Development of a structured interview for the modified version of the Beth Israel Hospital psychosomatic questionnaire for alexithymia
Gen Komaki, Takanobu Baba, Toshiyuki Yoshida, Tatsuyuki Arimura, Yoshiya Moriguchi, Motonari Maeda

TL;DR
This study developed a reliable and valid structured interview for measuring alexithymia in Japanese young adults.
Contribution
The study introduces a new structured interview (m-SIBIQ) with improved reliability and validity for assessing alexithymia.
Findings
The m-SIBIQ showed high internal consistency (Cronbach’s α.950) and moderate inter-rater reliability (ICC.75).
The factor structure of m-SIBIQ was validated using confirmatory factor analysis.
m-SIBIQ scores were significantly correlated with specific psychological traits like emotional empathy and openness to experience.
Abstract
An observer-rated questionnaire for alexithymia based on the original 17-item Beth Israel Hospital Psychosomatic Questionnaire for Alexithymia (BIQ) was developed by Sifneos in 1973 and modified into a 12-item version of BIQ by Taylor et al. in 1997. However, it has rarely been used in a clinical or research context and studies have not given satisfactory inter-rater reliability for the 12-item version. To develop a structured interview in Japanese for the12-item modified version of BIQ (m-SIBIQ) to determine the reliability and validity of the m- scores and its factor structure model. Ninety-two Japanese young adults were interviewed. The inter-rater reliability of the m-SIBIQ was assessed by exploratory factor analysis. For the concurrent and convergent validities, correlation analysis was done between the scores of m-SIBIQ and the self-reported questionnaires: 20-Item Toronto…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
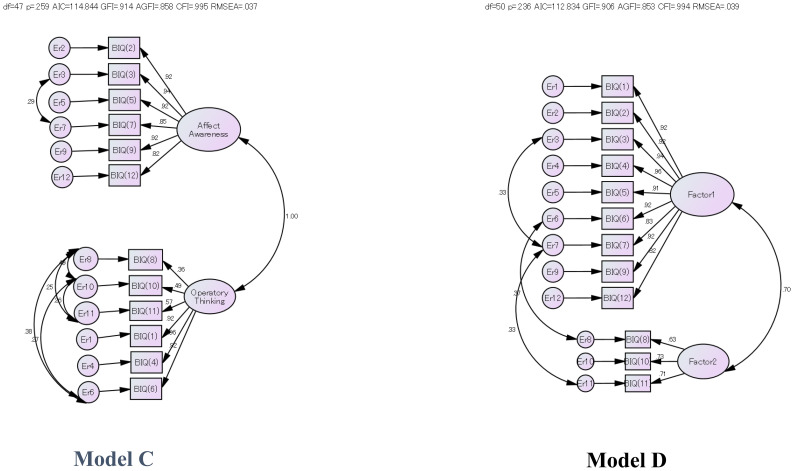 Figure 1
Figure 1| Self-reported Questionnaire | r | p | Self-reported Questionnaire | r | p | ||
|---|---|---|---|---|---|---|---|
|
| Total | 233* | .025 |
| Empathetic Concern | -.194 | .064 |
| DIF | .179 | .088 | Fantasy | -.284** | .006 | ||
| DDF | .181 | .084 | Personal Distress | .050 | .634 | ||
| EOT | .230* | .028 | Perspective Taking | -.118 | .264 | ||
|
| Neuroticism (N) | .122 | .245 |
| Emotional warmth | -.213* | .042 |
| Extraversion (E) | -.305** | .003 | Emotionally chilly | .284** | .006 | ||
| Openness to Experience (O) | -.319** | .002 | Emotional affectedness | -.034 | .745 | ||
| Agreeableness (A) | -.218* | .037 | |||||
| Conscientiousness (C) | -.134 | .204 |
| State anxiety | .246* | .018 | |
|
|
| .072 | .496 | Trait anxiety | .158 | .110 | |
| DIF | DDF | EOT | |
|---|---|---|---|
|
| .915** | .857** | .633** |
|
| .718** | .371** | |
|
| .347** | ||
|
|
| Model | CFA goodness of various factor structure models for m-SIBIQ. | ||||||
|---|---|---|---|---|---|---|---|
| χ2 (d.f.) | X2 | AIC | GFI | AGFI | CFI | RMSEA | |
|
| 104.91(53) | 0 | 154.91 | 0.843 | 0.768 | 0.958 | 0.104 |
|
| 82.92(53) | 0.005 | 132.92 | 0.867 | 0.804 | 0.976 | 0.079 |
|
| 52.844(47) | 0.259 | 114.844 | 0.914 | 0.858 | 0.995 | 0.037 |
|
| 56.834(50) | 0.236 | 112.834 | 0.906 | 0.853 | 0.994 | 0.039 |
| Dependent | Independent variables | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Model | Item | Standardized β | t-score |
| adjusted R2 | F value |
| |||
|
| 1 | Openness (NEO-FFI) | - 0.359 | - 3.785 | 0.001 | ** | 0.092 | |||
| 2 | Emotionally Chilly (EES) | 0.270 | 2.855 | 0.005 | ** | 0.172 | ||||
| 3 | DDF (TAS-20) | 0.195 | 2.041 | 0.044 | * | 0.2 | 8.596 | ** | ||
|
|
| 1 | Extroversion (NEO-FFI) | - 0.321 | - 3.351 | 0.001 | ** | 0.094 | ||
| 2 | EOT (TAS-20) | 0.281 | 2.292 | 0.004 | ** | 0.165 | 9.966 | ** | ||
|
| 1 | Openness (NEO-FFI) | - 0.287 | - 2.901 | 0.005 | ** | 0.114 | |||
| 2 | Emotionally Chilly (EES) | 0.226 | 2.399 | 0.019 | ** | 0.171 | ||||
| 3 | Fantasy (IRI) | - 0.229 | - 2.305 | 0.024 | * | 0.209 | 9.098 | ** | ||
|
|
| 1 | Extroversion (NEO-FFI) | - 0.333 | - 3.482 | 0.001 | ** | 0.102 | ** | |
| 2 | EOT (TAS-20) | 0.268 | 2.796 | 0.006 | ** | 0.166 | 10.04 | |||
|
| 1 | Fantasy (IRI) | - 0.334 | - 3.394 | 0.001 | ** | 0.162 | |||
| 2 | Openness (NEO-FFI) | - 0.247 | - 2.505 | 0.014 | * | 0.209 | 12.99 | ** | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsychosomatic Disorders and Their Treatments · Mental Health and Psychiatry · Complementary and Alternative Medicine Studies
Introduction
“A limited ability in understanding, processing, or describing one’s own feelings is generally referred to as “alexithymia,” and literally means “no words for feelings.” P.E. Sifneos (1) introduced this concept from his observations of psychosomatic patients who had “deficits in identifying, describing, and working with their own feelings as well as difficulty in distinguishing between their feelings and bodily sensations of emotional arousal.” Nemiah, Freyberger, and Sifneos later refined the alexithymia construct to include “a paucity of a fantasy and operative thinking as well as difficulty identifying and describing feelings” (2, 3). More recently, alexithymia has been used with broader populations with common medical and psychiatric disorders (4).
Several self-report measures of alexithymia have been developed, and the twenty-item Toronto Alexithymia Scale (TAS-20), one of the most widely used inventories (5, 6), has been translated into various languages, including Japanese (7–9). It has a three-factor structure: “Difficulty identifying feelings (DIF), difficulty describing feelings to others (DDF), and externally oriented thinking (EOT).” TAS-20 has provided a reliable, valid method for measuring alexithymia in both research and clinical practice. However, TAS-20 has been criticized for not including items of imaginal processes that directly assess the construct describing fantasies in the original TAS-26 (10–12). In addition, there are debates about whether or not a self-report scale like TAS-20 should be used to assess a construct that involves impairments in self-awareness (10–14). TAS-20 scoring may be influenced by negative affectivity (15–17).
When TAS-20 was administered concurrently with the NEO-Five Factor Inventory to a large number of nonclinical subjects (n=2,188), the results identified two subgroups with high TAS-20 scores (18): one with high scores for difficulty identifying feelings (DIF) and neuroticism on NEO-FFI and the other with high scores for externally oriented cognitive style and low openness to experience of NEO-FFI. These results suggest that the total score on the TAS-20 should not be considered a unidimensional measure of alexithymia.
Based on the above findings and others, the main problem with the alexithymia construct has always been its measurement. Because there are currently no uniform methods for evaluating alexithymia in a clinical setting, we translated the twelve-item modified version of the Beth Israel Hospital Psychosomatic Questionnaire (M-BIQ) (19, 20) into Japanese: the original BIQ is the first objective alexithymia scale that was developed by Sifneos (2). M-BIQ is an observer-rated measure with 12 items: nine items of the original BIQ were eliminated and four new items added. Six items assess the ability to identify and verbally communicate feelings (i.e., affect awareness) and six items assess imaginal activity and externally oriented thinking (i.e., operatory thinking, or pensée opératoire). Subsequently, we developed our Structured Interview (SIBIQ) to supplement TAS-20 for use with patients with psychosomatic symptoms (7). Factor analysis of the SIBIQ extracted alexithymia and fantasy ability as significant. We then did a similar investigation of healthy people with no or fewer symptoms, which was necessary to newly develop a modified structure interview format for the Japanese version of the M-BIQ (m-SIBIQ) for a broader population.
An observer-rated interview method, the Toronto Structured Interview for Alexithymia (TSIA), was reported in 2006 by Bagby et al. (21). The alexithymia construct of the TSIA is composed of the three facets of TAS-20 (DIF, DDF and OT) with an additional facet, fantasy and other imaginal processes (IMP). Although the construct validity has been reported to be excellent (22, 23), it needs special training for valid scoring of the 24 items and requires controlling for negative affectivity (23).
Herein, we examine and confirm the reliability and validity of our Japanese version of the m-SIBIQ.
Materials and methods
Participants, interviewers, and procedure
Eligibility
The study targeted university students aged between 19 and 25, all of whom passed the general academic ability test for university entrance. They were majoring in academic courses such as physical and occupational therapy, speech-language pathology, and psychology. None had failed, so academically they were no less linguistically competent than the average person. At the beginning of a lecture to 486 students, we distributed an A4 sheet of paper giving a brief summary of the research: a-cooperation request form containing detailed information about the nature of the government funded-scientific research program to investigate affectivity. After asking them if they would volunteer to take part in our research for a participation reward of 5,000 yen, 220 agreed to participate, with 93 of them taking the interview and completing the self-reported questionnaires at their homes, then returning them at the time of their first interview. They were not scored by the interviewers at that time. One person who did not fill out the BDI-II section of the self-reported questionnaires was excluded from the study, leaving the data of 92 students available for analysis (age range 19-25 years, mean age 20.7 ± 1.1 years: 29 men, mean age 20.6 ± .9 years and 63 women, mean age 20.7 ± 1.2 years). None of the subjects had a major medical, neurological, or psychiatric disorder, including schizophrenia, a depressive disorder, or an anxiety disorder, confirmed by the Mini-International Neuropsychiatric Interview (MINI) (24, 25).
We used three different interviewers/raters, one with a doctoral degree in medicine who specializes in psychosomatic medicine and psychiatry and two with doctoral degrees in psychology who specialize in clinical psychology. They also have master’s degrees in clinical/counseling and considerable training and experience in diagnostic interviewing.
Questions used in the structured interviews
Development of the structured interview for the Japanese version of the modified Beth Israel questionnaire
The interview we developed for the Japanese version of m-SIBIQ is a 12-item structured interview based on the modified Beth Israel Hospital Psychosomatic Questionnaire (M-BIQ) (3, 19, 26) that asks patients with physical or psychiatric symptoms to describe how they perceive their own symptoms. “The 12-item questionnaire of the m-BIQ as originally reported is composed of two subscale scores: (a) Affect Awareness includes six items (items 2, 3, 5, 7, 9 and 12) that pertain to the ability to identify and verbally communicate feelings; and (b) Operatory Thinking, includes six items (items 1, 4, 6, 8, 10 and 11) that pertain to imaginal activity and externally oriented thinking” (3). Because the participants were non-patients with no symptoms, we modified the questionnaire protocol of the SIBIQ (19) by adding questions about feelings in response to negative life events they had experienced: bad, sad, difficult, stressful. If they replied that they had no such life events, we added “if” questions in which they were asked to imagine situations that would generally be expected to cause emotional responses (similar to the Alexithymia-provoked response questionnaire) (27) and asked them to answer in terms of their own emotions. The interviewers rated their answers on the same scale that is used for the m-SIBIQ, with the testers rating their answers according to our interview guidelines.
We request the interviewees to talk freely about their current complaints and symptoms. If they report past symptoms, we ask them to identify the life events that might be associated with their onset and/or exacerbation and ask how they feel about the events. The questions are specific, but if the interviewee does not understand a question, we rephrase it in such a way that they answer in their own words without being influenced by the interviewer; the interviewer adding concrete questions until the necessary information for rating is obtained. Interview guidelines and sample questions are available in the Supplementary Material.
Rating criteria
The explanation of an interviewee’s behavior should not be influenced by the interviewer’s own feeling or affect. Expressions that the interviewer considers to be unnatural: a policy, an official stance, and/or not the interviewee’s real feeling: are rated as inappropriate. The rating scale of the m-SIBIQ is a 7-point Likert type from 1 (strongly disagree) to 7 (strongly agree). Of the 12 items, 3, 7, 8, and 12 are negatively keyed such that scores on these items are appropriately converted before statistical analysis. The total score ranges between 12 and 84 points, with a higher score indicating a person is more alexithymic (2, 19).
Our structured interviews were always done by a pair of interviewers, both of whom have clinical experience with alexithymia. One was always G. K. Briefly, each subject was interviewed for approximately 20 ~ 30 min by one of the two interviewers, as randomly selected, but who in each interview asked the questions while the other watched in the interview room. After the interview, both scored the answers. When the score for a question was assessed differently, they decided on one or the other after discussing their reasons for giving the score.
The 20-item Toronto alexithymia scale
The Japanese translation of the 20-item Toronto Alexithymia scale (TAS-20) was done by Komaki, et al. (7) “TAS-20 is a self-reported questionnaire that consists of 20 items, with three subscales that measure the characteristics of alexithymia. Participants rate each question using a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). A higher score indicates that a person is more alexithymic. The TAS-20 includes three subscales: (a) difficulty in identifying feelings (DIF); (b) difficulty in describing feelings to others (DDF); and (c) externally-oriented thinking (EOT).” The Japanese version of the TAS-20 showed good reliability and validity in a large population (8).
NEO-FFI
“A five factor model of personality traits has been found to account for a large amount of the variance in the data from studies of personality” (28). “The NEO-FFI (NEO-Five Factor Inventory) consists of 60 items and is an abridged version of the NEO-PI-R (the Revised NEO Personality Inventory). It is a widely used self-report instrument designed to provide a general description of normal personality. The NEO-FFI uses a 5-point Likert scale, ranging from 0 (Strongly disagree) to 4 (Strongly agree). The five major domains (factors) of personality are as follows: Neuroticism (N), Extraversion (E), Openness to Experience (O), Agreeableness (A), and Conscientiousness (C). Scores are summed totals and have a range of 0–48 for each of the five personality domains.” The Japanese version of NEO-FFI has been well cross-validated and its reliability has been confirmed (29). High correlations (r = 0.82–0.92) between respective domains of the Japanese version of the NEO-PI-R and the NEO-FFI confirm that the two questionnaires have the same factorial structure.
Emotional empathy scale
The emotional empathy scale (EES) was developed by Mehrabian and Epstein (30) and the Japanese version was done by Kato and Takagi (31). It is a self-administered questionnaire that measures “emotional empathy,” defined as an “affective response to someone else’s emotional experience.” Mehrabian and Epstein (30) created the items of EES with the expectation of multiple subscales, but none were extracted. The Japanese version is subdivided into three components (31) for use with Japanese samples as follows: I) Emotional warmth; a tender and compassionate attitude toward other’s feelings. People with emotional warmth are impressionable in response to art, literature, and movies as well as with other’s sorrow and distress and sometimes participate in voluntary activities. 2) Emotionally chilly: an apathetic and sometimes disfavoring attitude toward other’s feelings like sorrow, distress, and joy. Such people always keep others at a distance. 3) Emotional affectedness; a tendency to be easily influenced by other’s feelings. It is almost the same as “emotional contagion.”
Interpersonal reactivity index
The interpersonal reactivity index (IRI) (32) is “a self-administered questionnaire that measures the empathetic ability of the participant. The Japanese version was developed by Aketa (33). The IRI consists of four scales, each measuring a distinct component of empathy: 1) empathic concern, feeling emotional concern for others: 2) perspective taking, cognitively taking the perspective of another; related to social competence. Factors (I) and (2) are characterized as desirable interpersonal styles: 3) fantasy, emotional identification with characters in books, films, etc.: and 4) personal distress, negative feelings in response to the distress of others.”
The Beck depression inventory-II
“The BDI-II is a 21-item self-report questionnaire used to assess the severity of depression symptoms that is based on the diagnostic criteria for depressive disorders in DSM-IV. Each item is scored from 0 to 3, with a higher score indicating greater intensity of the symptom. The total score is the sum of the items and rages from 0 to 63; a higher score indicates greater depression.” The reliability and validity of the Japanese version of the BDI-II are well documented (34).
State/trait anxiety scales
The Japanese version of the State-Trait Anxiety Inventory (STAI) was used to assess anxiety (35). STAI is a self-reported questionnaire consisting of two scales, with STAI-1 assessing state anxiety and STAI-2 assessing trait anxiety. Each scale consists of 20 items indicating the presence or absence of anxiety symptoms (36). The score of each scale ranges from 20 to 80.
Statistical analysis
Data analyses were performed using IBM SPSS Statistics Ver. 27.0. and Amos Ver. 27.0 The level for statistical significance was set at p < 0.05.
Results
Reliability of the m-SIBIQ
For the sample data sets (n=92), the reliability of the m-SIBIQ was assessed from two perspectives: internal consistency by calculating Cronbach’s α and interrater reliability by calculating the intraclass correlation coefficient (ICC), which is used when there are more than two raters. Cronbach’s α was 0.950 (p<.001), indicating excellent internal consistency and the Intraclass Correlation Coefficient ICC (2,1) was 0.75 (p <.05), indicating good interrater reliability (37).
Exploratory Factor Analysis of the m-SIBIQ
Exploratory factor analysis using the principal factor method with varimax rotation of the samples (n=92) was done to explore the factor structure of the m-SIBIQ. The sample performed adequately on the Kaiser-Meyer-Olkin measure (= 0.91 > minimum acceptable level = 0.50) and on the Bartlett’s test of sphericity (χ2 = 727.9, df = 66, P < 0.0001). Eigenvalues of 1, 2, and 3 number factors to be extracted were as follows: 9.15, 1.34, and 0.58, respectively. When we chose ‘eigenvalue >1’ criteria, the 2-factor solution was optimal with the theoretical constructability, and these two components accounted for 87.5% of the total variance. The two factors extracted, Alexithymia and Fantasy Ability, are different from the factors extracted from the m-BIQ (3). Items 1, 4, and 6, which were originally included in Operatory Thinking, are relegated to Alexithymia and items 8 and 10 are relegated to Fantasy Ability.
Table 1A shows the Pearson correlations of the total m-SIBIQ score for the self-reported questionnaires: TAS-20 Total and three Factors (DIF, DDF, EOT); NEO-FFI five factors; Emotional Empathy Scale (EES); Interpersonal Reactivity Index (IRI); State-Trait Anxiety Inventory (STAI); and BDI-II. Significant, positive correlations were obtained for TAS-20 Total and Factor 3 (EOT), Emotionally Chilly of EES, and State Anxiety, whereas significant, negative correlations were obtained for Extraversion (E), Openness to Experience (O), Agreeableness (A) of NEO-FFI, Fantasy of IRI, and Warmness of EES.
Table 1B shows the Pearson correlations for the TAS-20 total score and its three Factors (DIF, DDF, EOT). All correlations are statistically significant (P < 0.01).
Validity of the m-SIBIQ
Confirmatory factor analysis
The two best candidate models are shown in Figure 1. We tested the goodness-of-fit results (N=92) for the candidates of the m-SIBIQ structure models. Although the sample number is too small to confirm the model structure, we further calculated the covariance as an error based on the exploratory factor analysis as well as the two-factor model of the original version of Sifneos, which allowed us to examine the goodness of fit of several hypothesized models. From among them, the typically good models of the candidates were examined, as described below:
Various factor structure models for m-SIBIQ.
Goodness-of-fit was evaluated by the following criteria as recommended by Cole and Marsh et al. (38, 39); goodness-of-fit (GFI) > 0.85, adjusted goodness-of-fit (AGFI) > 0.80, and root-mean-square residual (RMSR) <0.10. However, the GFI, AGFI, and RMSR are all dependent on sample size and tend to indicate a good fit in a large sample; thus, a good fit might have been obtained as an artifact of sample size, regardless of the real fit, in the present study. We also calculated the comparative fit index (CFI), root mean square error of approximation (RMSEA), and upper and lower end of the 90% confidence interval for the RMSEA to see if the interval includes the area of “close fit” at 0.05. The global fit indices are also supported by a RMSEA > 0.08 (preferably close model fit of < 0.06) and CFI > 0.90 (40).
Model A: Two factor model: the original two factor model by P.E. Sifneos composed of Affective Awareness (BIQ items 2, 3, 5, 7, 9 and 12) and Operatory Thinking (BIQ items 1, 4, 6, 8, 10 and 11). The fit of this model is not sufficiently high, assuming no covariances.
Model B: Two factor model: based on the results of the exploratory factor analysis; Alexithymia (BIQ items 1, 2, 3, 4, 5, 6, 7, 9 and 12) and Fantasy and Dream (BIQ items 8, 10 and 11).
Model C: Two factor confirmatory analysis model (Model A-1); Affect Awareness (BIQ items 2, 3, 5, 7, 9 and 12) and Operatory thinking (BIQ items 1, 4, 6, 8,10 and 11), assuming six covariances.
Model D: Two factor confirmatory analysis model (Model A-2); Alexithymia (BIQ items 1, 2, 3, 4, 5, 6, 7, 9 and 12) and Fantasy/Dream (BIQ items 8, 10 and 11), assuming three covariances (Table 2).
Stepwise multiple regression analysis
Multiple regression analysis was conducted to confirm the extent to which the characteristics of the self-reported questionnaire scales could explain the validity of the structure in each model (Table 3). The dependent variables were the total and two specific sub-class m-SIBIQ scores that were obtained by the Confirmatory Factor Analysis Models, and the independent variables were the scores of the self-reported questionnaires: three factors of TAS-20 (DIF, DDF, and EOT), five major domains of Neo-FFI (Neuroticism, Extraversion, Openness to experience, Agreeableness, and Conscientiousness), Emotional Empathy Scale (EES; Emotional warmth, Emotionally chilly, and Emotional affectedness), Interpersonal Reactivity Index (IRI; Empathic concern, Perspective taking, Fantasy, and Personal distress), BDI-II, and State/Trait Anxiety Scales. For the calculation formula, the TAS-20 total score was excluded beforehand because of its significantly high correlations obtained with the DIF, DDF, and EOT (Table 1B). Finally, the eighteen independent items above were used.
The results showed that the total m-SIBIQ model extracted one negative domain: Openness to Experience in NEO-FFI. No other personality domains were extracted. For other independent self-reported questionnaire items, Emotionally Chilly (EES) and DDF (TAS-20) were positive.
In Model C, the construct component Affective Awareness was negative for Extraversion (NEO-FFI) and positive for EOT (TAS-20), and the other construct component Operatory Thinking was negative for Openness to experience (NEO-FFI), positive for Emotionally Chilly (EES), and negative for Fantasy (IRI).
In Model D, the Factor 1 component “Alexithymia” was negative for Extraversion (NEO-FFI) and positive for EOT (TAS-20). For “Fantasy and Dreams” of Factor 2, both Fantasy (IRI) and Openness to experience (NEO-FFI) were negative.
Discussion
The purposes of the present study were to develop a structured interview for alexithymia and to assess its reliability and validity for use with m-SIBIQ. The reliability, construct, and concurrent and discriminant validity of this m-SIBIQ were evaluated, and it was found to be reliable and valid for the assessment of alexithymia in Japan.
The total m-SIBIQ score model extracted one personality domain, a low score for Openness to Experience (NEO-FFI). Among the other independent items, high Emotionally Chilly (EES) and DDF (TAS-20) scores were extracted. Low Openness to experience and high Emotional Chill represent generally recognized characteristics of alexithymia (3, 41, 42). It is interesting that DDF rather than DIF was extracted as a typical TAS-20 subscale. It is said that the total TAS-scale is generally reliable, yet, the subscale scores can have an added value beyond the total scale score (42). The implication of this is that findings related to TAS DDF make a positive contribution to the m-SIBIQ total score, differently from DIF. TAS DIF was originally defined theoretically to distinguish between feelings and bodily sensations of emotional arousal (1), whereas DDF is related to social context like difficulties in social communication. This finding is consistent with Nemiah’s findings (43) that the alexithymia characteristics difficulties in ‘verbalizing’ and ‘analyzing’ represented by DDF and EOT scores have a significant negative relation with Openness to experience. In addition, Emotionally Chilly (EES) well reflects another characteristic of alexithymia that is related to uncooperative and critical interpersonal behaviors (44).
For construct validity, two best models, C and D, were obtained: Model C is composed of the facets Affective Awareness (AA) and Operative Thinking (OT); Model D is composed of Alexithymia (Factor 1) and Fantasy/dreams (Factor 2).
The facets of Model C are consistent with the construct characteristics of BIQ (42, 45) and confirmed the generally accepted structure model of alexithymia as described by Nemiah and Sifneos (2, 3). This construct model is composed of “Affective Awareness” and “Operative Thinking (la pensée opératoire)” components. For the lower facet of Affective Awareness, it extracts the personality trait Extraversion (NEO-FFI) as negative and the EOT factor of TAS-20 as positive. For the lower facet of the Operative Thinking style (la pensée opératoire), it extracts less Openness to Experience trait (NEO-FFI), a tendency toward Emotionally Chilly (EES), and less Fantasy (IRI) life. These findings are consistent with personality findings observed among people with alexithymic characteristics (42, 45).
In contrast, model D is distinguished by two facets of the alexithymia construct: “Fantasy ability” appears to be another independent factor related to “Alexithymia.” This model reconfirms lack of imagination as a concept of the alexithymia model (2), which was supported and measured in the original TAS but was later eliminated from TAS-20 because the validation of the ‘fantasy’ factor was not successfully established as an independent factor (20). Model D was observed previously in a patient group studied for the development of the SIBIQ (19). The facets fantasy and imaginal processes were poorly mapped on the alexithymia construct (45). The negative relation of the Extraversion personality trait to the alexithymia score is not surprising: an extrovert would have the ability to put feelings into words in the interviews, as when participating in a normal social context.
To summarize the findings above, a paucity of openness to experience as a personality trait significantly affects the formation of the total alexithymia characteristics for m-SIBIQ and strongly affects operatory thinking style and fantasy/dreams, which are characterized in the Alexithymia construct (46). The dimensions of personality traits in reports of recent studies are somewhat different from the present m-SIBIQ findings (12, 42, 45, 46). We completely agree with Rosenberg et. al’s concern that the differences are a limitation of almost all recent studies that examine the relation between alexithymia and the personality traits using self-reports like TAS-20 (47).
For discriminative validity, the depression scores of BDI-II were not correlated with m-SIBIQ in the present study. Many studies have shown that when using a self-reported alexithymia questionnaire like TAS-20, alexithymia appears to be associated with depression and anxiety (15–17, 20, 48). Particularly, the facet “difficulty identifying feelings” is related to negative affectivity, but alexithymia differs from depression. People who score high on the subscales of the above facets may be viewed by others as emotionally aware or they may use emotional language in relatively complex ways. Clearly, people with high negative affect differ substantially from those with alexithymia, who are much less interested in their own psychological and emotional lives. Moreover, this type of structured interview has less of an impact than self-evaluation, probably because when people are depressed they may talk less to others. Thus, one of the important findings of this study is that m-SIBIQ is not influenced by negative affectivity, such as depression.
Some reviews across numerous studies on alexithymia have shown a significant correlation with the neuroticism domain. The findings were from both TAS-20 and TAS-26 (10, 12, 46) which are self-reported questionnaires, thus the correlation of alexithymia with neuroticism may represent a method-specific effect (47). The present study of m-SIBIQ, however, supports evidence that, as Sifneos emphasized at every turn, “what is really needed is for physicians to learn to recognize the difference between neurotic and alexithymic patients” (1).
The present findings show a multi-dimensional view of the personality traits and personality type of persons with alexithymia (12). One reason for the absence of alexithymia in DSM-5 may be because of the failure of taxometric studies to identify alexithymia. As empirical evidence has suggested, alexithymia is related inversely to the psychological mindedness and emotional intelligence traits. Also, alexithymia is better thought of as a coping style that is used to defend against emotional distress associated with specific situations, such as trauma or chronic medical illness (49).
Attachment studies have reported an association between alexithymia and an insecure attachment life style in early childhood (50). Openness to experience may be necessary for the regulation of distressing emotions and doing something to change for the better the problem causing the distress (51). It should be emphasized that being open to one’s own feelings is essential. The relation of alexithymia to health and disease will be better clarified by development of the SIBIQ, and it will help with the investigation of various psychosomatic diseases and reduce the risk of their development.
Some limitations of the present study should be noted. First, our sample consisted of only young adults and there was a statistically small number of subjects. Second, all were well educated students, so more heterogeneous samples are necessary. Future research should include a patient group with high alexithymia scores and analysis of test-retest reliability to confirm these results.
The findings of the present study indicate that m-SBIQ is consistent with the most widely used assessments of the alexithymia construct and that it has great potential as a treatment and research tool for not only psychosomatic patients but also those who are difficult to treat in clinical settings. The characteristics identified represent the personality traits openness to experience, difficulty in describing feelings in self-reported expression, and less fantasy life.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the ethics committee of International university of health and welfare. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
GK: Writing – original draft, Writing – review & editing, Conceptualization. TB: Formal Analysis, Investigation, Methodology, Writing – review & editing. TY: Formal Analysis, Methodology, Writing – review & editing. TA: Conceptualization, Writing – review & editing. YM: Conceptualization, Writing – review & editing. MM: Conceptualization, Supervision, Writing – review & editing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sifneos PE. The prevalence of A’lexithymic’ characteristics in psychosomatic patients. Psychother Psychosom. (1973) 22:255–62. doi: 10.1159/000286529 4770536 · doi ↗ · pubmed ↗
- 2Nemiah JC Sifneos PD. Affect and fantsy in patients with psychosomatic disorders. In: Hill OW, editor. Modern trends in psychosomatic medicine, vol. 2. Butterworths, London (1970). p. 26–34.
- 3Nemiah JC Freyberger H Sifneos PE. Alexityymia: A view of the psychosomatic process. In: Hill OW, editor. Modern trends in psychosomatic medicine, vol. 3. Butterworths, London (1976). p. 430–39.
- 4Taylor GJ Bagby RM. New trends in alexithymia research. Psychother Psychosom. (2004) 73:68–77. doi: 10.1159/000075537 14767148 · doi ↗ · pubmed ↗
- 5Bagby RM Parker JD Taylor GJ. The twenty-item Toronto Alexithymia Scale–I. Item selection and cross-validation of the factor structure. J Psychosom Res. (1994) 38:23–32. doi: 10.1016/0022-3999(94)90005-1 8126686 · doi ↗ · pubmed ↗
- 6Bagby RM Taylor GJ Parker JD. The Twenty-item Toronto Alexithymia Scale-II. Convergent, discriminant, and concurrent validity. J Psychosom Res. (1994) 38:33–40. doi: 10.1016/0022-3999(94)90006-X 8126688 · doi ↗ · pubmed ↗
- 7Komaki G Maeda M Arimura T Nakata A Shinoda H Ogata I. The reliability and factorial validity of the Japanese version of the 20-Item Toronto Alexithymia Scale (TAS-20). Japanese J Psychosomatic Med. (2003) 43:839–46. doi: 10.5926/jjep 1953.56.3_403 · doi ↗
- 8Moriguchi Y Maeda M Igarashi T Ishikawa T Shoji M Kubo C. Age and gender effect on alexithymia in large, Japanese community and clinical samples: a cross-validation study of the Toronto Alexithymia Scale (TAS-20). Biopsychosoc Med. (2007) 1:7. doi: 10.1186/1751-0759-1-7 17371586 PMC 1838425 · doi ↗ · pubmed ↗