Upper gastrointestinal bleeding from primary aortoesophageal fistula in a patient with aneurism of the thoracoabdominal aorta: Case report and literature review
Elena Curakova Ristovska, Gregor Krstevski, Misel Andov, Aleksandar Kolev, Kristijan Bundovski, Kemal Rusiti, Svetozar Antovic, Ivan Rankovic, Smiljana Bundovska Kocev, Natasa Hadzi‐Nikolova Alcinova, Ante Bogut

TL;DR
A rare case of upper gastrointestinal bleeding caused by a primary aortoesophageal fistula in a patient with a thoracoabdominal aortic aneurysm is reported, highlighting the need for rapid diagnosis and multidisciplinary care.
Contribution
This case report adds to the limited literature on primary aortoesophageal fistulas and emphasizes the importance of clinical awareness for timely intervention.
Findings
A 55-year-old male presented with back pain and upper gastrointestinal bleeding due to a primary aortoesophageal fistula.
Computed tomography confirmed a thoracoabdominal aortic aneurysm with active contrast extravasation.
Despite urgent surgical repair, the patient had a lethal outcome, underscoring the high mortality risk of this condition.
Abstract
Upper gastrointestinal bleeding due to primary aortoesophageal fistula is a rare clinical condition burdened with high mortality rate. However, the outcomes are closely related to the level of clinical awareness, the complementary and multidisciplinary approach during the diagnostic workup, and the selected treatment option. We present an atypical case of an aneurysm of the thoracoabdominal aorta complicated with primary aortoesophageal fistula (AEF). A 55‐year‐old male with no previous diseases, presented with prolonged and intense back pain and upper gastrointestinal bleeding. The gastroscopy detected an unusual culprit lesion in the distal esophagus resembling an esophageal wall defect, and the computed tomography revealed an aneurysm of the thoracoabdominal aorta, remarkable surrounding hematoma, and active contrast extravasation. Despite the urgent surgical repair, a lethal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
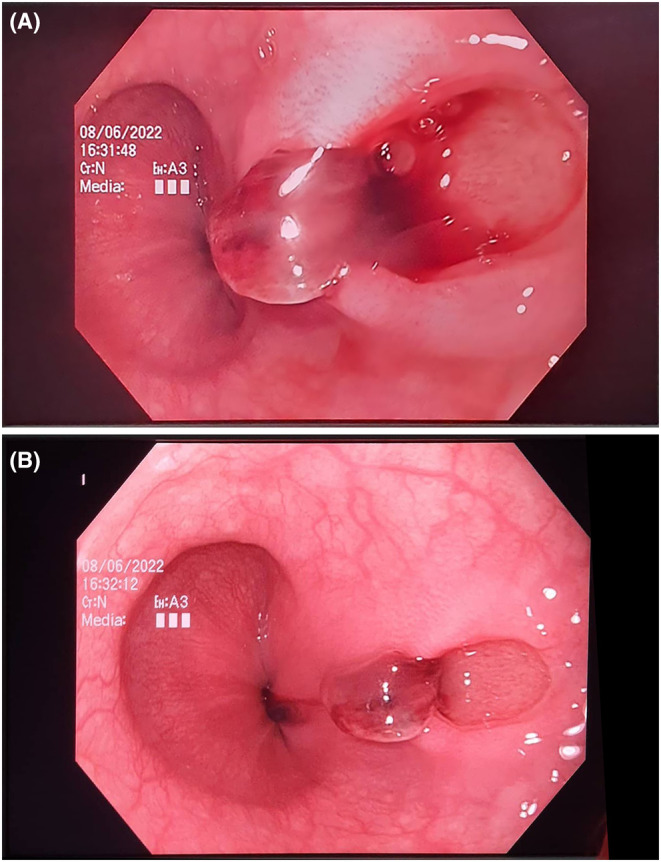 FIGURE 1
FIGURE 1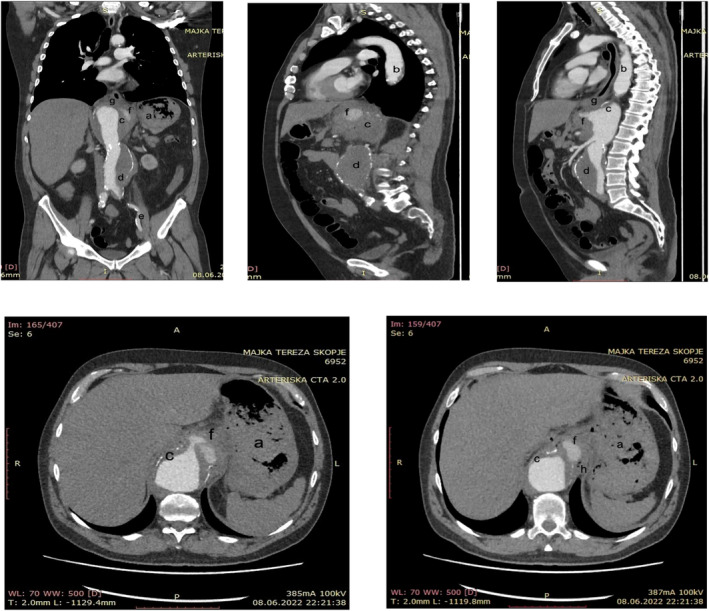 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Aortic and Vascular Conditions · Aortic aneurysm repair treatments · Aortic Disease and Treatment Approaches
INTRODUCTION
1
Aortoesophageal fistula (AEF) is an abnormal communication between the aorta and the esophagus that represents approximately 10% of all the aortoenteric fistulas.1 AEF is a rare, but serious life‐threatening cause of upper gastrointestinal bleeding (UGB) burdened with a high mortality rate.2, 3, 4 Primary AEF occurs in patients with native aorta, while the secondary AEF occurs after surgery of the thoracic aorta or the esophagus. The estimated annual incidence of primary and secondary AEFs is about 0.0015% and 0.6%–2%, respectively.5 The primary AEF is mainly caused by atheromatous aortic aneurysms, or less frequently by penetrating aortic ulcer, tumor, foreign body, radiotherapy, or infection.2, 6, 7 The secondary AEF occurs due to infection of artificial blood vessels after artificial revascularization surgery.8 The entity was reported for the first time in 1818 by Dubrueil, while in 1914, Chiari described the typical clinical triad presented by sentinel bleeding, mid‐thoracic chest pain, and fatal exsanguinating hemorrhage after a variable symptom‐free interval.7 The gastroscopy usually detects the culprit bleeding lesion with unusual aspect, but the definitive diagnosis is made by the dynamic CT showing the aortic aneurysm and abnormal contrast extravasation. UGB due to AEF is burdened with a high morbidity and mortality rate, which raises the need for high clinical awareness and prompt diagnosis and treatment.
CASE HISTORY
2
We present an atypical case of male patient with an aneurysm of the thoracic and abdominal aorta complicated with UGB due to a primary AEF. A 55‐year‐old male patient was referred to our tertiary care gastroenterology center by a surgical emergency department due to hematemesis. A few days ago, the patient was prescribed NSAIDs and corticosteroids for a prolonged and severe back pain. There was no previous cardiovascular or gastrointestinal pathology whatsoever. On admission, he had stable vital signs (blood pressure, 140/90 mmHg; heart rate, 90/min; oxygenation, 98%), the initial blood count was slightly reduced (Hb, 141 g/L; RBC, 4.72 × 10^12^; HCT, 0.41; WBC, 23.3 × 10^9^; PLT, 326 × 10^9^), and BUN (9.2 μmol/L) and creatinine (103 μmol/L) were slightly elevated. After the initial evaluation, the patient was admitted to the Clinic for Gastroenterohepatology.
METHODS (DIFFERENTIAL DIAGNOSIS, INVESTIGATIONS AND TREATMENT)
3
After the admission and primary stabilization, a gastroscopy was performed. The only significant finding during gastroscopy was an unusual regular, oval mucosal lesion in the distal esophagus, 7–8 mm in size, with a small adherent clot, without active bleeding (Figure 1A,B). Afterwards, the patient was intensively monitored, and high‐dose parenteral proton pump inhibitors were administered. During observation, the vitals remained stable, the control blood count performed several hours later was slightly reduced (Hb, 129 g/L; RBC, 4.20 × 10^12^; HCT, 0.35; WBC, 6 × 10^9^; PLT, 347 × 10^9^) and the patient insisted on intense back pain. A dynamic CT of the thorax and abdomen was performed. The CT scan revealed dilated thoracoabdominal aorta through her whole extension. The aneurysmatic dilation of the distal thoracic aorta at the level of the diaphragm was 6.3 cm in size, with irregular flow lumen and presence of mural and eccentric periaortic inflammatory thrombotic masses. The dilation continued towards the abdominal aorta, reaching 4 cm in size at the suprarenal level, 3.5 cm in the infrarenal segment, and propagated towards the common iliac arteries. The thrombotic mass occluded the branching lumen of the celiac trunk, without affecting the branching of the splenic and hepatic artery. At the level of the diaphragm, on the ventrolateral segment of the circumference, an active contrast extravasation in the periaortic area was registered, with periaortic fat stranding, and air inclusions in the mediolateral segment of the extravasation. Inferiorly, in the distal esophagus, above the gastroesophageal junction there was no clear demarcation between the fat tissue and the distal esophagus, indicating a formation of an AEF (Figure 2). After surgical consultation, an urgent open surgery was performed at the University Clinic for Cardiac Surgery. The aortic aneurysm was opened, the thrombotic masses were removed and the esophageal defect was repaired. The aortic reconstruction was performed by using a 22 mm tubular graft, which was proximally anastomosed with the thoracic aorta and distally with the aortic bifurcation. By using 5 and 6 mm Dacron grafts, anastomoses between the tubular graft and the celiac trunk, the superior mesenteric artery and the renal arteries, were made.
(A) Endoscopic aspect of the aortoesophageal fistula: Regular, oval mucosal lesion in distal esophagus, 7–8 mm in size, with a small adherent clot. (B) Endoscopic aspect of the aortoesophageal fistula: regular, oval mucosal lesion in distal esophagus, 7–8 mm in size.
Thoracic and abdominal CT scan presenting the aneurysm of the thoracic and abdominal aorta propagating toward the left common iliac artery, mural thrombosis, and active contrast extravasation with air inclusions in the mediolateral segment of the extravasation. (a) Gastric content, (b) aneurism of the thoracic aorta, (c) suprarenal abdominal aorta, (d) infrarenal abdominal aorta, (e) aneurism propagating to the left common iliac artery, (f) contrast extravasation, (g) distal esophagus, and (h) air bubbles.
CONCLUSION AND RESULTS (OUTCOME AND FOLLOW‐UP)
4
Shortly after the patient was withdrawn from the extracorporeal circulation, a severe hemodynamic instability with persistent hypotension and bradycardia occurred followed by a lethal outcome despite the administration of high‐dose inotropes and vasopressors.
DISCUSSION
5
Although there are several similar cases previously reported, still, there are few unusual and specific aspects of our case that should be discussed in more details. Our patient did not report any previous trauma, cardiovascular, gastrointestinal, or malignant diseases. Also, lacking the typical clinical triad, the natural course was not typical. Although the proportion of AEF that presents with Chiari's triad is not that high,4 still, most patients present with hematemesis, chest pain, and a significant circulatory instability. Our patient was clinically and circulatory stable, he complained of back pain and the bleeding was not particularly massive. Hence, at presentation, there were not many elements that would reasonably rise the clinical suspicion for the presence of this entity.
Regarding the endoscopic appearance of the lesion representing the aortoesophageal communication, there is a large variability in the endoscopic aspect among different reports. Most authors report fresh blood into the gastrointestinal lumen and a lesion described as an ulcer or a mucosal defect with an adherent clot or a fibrin exudate.1, 9, 10, 11 A livid mucosa due to submucosal hematoma or a protruding pulsative luminal mass with narrowing of the esophageal lumen has also been described.6, 12 Interestingly, the initial endoscopy often cannot detect the culprit bleeding lesion, and according to the literature, the AEFs were detected on time only in approximately 25% of the cases.4 Although not diagnostic, the presence of fresh blood, the localization and the endoscopic aspect of the lesion in our patient was indicative of a communication between the digestive tract and a vascular structure. Still, the continuous back pain obliged us to perform additional diagnostic imaging and to seek for a specific and unusual pathology.
The CT scan is the most useful diagnostic tool in the diagnosis of AEF. Although, it does not always clearly identify the actual fistulous tract, the CT scan can demark the aneurysmatic sac, the thrombotic mass, and the mural thickening of the esophageal wall. Most importantly, it can detect the air bubbles in the thrombotic mass, a finding that is pathognomonic for the diagnosis of AEF.1, 2, 7, 12 The performed CT revealed the definitive diagnosis in our patient. However, it is rather unusual that the active contrast extravasation was detected in the abdomen, closely below the diaphragm, while the invasion in the gastrointestinal tract was located in the distal esophagus. That indicates a development of a complex abdominal aneurysm affecting a long aortic segment complicated with an inflammatory thrombotic process invading the esophageal wall.
UGB related to AEF is a potentially fatal condition associated with a high mortality rate that reaches 77% if treated and 100% without intervention.5 The therapeutic approach depends on a patient's current hemodynamic stability and general clinical state. However, successful management of AEF is rare.2 There are two main available treatment options: open surgery and thoracic endovascular aortic repair (TEVAR). Despite treatment, the conventional surgical repair reports in‐hospital mortality rate that approaches 40%.13 TEVAR is an innovative, safe, and less invasive technique associated with lower mortality and morbidity. It is the preferred alternative of open surgery, especially in the emergency setting and in cases with hemodynamic instability.14, 15, 16, 17, 18 However, TEVAR does not definitely repair the esophagus, and there is an increased risk of mediastinitis and infection of the stent‐graft.13 Therefore, TEVAR should only be used as a “bridge” to a definitive surgical intervention,15 except in patients with cancer‐related AEF.2 Alternatively, in order to control the massive bleeding, temporizing measures such as Sengstaken–Blakemore tube placement and radiologic embolization have been occasionally implemented in the past.19, 20, 21 In patients with AEF, initial management with TEVAR followed by an open surgical repair along with appropriate antibiotic use, is associated with a lower mortality rate and better outcomes and is currently the preferred therapeutic approach.15 However, despite the better short‐time survival after endovascular repair, still, both procedures are associated with a similar long‐term mortality.22
In North Macedonia, approximately 10 TEVAR procedures are performed yearly and all of them are planned and performed electively. Considering the small number of performed interventions, the price, and the different available sizes of the stent graft, it is not possible to obtain a stent graft on demand and to perform the TEVAR procedure in an urgent clinical setting. Additionally, considering the remarkable size and morphology of the aneurism that extended up to the common iliac arteries, according to the expert opinion of the vascular surgeon, performing the TEVAR procedure in this particular case would have been challenging. Hence, taking into account the available therapeutic options in our professional environment, open surgical repair was the only available treatment option in our case. However, due to significant hemodynamic instability, shortly after the vascular and digestive repair was performed, a lethal outcome occurred.
Despite the rapid diagnostic process, the accurate diagnosis, and the appropriate hemodynamic support provided by a multidisciplinary approach, unfortunately, in the end, the patient did not survive. We are aware of the fact that case studies presenting rare conditions with an odd presentation as ours, may sometimes be susceptible to publication bias. However, despite the unfavorable outcome, we feel that the benefit of raising awareness for this entity by the publication of the article would overcome the harm of the potential publication bias.
CONCLUSION
6
UGB related to AEF is a rare, but fatal life‐threatening condition in most reported cases. A high index of suspicion and clinical awareness, early recognition, prompt medical intervention, good emergency services, and interdisciplinary collaboration could contribute to early diagnosis and increase the probability for better outcomes.
AUTHOR CONTRIBUTIONS
Elena Curakova Ristovska: Writing – review and editing. Gregor Krstevski: Conceptualization; writing – original draft. Misel Andov: Resources. Aleksandar Kolev: Conceptualization. Kristijan Bundovski: Visualization. Kemal Rusiti: Resources. Svetozar Antovic: Supervision. Ivan Rankovic: Validation. Smiljana Bundovska Kocev: Investigation. Natasa Hadzi‐Nikolova Alcinova: Investigation. Ante Bogut: Visualization.
FUNDING INFORMATION
There was no specific funding for this article.
CONFLICT OF INTEREST STATEMENT
The author declares that there are no conflicts of interest regarding the publication of this paper.
CONSENT
Written inform consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jiao Y , Zong Y , Yu ZL , Yu YZ , Zhang ST . Aortoesophageal fistula: a case misdiagnosed as esophageal polyp. World J Gastroenterol. 2009;15(47):6007‐6009. doi:10.3748/wjg.15.6007 20014468 PMC 2795191 · doi ↗ · pubmed ↗
- 2Zhong XQ , Li GX . Successful management of life‐threatening aortoesophageal fistula: a case report and review of the literature. World J Clin Cases. 2022;10(12):3814‐3821. doi:10.12998/wjcc.v 10.i 12.3814 35647167 PMC 9100730 · doi ↗ · pubmed ↗
- 3Saha BK . Few and far between: a case of aortoesophageal fistula in locally advanced esophageal cancer. Am J Med Sci. 2021;361(1):e 3‐e 4. doi:10.1016/j.amjms.2020.06.010 32631579 · doi ↗ · pubmed ↗
- 4Saers SJ , Scheltinga MR . Primary aortoenteric fistula. Br J Surg. 2005;92(2):143‐152. doi:10.1002/bjs.4928 15685700 · doi ↗ · pubmed ↗
- 5Yang Y , Hu D , Peng D . Primary aortoesophageal fistula: a fatal outcome. Am J Emerg Med. 2018;36(2):343.e 1‐343.e 3. doi:10.1016/j.ajem.2017.11.008 29137907 · doi ↗ · pubmed ↗
- 6Gomes SIM , de Campos FPF , Martines BMR , Martines JADS , Tafner E , Maruta LM . Primary aortoesophageal fistula: a rare cause of acute upper gastrointestinal bleeding. Autops Case Rep. 2011;1(4):57‐63. doi:10.4322/acr.2011.018 31528554 PMC 6735559 · doi ↗ · pubmed ↗
- 7Monteiro AS , Martins R , Martins da Cunha C , Moleiro J , Patrício H . Primary aortoesophageal fistula: is a high level of suspicion enough? Eur J Case Rep Intern Med. 2020;7(8):001666. doi:10.12890/2020_001666 32789135 PMC 7417061 · doi ↗ · pubmed ↗
- 8Kayashima A , Mori H , Okuzawa A , et al. An esophageal ulcer associated with a thoracoabdominal aortic aneurysm. Case Rep Gastroenterol. 2019;13(1):214‐218. doi:10.1159/000500067 31123449 PMC 6514484 · doi ↗ · pubmed ↗