS-CoV-2…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
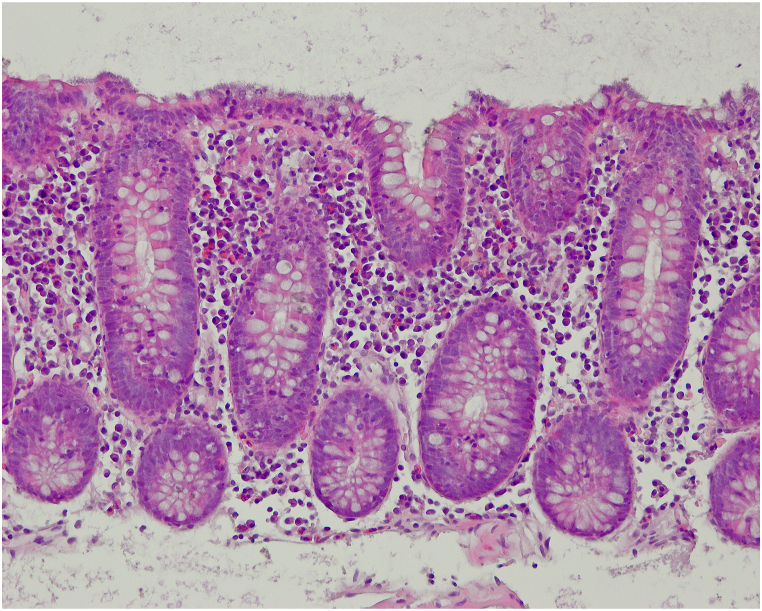 Figure 1
Figure 1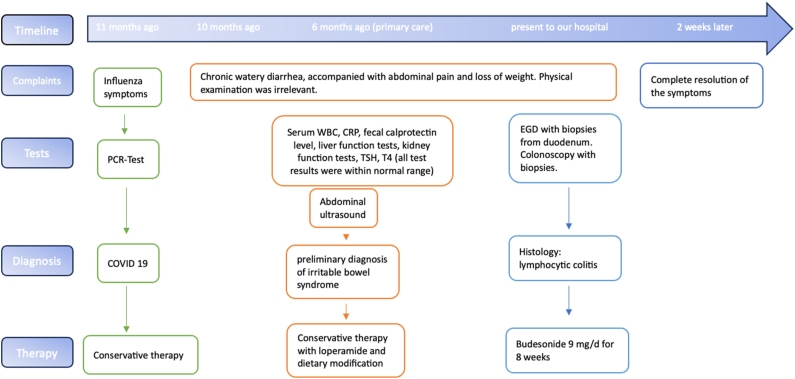 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMicroscopic Colitis · Clostridium difficile and Clostridium perfringens research · Inflammatory Bowel Disease
Introduction
1
Microscopic colitis (MC), a chronic inflammatory condition affecting the colon, is experiencing a rising incidence. Based on biopsy findings, there are two types of microscopic colitis: collagenous and lymphocytic colitis. The incidence of microscopic colitis has increased over time ranges from of 4.9 (95 % CI 4.2–5.7) cases per 100,000 patient-years for collagenous colitis and 5.0 (95 % CI 4.0–6.1) cases per 100,000 patient-years for lymphocytic colitis, with higher prevalence in northern Europe and the northern regions of North America [1]. MC primarily affects older adults around the age of 65, although approximately 25 percent of cases are identified before the age of 45 [2]. While rare in children, there is a female predilection in both collagenous and lymphocytic colitis. The hallmark feature is chronic or intermittent watery non-bloody diarrhea, accompanied by urgency, abdominal discomfort and normal or almost normal mucosal appearance on colonoscopy. There is no particular biomarker available for diagnosing microscopic colitis. Therefore, confirmation currently relies on examining tissue samples obtained through colonoscopy. While infectious agents causing episodes of infectious gastroenteritis may play a role in initiating and/or exacerbating inflammatory bowel disease (IBD), there is limited data linking SARS-CoV-2 infection as a trigger for microscopic colitis [3].
Case presentation
2
A 39-year-old male presented to our department for evaluation and treatment of chronic loose diarrhea, accompanied with recurrent abdominal pain lasting for 10 months. Additionally, he reported a weight loss of 6 kg during this period. His medical history revealed a past SARS-CoV-2 infection 6–8 weeks prior to his current symptoms. However, he did not directly attribute his symptoms to this prior SARS-CoV-2 infection. Furthermore, the patient had received his last dose of the SARS-CoV-2 mRNA vaccine approximately 18 months before his presentation to us. Aside from these occurrences, his medical history and examination revealed no other significant findings. Notably, there were no reports of fever, blood or pus in the stools, medication intake, or family history of inflammatory bowel disease (IBD). The symptoms appeared more pronounced during periods of stress at work. The initial laboratory tests, including blood counts, C-reactive protein, fecal calprotectin level, liver function tests, kidney function tests, stool microscopy and cultures, and thyroid function tests, provided no significant findings. Abdominal ultrasound also showed no abnormalities. Six months prior, the patient sought medical advice from primary care, resulting in a preliminary diagnosis of irritable bowel syndrome. Symptomatic treatment with loperamide and a recommended dietary modification showed no success. We decided to perform an esophagogastroduodenoscopy and colonoscopy to complete the evaluation. Esophagogastroduodenoscopy and biopsies from the stomach and duodenum revealed no abnormalities, providing no evidence for coeliac disease or Whipple's disease. Colonoscopy showed an unremarkable mucosa in the colon and terminal ileum. Mucosal biopsies were taken from the entire colon to rule out microscopic colitis. Histology revealed a moderate but definitely abnormal lymphocytic infiltration of the colonic surface epithelium throughout the entire colonic mucosa (Fig. 1) which otherwise was essentially unremarkable. Importantly, there was not observed any increase of subepithelial collagen. Based on the combination of the clinical presentation of chronic watery diarrhea, normal colonoscopic examination, and typical microscopic findings, a diagnosis of lymphocytic colitis was established. The patient was prescribed an 8-week course of oral budesonide 9 mg once a day for induction of remission. Complete resolution of symptoms was noted after few days, and clinical remission has been maintained so far. The treatment was well tolerated, with no reported adverse or unexpected events. The timeline of the patient's complaints, clinical findings, tests results, diagnosis and interventions applied are summarized in Fig. 2.Fig. 1. Representative microscopic image of the colonic mucosa. Note the intraepithelial lymphocytosis which was seen in all biopsies.Fig. 1. Fig. 2Timeline of the patient's complaints, clinical findings, tests results, diagnosis and interventions. Abbreviations: PCR, Polymerase chain reaction test; COVID 19, Coronavirus disease 2019; WBC, white blood cell; EGD, Esophagogastroduodenoscopy.Fig. 2
Discussion
3
Microscopic colitis symptom severity varies widely, with some individuals experiencing mild, occasional episodes and others struggling with persistent, debilitating symptoms. In severe cases, electrolyte imbalances and dehydration can pose additional health risks. The disease course itself is equally unpredictable, ranging from spontaneous remission to chronic, recurrent manifestations. While some patients find relief without intervention, others require ongoing maintenance therapy to manage their symptoms effectively [4]. Due to the considerable symptom load and significant impact on quality of life, it's crucial to accurately distinguish between patients with microscopic colitis and those with irritable bowel syndrome.
Several factors increase the risk of developing MC. These include advanced age, female sex, smoking and the presence of other autoimmune diseases. Certain medications, such as proton pump inhibitors (PPIs), nonsteroidal anti-inflammatory drugs (NSAIDs) and selective serotonin reuptake inhibitors (SSRIs), may also play a role [5]. The underlying mechanisms of microscopic colitis remain poorly understood, yet it is probable a result of a complex interplay of factors. These include immune system imbalances, epithelial dysfunction, collagen metabolism abnormalities, secretory diarrhea, and gut microbiota alterations, combined with the risk factors mentioned above in genetically predisposed individuals [[6], [7], [8], [9]]. While others have extensively explored this intricate domain, our focus in this case report is directed towards recent insights within the framework of SARS-CoV-2. Infectious agents are believed to induce autoimmunity through mechanisms such as molecular mimicry, bystander activation, polyclonal activation, and epitope spreading [10]. Among these, molecular mimicry is considered the most likely mechanism. This occurs when there is cross-reactivity between epitopes—proteins, carbohydrates, or DNA—shared by the pathogen and the host, leading the immune system to mistakenly attack the body's own tissues [10]. It is speculated that SARS-CoV-2 can disrupt self-tolerance and trigger autoimmune responses through cross-reactivity with host cells, and that the COVID-19 mRNA vaccines might induce a similar response [11]. Reports suggest that the SARS-CoV-2 spike protein can interact with different human tissue antigens [12]. It is also speculated that adverse events following vaccination could be linked to the spike protein present in both the virus and the vaccines [13].
Additionally, other vaccines have been associated with the development of autoimmune diseases, such as narcolepsy, Guillain-Barré syndrome, multiple sclerosis, demyelinating neuropathy, systemic lupus erythematosus, and postural orthostatic tachycardia syndrome [14].
Chey et al. reported a case of lymphocytic colitis after mRNA vaccination and mentioned a Review of the Vaccine Adverse Event Reporting System identifying five cases of mRNA vaccine-associated microscopic colitis following both Pfizer-BioNTech and Moderna vaccinations. Among these cases, three individuals experienced severe diarrhea shortly after their second mRNA vaccine dose, while two others developed diarrhea approximately one month after their second dose [15]. Lee et al. reported a case of lymphocytic colitis that occurred in a healthy middle-aged man after Moderna SARS-CoV-2 mRNA vaccination [16]. Nassar et al. and Moiteiro da Cruz et al. each reported cases of lymphocytic colitis and collagenous colitis, respectively, following SARS-CoV-2 infection [17,18]. In the absence of other identifiable risk factors for microscopic colitis, we hypothesize that the prior SARS-CoV-2 infection in our case may have triggered his current condition by activating the innate immune system.
Clinical relevance
4
This case highlights the significance for healthcare providers to include microscopic colitis in their differential diagnosis when evaluating patients with persistent diarrhea, particularly in the context of recent SARS-CoV-2 infection or vaccination. However, further research is warranted to better understand this association.
Data availability statement
No data was used for the research described in the article.
Additional information
No additional information is available for this paper.
Informed consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given consent for his histological image and other clinical information to be reported in the journal.
Fundings
This research did not receive any funding from agencies in the public, commercial, or not-for-profit sectors.
CRediT authorship contribution statement
A. Alwali: Writing – review & editing, Writing – original draft, Methodology, Data curation, Conceptualization. C. Schafmayer: Validation, Supervision, Data curation. F. Prall: Writing – review & editing, Investigation, Data curation. I. Kamaleddine: Writing – review & editing, Data curation.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nielsen O.H.Fernandez-Banares F.Sato T.Pardi D.S.Microscopic colitis: etiopathology, diagnosis, and rational management Elife 112022 Aug 1e 7939710.7554/e Life.79397 PMID: 35913459; PMCID: PMC 9342949 PMC 934294935913459 · doi ↗ · pubmed ↗
- 2Bonderup O.K.Wigh T.Nielsen G.L.Pedersen L.Fenger-Grøn M.The epidemiology of microscopic colitis: a 10-year pathology-based nationwide Danish cohort study Scand. J. Gastroenterol.5042015 Apr 39339810.3109/00365521.2014.940378 Epub 2015 Feb 3. PMID: 2564562325645623 · doi ↗ · pubmed ↗
- 3García Rodríguez L.A.Ruigómez A.Panés J.Acute gastroenteritis is followed by an increased risk of inflammatory bowel disease Gastroenterology 13062006 May 1588159410.1053/j.gastro.2006.02.004PMID: 1669772216697722 · doi ↗ · pubmed ↗
- 4Nyhlin N.Wickbom A.Montgomery S.M.Tysk C.Bohr J.Long-term prognosis of clinical symptoms and health-related quality of life in microscopic colitis: a case-control study Aliment. Pharmacol. Ther.3992014 May 96397210.1111/apt.12685 Epub 2014 Mar 11. PMID: 2461205124612051 · doi ↗ · pubmed ↗
- 5Masclee G.M.Coloma P.M.Kuipers E.J.Sturkenboom M.C.Increased risk of microscopic colitis with use of proton pump inhibitors and non-steroidal anti-inflammatory drugs Am. J. Gastroenterol.11052015 May 74975910.1038/ajg.2015.119Epub 2015 Apr 28. PMID: 2591622125916221 · doi ↗ · pubmed ↗
- 6Barmeyer C.Erko I.Awad K.Fromm A.Bojarski C.Meissner S.Loddenkemper C.Kerick M.Siegmund B.Fromm M.Schweiger M.R.Schulzke J.D.Epithelial barrier dysfunction in lymphocytic colitis through cytokine-dependent internalization of claudin-5 and -8J. Gastroenterol.52102017 Oct 1090110010.1007/s 00535-017-1309-2Epub 2017 Jan 30. PMID: 2813875528138755 · doi ↗ · pubmed ↗
- 7Escudero-Hernández C.Münch A.Østvik A.E.Granlund A.V.B.Koch S.The water channel Aquaporin 8 is a critical regulator of intestinal fluid homeostasis in collagenous colitis J Crohns Colitis 1472020 Jul 3096297310.1093/ecco-jcc/jjaa 020PMID: 32016376; PMCID: PMC 739318332016376 PMC 7393183 · doi ↗ · pubmed ↗
- 8Khalili H.Axelrad J.E.Roelstraete B.Olén O.D'Amato M.Ludvigsson J.F.Gastrointestinal infection and risk of microscopic colitis: a nationwide case-control study in Sweden Gastroenterology 16052021 Apr 15991607.e 510.1053/j.gastro.2021.01.004Epub 2021 Jan 6. PMID: 33421519; PMCID: PMC 803529733421519 PMC 8035297 · doi ↗ · pubmed ↗