Efficacy of Local Anesthesia for Radial Artery Puncture Pain: A Systematic Review and Network Meta-Analysis
Shunsuke Yasuo, Minoru Hayashi, Chiaki Suda, Yuki Kataoka, Shunsuke Taito, Eriya Imai, Kohei Sazanami

TL;DR
This study compares local anesthetics for reducing pain during radial artery punctures, finding mepivacaine and lidocaine most effective.
Contribution
A network meta-analysis comparing multiple local anesthetics for radial artery puncture pain, identifying mepivacaine and lidocaine as most effective.
Findings
Mepivacaine infiltration and lidocaine spray significantly reduce radial artery puncture pain compared to placebo.
No systemic or severe local adverse events were reported in the included studies.
The analysis used a frequentist random-effects model and CINeMA tool for confidence evaluation.
Abstract
We performed a systematic review and network meta-analysis (NMA) to assist clinicians in determining the optimal patient-specific method of analgesia during radial artery puncture by comparing radial artery puncture procedural pain. We included randomized controlled trials that assessed the prophylactic efficacy of local anesthesia for radial artery puncture-associated pain. We searched the Medical Literature Analysis and Retrieval System Online in January 2023, the Cochrane Central Register of Controlled Trials in January 2023, the Excerpta Medica Database in December 2022, the World Health Organization International Clinical Trials Platform Search Portal in January 2023, and ClinicalTrials.gov in January 2023. We synthesized the pain scores (0-100 scale) using the frequentist random-effects NMA model. We evaluated the confidence in each outcome using the CINeMA tool…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
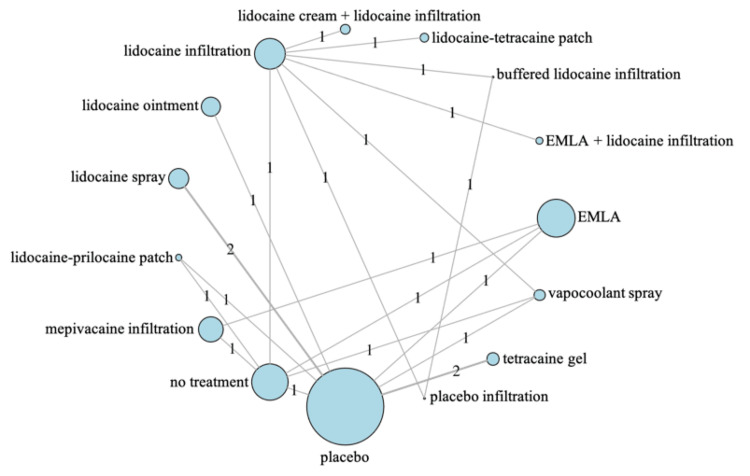 Figure 1
Figure 1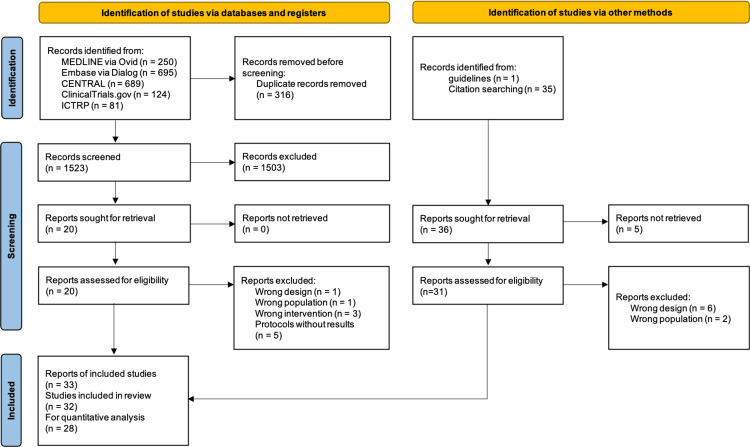 Figure 2
Figure 2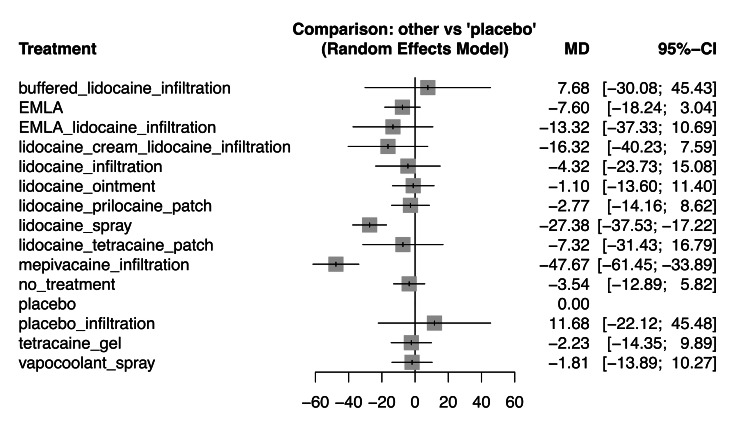 Figure 3
Figure 3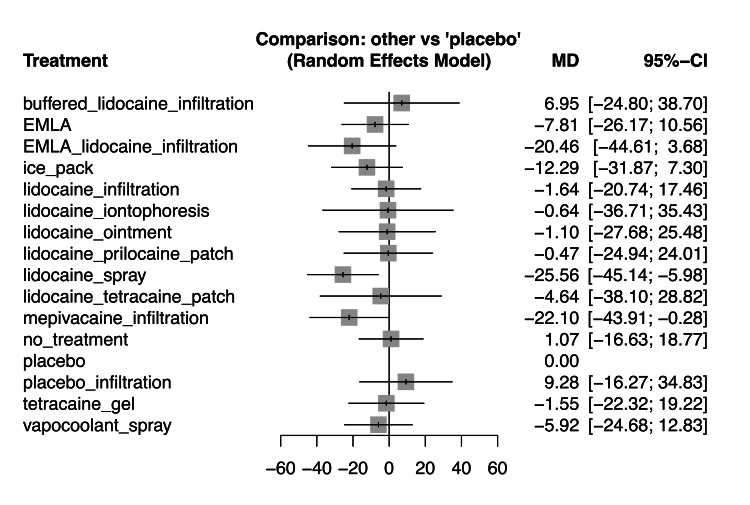 Figure 4
Figure 4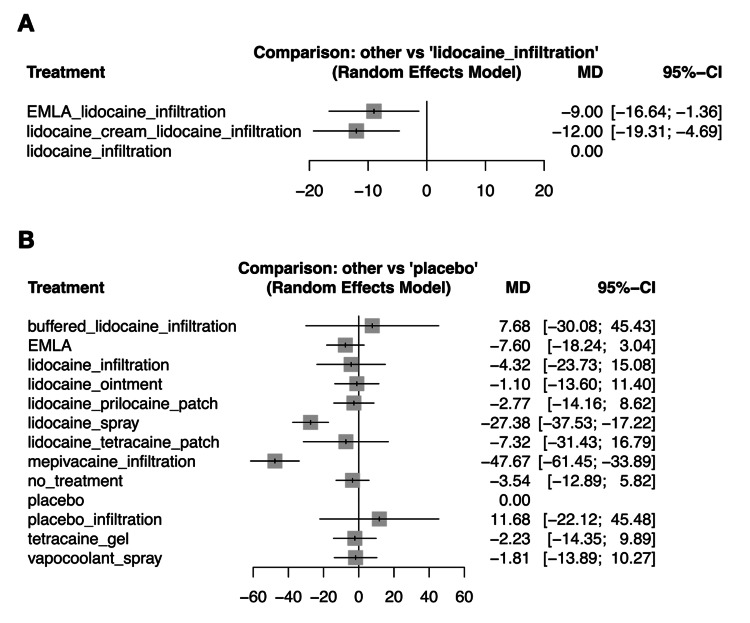 Figure 5
Figure 5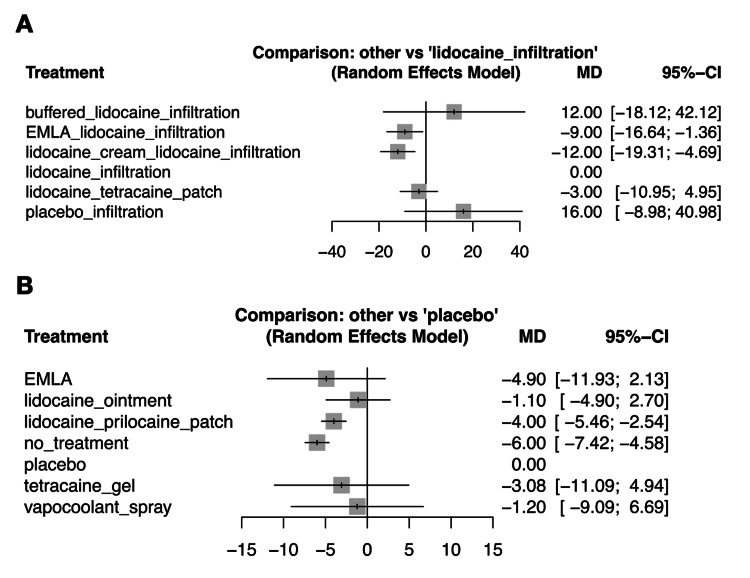 Figure 6
Figure 6| Study name | Intervention/comparison | Setting | Sample size | Age | Male, % | Previous RAP | Co-morbidity | Allen test* | Allergy† | |
| Mean | SD | |||||||||
| Yıldız et al., 2021 [ | Lidocaine spray | The ED | 34 | 60 | 19/84 | 61.76 | 10 | DM 7, HT 4, CHF 11, CKD 4, COPD/BA 8 | Exclude | Exclude |
| Placebo | 33 | 58 median | 24/86 min/max | 66.67 | 13 | DM 10, HT8, CHF 9, CKD 2, COPD/BA 10 | ||||
| Gur and Tekin, 2021 [ | Lidocaine spray | The ED of a tertiary hospital | 72 | 49 | 10 | 61.11 | 37 | Cases with peripheral neuropathy, DM, and methemoglobinemia were excluded | Unknown | Exclude |
| Placebo | 72 | 53 | 11 | 54.17 | 26 | |||||
| Giner et al., 1996 [ | Mepivacaine infiltration | Pulmonary function laboratory | 70 | 61 | 12 | 66.19 | 111 | NR | NR | NR |
| Placebo infiltration | 70 | |||||||||
| No treatment | 70 | |||||||||
| Ruetzler et al., 2012 [ | Lidocaine infiltration | Elective valve replacement or CABG | 45 | 69 | 59/74 | 73.33 | NR | Type of surgery: CABG 18, valve 22, CABG + valve 5 | Exclude | Exclude |
| Lidocaine-tetracaine patch | 45 | 68 median | 54/75 Q1/Q3 | 82.22 | Type of surgery: CABG 17, valve 20, CABG + valve 8 | |||||
| Farahmand et al., 2017 [ | Vapocoolant spray | The ED | 40 | 56.5 | 20/76 | 55 | NR | NR | Exclude | Exclude |
| Placebo | 40 | 48.5 | 19/75 min/max | 47.50 | ||||||
| Pagnucci et al., 2020 [ | Mepivacaine infiltration | The ED of a teaching hospital | 133 | 57 | NR | 63.91 | NR | NR | Unknown | Exclude |
| Ice pack | 134 | 59 | NR | 60.45 | ||||||
| EMLA | 133 | 55 | NR | 54.89 | ||||||
| No treatment | 133 | 57 median | NR | 52.63 | ||||||
| Mahto et al., 2016 [ | Ice pack | Medical ICU of the medical college hospital | 40 | 52.6 | 16 | 71.7 | NR | NR | NR | NR |
| No treatment | 40 | 54.2 | 18 | 65.5 | ||||||
| Olday et al., 2002 [ | Lidocaine infiltration | Elective cardiac surgery | 99 | NR | NR | NR | NR | NR | Exclude | Exclude |
| Tetracaine gel | ||||||||||
| Godoy Mayoral et al., 2010 [ | EMLA | The oxygen therapy office | 23 | 76 | 10.98 | 64.71 | NR | NR | NR | NR |
| Placebo | 28 | |||||||||
| Lightowler and Elliott, 1997 [ | Lidocaine infiltration | The university hospital respiratory unit | 33 | NR | NR | NR | NR | NR | NR | Exclude |
| Placebo infiltration | 34 | |||||||||
| No treatment | 34 | |||||||||
| Hajiseyedjavady et al., 2012 [ | Lidocaine jet injection | The ED | 21 | 52 | 19/85 | 71.43 | NR | NR | NR | Exclude |
| Lidocaine gel | 21 | 60 median | 21/89 min/max | 47.62 | ||||||
| Beaumont et al., 2021 [ | EMLA | Hospitalized in or referred to the pneumology department | 67 | 64 | 12 | 61.19 | 53 | NR | Exclude | Exclude |
| Placebo | 69 | 65 | 12 | 72.46 | 52 | |||||
| Dhami et al., 2020 [ | Vapocoolant spray | Admitted to the pulmonary high-dependency unit of a tertiary care hospital | 30 | 50 | 9 | 80 | 21 | 13 | Exclude | Exclude |
| Ice pack | 30 | 45 | 10 | 83.33 | 21 | 17 details unknown | ||||
| Haynes, 2015 [ | Ice pack | The hospital-based pulmonary function laboratory | 40 | 64.9 | 13.3 | 52.50 | 20 | NR | NR | Exclude |
| No treatment | 40 | 64.4 | 15.3 | 45 | 20 | |||||
| Wade et al., 2015 [ | Lidocaine infiltration | The ED | 20 | 53.2 | 21.5 | 65 | NR | NR | Exclude | NR |
| No treatment | 21 | 54.8 | 20.5 | 57.14 | ||||||
| Khalil, 2017 [ | Ice pack | Medical critical care and emergency units | 50 | 56 | 2.1 | 62 | 10 | NR | Exclude | Exclude |
| No treatment | 50 | 54 | 2.1 | 54 | 11 | |||||
| Youn et al., 2011 [ | EMLA + lidocaine infiltration | Referred for CAG | 38 | 55 | 9 | 60.53 | NR | HT 22, DM 8, DL 5, MI 1, coronary intervention 2 | NR | NR |
| Lidocaine infiltration | 38 | 53 | 8 | 63.16 | HT 17, DM 9, DL 12, MI 2, coronary intervention 6 | |||||
| Tatlı et al., 2018 [ | Lidocaine cream + lidocaine infiltration | Presented to the university hospital with an indication for CAG | 52 | 60.5 | 9.4 | 69.23 | NR | HT 29, DM 23, HL 9, known CAD 12 | NR | Exclude |
| Lidocaine infiltration | 52 | 60.4 | 9.7 | 69.23 | HT 32, DM 16, HL 13, known CAD 13 | |||||
| Bastami et al., 2015 [ | Ice pack | Admitted to a public educational center (the emergency ward) | 31 | 61.25 | 12.61 | 58.06 | 18 | NR | Exclude | Exclude |
| No treatment | 30 | 62.2 | 14.99 | 53.33 | 16 | |||||
| Sherwin et al., 2003 [ | Lidocaine infiltration | Vascular surgery requiring intraarterial pressure monitoring | 15 | 70.7 | 8.5 | 80 | NR | NR | NR | NR |
| Lidocaine iontophoresis | 15 | 73 | 6.6 | 86.67 | ||||||
| Kim et al., 2017 [ | EMLA + lidocaine infiltration | Elective CAG or PCI | 45 | 61 | 9 | 66.67 | NR | SA 17, UA 17, AMI 4 | Exclude | Exclude |
| Lidocaine infiltration | 98 | 60 | 10 | 59.18 | SA 31, UA 33, AMI 8 | |||||
| Matheson et al., 2014 [ | Lidocaine infiltration | Hospitalized | 10 | NR | NR | NR | NR | NR | Exclude | Exclude |
| Buffered lidocaine infiltration | 10 | |||||||||
| Placebo infiltration | 10 | |||||||||
| Latsios et al., 2017 [ | Lidocaine infiltration | Referred with the suspicion of CAD elective CAG | 219 | 64.76 | 10.7 | 74.43 | NR | HT133, DL 107, DM 42 | Exclude | Exclude |
| EMLA | 225 | 65.74 | 11.5 | 72 | HT135, DL 110, DM 54 | |||||
| Aaron et al., 2003 [ | Tetracaine gel | Referred to the pulmonary function laboratory | 24 | 60 | 12 | 66.67 | 7 | BA 3, COPD 5, lung cancer 12, ILD 0 | Unknown | Exclude |
| Placebo | 26 | 61 | 15 | 69.23 | 3 | BA 5, COPD 7, lung cancer 13, ILD 1 | ||||
| Smith et al., 1990 [ | EMLA + lidocaine infiltration | Neurosurgical patients who required arterial cannulation | 10 | 48.3 | 22/69 min/max | NR | NR | NR | NR | NR |
| EMLA | 10 | |||||||||
| Lidocaine infiltration | 10 | |||||||||
| Russell et al., 1988 [ | Lidocaine infiltration | Elective cardiac surgery | 20 | 59 | 9 | 50 | NR | NR | NR | Exclude |
| EMLA | 20 | 62 | 9 | 50 | ||||||
| Tran et al., 2002 [ | Tetracaine gel | The respiratory function laboratory, the respiratory outpatients, the oxygen clinic, and the respiratory ward at a major teaching hospital | 42 | 66.4 | 13.3 | 59.52 | 32 | NR | Exclude | Exclude |
| Placebo | 39 | 64.3 | 15.2 | 66.67 | 29 | |||||
| France et al., 2008 [ | Lidocaine infiltration | Two urban EDs | 20 | 62 | 25/92 | 60 | NR | SOB 2, COPD 11, BA 0, possible PE 4, metabolic 1 | NR | Exclude |
| Vapocoolant spray | 18 | 57 | 29/83 | 55.56 | SOB 3, COPD 4, BA 0, possible PE 8, metabolic 2 | |||||
| No treatment | 21 | 55 | 22/81 min/max | 52.38 | SOB 1, COPD 6, BA 2, possible PE 9, metabolic 2 | |||||
| Rüsch et al., 2017 [ | Lidocaine infiltration | elective cardiac surgery or carotid endarterectomy | 69 | 68 | 8 | 46.38 | NR | NR | Exclude | Exclude |
| Vapocoolant spray | 74 | 67 | 10 | 40.54 | ||||||
| Micu et al., 2006 [ | Lidocaine–prilocaine patch | Lung function laboratory | 34 | 60 | 2 | 67.65 | NR | NR | NR | NR |
| Placebo | 31 | 56 | 3 | 58.06 | ||||||
| No treatment | 38 | 53 | 2 | 76.32 | ||||||
| Cortés-Telles et al., 2012 [ | Lidocaine ointment | Pulmonary function laboratory | 102 | 57 | 18 | 50 | NR | Obstructive diseases (including COPD, BA, and bronchiectasis) 42%, IP 30% | Exclude | Exclude |
| Placebo | 98 | 56 | 18 | 44.9 | ||||||
| Giner et al., 1997 [ | Mepivacaine infiltration | NR | 30 | NR | NR | NR | NR | NR | NR | NR |
| No treatment | 30 | |||||||||
| Study name | Intervention/comparison | Details of intervention | Reason for RAP | Pre-medication | Needle gauge (LA infiltration) | Time from LA to RAP, min* | Healthcare professionals |
| Yıldız et al., 2021 [ | Lidocaine spray | 10%, spraying six times | ABG | NR | 22 | 5 | Emergency medicine residents |
| Placebo | - | - | |||||
| Gur and Tekin, 2021 [ | Lidocaine spray | 10%, spraying six times (each spray contained 0.1 ml) | ABG | NR | 25 | 4 | The same physician in the ED |
| Placebo | - | - | |||||
| Giner et al., 1996 [ | Mepivacaine infiltration | 1%, 0.2 mL | ABG | NR | 22 (27.5) | <1 | NR |
| Placebo infiltration | Saline, 0.2 mL | ||||||
| No treatment | - | ||||||
| Ruetzler et al., 2012 [ | Lidocaine infiltration | 1%, 0.5 mL | A-line | NR | 20 (NR) | 3 | An independent researcher |
| Lidocaine-tetracaine patch | 70 mg each of lidocaine and tetracaine | 20 | |||||
| Farahmand et al., 2017 [ | Vapocoolant spray | 5 seconds | ABG | NR | 23 | <1 | An experienced 2nd year ED resident |
| Placebo | - | - | |||||
| Pagnucci et al., 2020 [ | Mepivacaine infiltration | 1%, 1 mL | ABG | NR | 22 (30) | 10 seconds | An expert nurse, who was also certified in this procedure |
| Ice pack | A plastic bag containing 200 grams of ice | 3 | |||||
| EMLA | 5%, 2 g | 60 | |||||
| No treatment | - | - | |||||
| Mahto et al., 2016 [ | Ice pack | NR | ABG | NR | 23 | 3 | The respiratory therapist |
| No treatment | - | - | |||||
| Olday et al., 2002 [ | Lidocaine infiltration | 2%, 0.5-0.7 mL | A-line | Lorazepam 1-3 mg | 20 (25) | 1 | An experienced registrar or consultant anaesthetist |
| Tetracaine gel | 4% | 60 | |||||
| Godoy Mayoral et al., 2010 [ | EMLA | 1 mL | ABG | NR | 23 G or 0.57 mm in diameter | 30 | The nurses of the laboratory |
| Placebo | - | ||||||
| Lightowler and Elliott, 1997 [ | Lidocaine infiltration | 2%, 0.5 mL | ABG | None | 29 (NR) | 2 | Senior house officers in respiratory medicine |
| Placebo infiltration | Normal saline, 0.5 mL | - | |||||
| No treatment | - | ||||||
| Hajiseyedjavady et al., 2012 [ | Lidocaine jet injection | 2%, 0.2 mL | ABG | NR | 29 | 5 | Experienced postgraduate year–3 ED residents |
| Lidocaine gel | 2%, 1 mL | ||||||
| Beaumont et al., 2021 [ | EMLA | 5%, 2 g | ABG | NR | 23 | 120 | Nurses in the respiratory care unit |
| Placebo | - | - | |||||
| Dhami et al., 2020 [ | Vapocoolant spray | 3 seconds | ABG | NR | 23 | <1 | The primary investigator |
| Ice pack | - | 3 | |||||
| Haynes, 2015 [ | Ice pack | A small plastic bag filled with 12 oz of crushed ice | ABG | NR | 23 | 3 | The principle investigator |
| No treatment | - | - | |||||
| Wade et al., 2015 [ | Lidocaine infiltration | 1%, 1 mL | ABG | NR | 22 or 25 (30) | 10 seconds | The 1st author |
| No treatment | - | - | |||||
| Khalil, 2017 [ | Ice pack | NR | ABG | NR | 25 | 10 | The researcher |
| No treatment | - | - | |||||
| Youn et al., 2011 [ | EMLA + lidocaine infiltration | EMLA: 5%, 2.5 g lidocaine infiltration: 2%, 0.6 mL | CAG | NR | 20 G→5Fr sheath (26) | 60-180 | The operator experienced with TRA in 1,000 or more cases in one year |
| Lidocaine infiltration | NR | ||||||
| Tatlı et al., 2018 [ | Lidocaine cream + lidocaine infiltration | lidocaine cream: 5% lidocaine infiltration: 1%, 1 mL | CAG or PCI | NR | 20 G→5Fr sheath (30) | 30+3 | An experienced cardiologist |
| Lidocaine infiltration | 3 | ||||||
| Bastami et al., 2015 [ | Ice pack | NR | ABG | NR | 25 | 5 | One researcher experienced with the procedure to maintain consistency |
| No treatment | - | - | |||||
| Sherwin et al., 2003 [ | Lidocaine infiltration | 1%, 1 mL | A-line | None | 20 (25) | 1 | An investigator who was blinded to the method of analgesia used |
| Lidocaine iontophoresis | 4%, 4 ml | 10 | |||||
| Kim et al., 2017 [ | EMLA + lidocaine infiltration | 5%, 2.5 g | CAG or PCI | None | 20 G→5-7Fr (24) | 180-240 | Internship medical doctors |
| Lidocaine infiltration | 0.6 mL | NR | |||||
| Matheson et al., 2014 [ | Lidocaine infiltration | 1%, 0.7 ml | ABG | NR | NR (NR) | NR | One researcher who had 12 years of experience as a critical care nurse and routinely draws ABGs on patients in the ICUs |
| Buffered lidocaine infiltration | 1%, 0.7 ml | ||||||
| Placebo infiltration | Bacteriostatic saline, 0.7 ml | ||||||
| Latsios et al., 2017 [ | Lidocaine infiltration | 2%, 1-2 mL | CAG | None (IV sedation) | 20 G→6Fr sheath (26) | 1 | Experienced and radial dedicated interventional cardiologists |
| EMLA | 5%, 2.5 g | 30 | |||||
| Aaron et al., 2003 [ | Tetracaine gel | 4%, 1 g | ABG | None | 23 | 45 | The respiratory therapist |
| Placebo | - | ||||||
| Smith et al., 1990 [ | EMLA + lidocaine infiltration | EMLA: 5% lidocaine infiltration: 1%, 0.2-0.3 mL | A-line | None | 20 (25) | 60+2 | One of the authors |
| EMLA | 60 | ||||||
| Lidocaine infiltration | 2 | ||||||
| Russell et al., 1988 [ | Lidocaine infiltration | 2%, 1-2 mL | A-line | Diazepam 5-10 mg orally | 17.5 (25) | 2 | One of four senior clinicians |
| EMLA | 5%, 2.5 g | 90 | |||||
| Tran et al., 2002 [ | Tetracaine gel | 4% | ABG | NR | 25 | 30 | Respiratory scientists or hospital medical officers experienced with the procedure |
| Placebo | - | - | |||||
| France et al., 2008 [ | Lidocaine infiltration | 2%, 0.5 mL | ABG | NR | 23 (25) | 5 | ED doctors (29 different doctors) |
| Vapocoolant spray | Until the skin becomes "frosted" | <1 | |||||
| No treatment | - | - | |||||
| Rüsch et al., 2017 [ | Lidocaine infiltration | 2%, 0.5 mL | A-line | NR | 20 (27) | <1 | The same physician who was in the fourth year of his anesthesia residency |
| Vapocoolant spray | Approximately 2 to 3 seconds until the skin surface turns white in color | <1 | |||||
| Micu et al., 2006 [ | Lidocaine–prilocaine patch | NR | ABG | NR | 26 | 60 | One of the four nurses |
| Placebo | - | - | |||||
| No treatment | - | - | |||||
| Cortés-Telles et al., 2012 [ | Lidocaine ointment | 5%, 2 g (1 g equals 250 mg of lidocaine) | ABG | NR | 27 | 30 | A respiratory technician |
| Placebo | - | - | |||||
| Giner et al., 1997 [ | Mepivacaine infiltration | NR | ABG | NR | 22 (27.5) | NR | NR |
| No treatment | - | 25 | - |
| Interventions vs. placebo | Within-study bias | Reporting bias | Indirectness | Imprecision | Heterogeneity | Incoherence | CR |
| EMLA | Major concerns | Low risk | No concerns | Some concerns | Some concerns | No concerns | Very low |
| Lidocaine ointment | Some concerns | Low risk | No concerns | No concerns | Major concerns | No concerns | Low |
| Lidocaine spray | Some concerns | Low risk | No concerns | No concerns | No concerns | No concerns | Moderate |
| Lidocaine-prilocaine patch | Some concerns | Low risk | No concerns | No concerns | Major concerns | No concerns | Low |
| No treatment | Some concerns | Low risk | No concerns | No concerns | Major concerns | No concerns | Low |
| Tetracaine gel | Some concerns | Low risk | No concerns | No concerns | Major concerns | No concerns | Low |
| Vapocoolant spray | No concerns | Low risk | Some concerns | No concerns | Major concerns | No concerns | Low |
| EMLA + lidocaine infiltration | Some concerns | Low risk | Some concerns | Some concerns | Some concerns | No concerns | Low |
| Buffered lidocaine infiltration | Some concerns | Low risk | No concerns | Major concerns | No concerns | No concerns | Low |
| Lidocaine-tetracaine patch | Some concerns | Low risk | Some concerns | Major concerns | No concerns | No concerns | Very low |
| Lidocaine cream + lidocaine infiltration | Some concerns | Low risk | No concerns | Some concerns | Some concerns | No concerns | Moderate |
| Lidocaine infiltration | Some concerns | Low risk | Some concerns | Some concerns | Some concerns | No concerns | Low |
| Mepivacaine infiltration | Some concerns | Low risk | Some concerns | No concerns | No concerns | No concerns | Moderate |
| Placebo infiltration | Some concerns | Low risk | No concerns | Major concerns | No concerns | No concerns | Low |
| Rank | Treatment | SUCRA* |
| 1 | Mepivacaine infiltration | 97.68 |
| 2 | Lidocaine spray | 85.31 |
| 3 | Lidocaine cream + lidocaine infiltration | 70.31 |
| 4 | EMLA + lidocaine infiltration | 64.84 |
| 5 | EMLA | 55.83 |
| 6 | Lidocaine-tetracaine patch | 51.76 |
| 7 | Lidocaine infiltration | 44.34 |
| 8 | Lidocaine-prilocaine patch | 42.03 |
| 9 | Tetracaine gel | 40.23 |
| 10 | Vapocoolant spray | 38.68 |
| 11 | Lidocaine ointment | 37.70 |
| 12 | Buffered lidocaine infiltration | 26.02 |
| Study name | Intervention/comparison | Adverse event, % (n) | |
| Yıldız et al., 2021 [ | Lidocaine spray | None | - |
| Placebo | None | - | |
| Gur and Tekin, 2021 [ | Lidocaine spray | None | - |
| Placebo | None | - | |
| Giner, 1996 [ | Mepivacaine infiltration | NR | - |
| Placebo infiltration | NR | - | |
| No treatment | NR | - | |
| Ruetzler et al., 2012 [ | Lidocaine infiltration | Erythema | 4.44 (2) |
| Lidocaine-tetracaine patch | Erythema | 6.67 (3) | |
| Farahmand et al., 2017 [ | Vapocoolant spray | Numbness | Some |
| Placebo | NR | - | |
| Pagnucci et al., 2020 [ | Mepivacaine infiltration | NR | - |
| Ice pack | NR | - | |
| EMLA | NR | - | |
| No treatment | NR | - | |
| Mahto et al., 2016 [ | Ice pack | Not tolerate ice application | 4.76 (2)* |
| No treatment | NR | - | |
| Olday et al., 2002 [ | Lidocaine infiltration | NR | - |
| Tetracaine gel | Erythema | Common | |
| Godoy Mayoral et al., 2010 [ | EMLA | NR | - |
| Placebo | NR | - | |
| Lightowler and Elliott, 1997 [ | Lidocaine infiltration | None | - |
| Placebo infiltration | None | - | |
| No treatment | None | - | |
| Hajiseyedjavady et al., 2012 [ | Lidocaine jet injection | None | - |
| Lidocaine gel | NR | - | |
| Beaumont et al., 2021 [ | EMLA | No significant between-group differences (details unknown) | - |
| Placebo | |||
| Dhami et al., 2020 [ | Vapocoolant spray | Hematoma | 6.67 (2) |
| Ice pack | Hematoma | 33.33 (10) | |
| Haynes, 2015 [ | Ice pack | Not tolerate ice application | 7.5 (3) |
| No treatment | NR | - | |
| Wade et al., 2015 [ | Lidocaine infiltration | None | - |
| No treatment | None | - | |
| Khalil, 2017 [ | Ice pack | NR | - |
| No treatment | NR | - | |
| Youn et al., 2011 [ | EMLA + lidocaine infiltration | NR | - |
| Lidocaine infiltration | NR | - | |
| Tatlı et al., 2018 [ | Lidocaine cream + lidocaine infiltration | Complications (details unknown) | 13.46 (7) |
| Lidocaine infiltration | Complications (details unknown) | 28.85 (15) | |
| Bastami et al., 2015 [ | Ice pack | NR | - |
| No treatment | NR | - | |
| Sherwin et al., 2003 [ | Lidocaine infiltration | NR | - |
| Lidocaine iontophoresis | Slight erythema | NR | |
| Kim et al., 2017 [ | EMLA + lidocaine infiltration | Erythema | 6.6 (3) |
| Lidocaine infiltration | NR | - | |
| Matheson et al., 2014 [ | Lidocaine infiltration | NR | - |
| Buffered lidocaine infiltration | NR | - | |
| Placebo infiltration | NR | - | |
| Latsios et al., 2017 [ | Lidocaine infiltration | None | - |
| EMLA | None | - | |
| Aaron et al., 2003 [ | Tetracaine gel | Redness | 4.17 (1) |
| Swelling | 4.17 (1) | ||
| Itching | 4.17 (1) | ||
| Placebo | Redness | 3.85 (1) | |
| Swelling | 3.85 (1) | ||
| Bruising | 11.54 (3) | ||
| Smith et al., 1990 [ | EMLA + lidocaine infiltration | Mild blanching | 26.67 (8)† |
| Erythema | NR | ||
| EMLA | Mild blanching | NR | |
| Erythema | NR | ||
| Lidocaine infiltration | Mild blanching | 20 (2) | |
| Erythema | NR | ||
| Russell et al., 1988 [ | Lidocaine infiltration | NR | - |
| EMLA | Pallor and slight edema | Common | |
| Tran et al., 2002 [ | Tetracaine gel | Self-limiting itchiness | 2.38 (1) |
| Placebo | Tingling feeling | 2.56 (1) | |
| A local sensation of swelling | 2.56 (1) | ||
| A transient fainting feeling | 2.56 (1) | ||
| France et al., 2008 [ | Lidocaine infiltration | NR | - |
| Vapocoolant spray | NR | - | |
| No treatment | NR | - | |
| Rüsch et al., 2017 [ | Lidocaine infiltration | Local complications (details unknown) | 8.75 (7) |
| Vapocoolant spray | Local complications (details unknown) | 5 (4) | |
| Micu et al., 2006 [ | Lidocaine–prilocaine patch | NR | - |
| Placebo | NR | - | |
| No treatment | NR | - | |
| Cortés-Telles et al., 2012 [ | Lidocaine ointment | None | - |
| Placebo | None | - | |
| Giner et al., 1997 [ | Mepivacaine infiltration | NR | - |
| No treatment | NR | - | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Dental Anxiety and Anesthesia Techniques · Pediatric Pain Management Techniques
Introduction and background
Background
Radial arterial puncture (RAP) is a routine medical procedure frequently employed to obtain arterial blood samples for analysis in patients with impending respiratory failure or metabolic disorders, monitor critically ill patients, and facilitate contrast studies and endovascular therapy in patients with embolism or bleeding. Despite its ubiquity, RAP is associated with intense pain, and numerous studies have been aimed at identifying interventions to reduce discomfort [1]. A prior systematic review (SR) and meta-analysis (MA) highlighted the efficacy of local anesthesia categories such as infiltration anesthesia, cryotherapy, and topical anesthesia [1]. However, these categories vary regarding analgesic efficacy, onset time, and local anesthesia-associated pain for each local anesthesia technique. Recent randomized controlled trials (RCTs) have demonstrated the efficacy of lidocaine spray for topical anesthesia [2,3]. Despite these advancements, there remains a gap in comparative research on the efficacy of each local anesthesia technique to reduce RAP-associated intraprocedural pain.
Goals of this study
To address this gap, this SR and network meta-analysis (NMA) aimed to compare the effect sizes of multiple interventions for RAP-associated intraprocedural pain and provide an updated literature review. NMA is a statistical method that allows for both direct and indirect comparisons, even when treatment pairs have not been directly compared in the same trial [4-6].
Review
Methods
Protocol and Registration
A pre-planned protocol for our SR was registered in the Open Science Framework (https://osf.io/eaxrv/?view_only=557f6c09bccf4f5a8e8230f0b974e54b) [7]. This NMA has been reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses for Network Meta-Analyses (PRISMA-NMA) guidelines [8,9], as shown in Supplemental Material 1 (https://osf.io/eaxrv/?view_only=557f6c09bccf4f5a8e8230f0b974e54b). This SR and NMA were based on published data. As researchers did not access any information that could lead to identifying an individual patient, no ethical issue was raised in this research. Therefore, obtaining ethical approval and consent from participants was waived.
Eligibility Criteria
Type of studies: We included RCTs that assessed the prophylactic efficacy of local anesthesia for RAP-associated pain. We did not apply language or country restrictions. We included all papers, including published and unpublished articles, conference abstracts, and letters. We excluded quasi-randomized trials (such as those allocated by using alternate days of the week). We did not exclude studies based on the observation period or publication year.
Study participants: We included patients of both sexes, 16 years of age or older, before undergoing RAP. We included in RAP any technique that punctures the radial artery, such as arterial blood gas sampling (ABG), cannulation for continuous blood pressure monitoring or blood sampling (A-line), and introducer sheaths for angiography or endovascular treatment. Additionally, we included all local anesthesia methods and comparators. We distinguished between drugs according to the type and route of administration and placebo for local anesthetic infiltration (placebo infiltration) from those for other interventions due to the puncture pain caused by placebo infiltration [10]. For a eutectic mixture of local anesthetic creams of prilocaine and lidocaine (EMLA), if a single study involved multiple interventions based on the time from application to RAP, we chose the intervention closest to three hours [11]. We excluded patients who underwent other procedures, such as puncture of arteries or veins other than the radial artery. Furthermore, we excluded patients who were unable to communicate verbally because of disturbances in consciousness, cognitive impairment, or dysphasia.
Outcomes of Interest
The primary outcome was the pain score during RAP-related procedures, including local anesthesia. We converted the pain scores used in each study, such as the visual analog scale (VAS) and numeric rating scale (NRS), into a 0-100 scale (0: no pain, 100: worst pain), and then integrated them using the mean difference (MD) [12,13]. We classified infiltration anesthesia and cryotherapy as painful local anesthesia [14-17]. We utilized a combined pain score for the entire procedure, which included both local anesthesia and RAP. We employed a higher score in cases where a composite pain score was unavailable, although scores for individual components (pain from local anesthesia and pain from RAP) were present.
The secondary outcomes were the pain scores during RAP alone and all adverse events. If it was not specified whether the pain was due to RAP alone or any RAP-associated pain, we inquired with the author. If the author did not respond, we regarded the pain as due to RAP alone. We used the definition of adverse events set by the original authors and evaluated the incidence proportion of all adverse events during the follow-up period.
Search Strategy
We searched the Medical Literature Analysis and Retrieval System Online, the Cochrane Central Register of Controlled Trials, and the Excerpta Medica Database for studies published after January 1, 2020, as previous research has retrieved studies published through that date [1]. Furthermore, we searched the World Health Organization International Clinical Trials Platform Search Portal (ICTRP) and ClinicalTrials.gov for ongoing or unpublished trials. The details of the search strategy are provided in Supplemental Material 2 (https://osf.io/eaxrv/?view_only=557f6c09bccf4f5a8e8230f0b974e54b). We checked the reference lists of the studies, including international guidelines [18-20] and previous research [1], as well as the reference lists of eligible studies and articles citing eligible studies. We asked the authors of original studies for unpublished or additional data.
Study Selection and Data Extraction
Three independent reviewers (SY, MH, and CS) screened the titles and abstracts, assessed the eligibility based on the full texts, and performed independent data extraction from the included studies using a standardized data collection form. We contacted the original authors if relevant data were missing. Any disagreements were resolved through discussion, and a third reviewer acted as an arbiter (EI) if this failed.
Data Items
We extracted the following study characteristics: (1) methods: study design, author, language, year, country, and setting; (2) participants: number, sex, age, the reason for RAP, previous RAP, comorbidity, and inclusion/exclusion criteria (Allen test, allergy, cold-related reaction, etc.); (3) interventions: local anesthetic technique, needle size for RAP and infiltration, premedication, and healthcare professionals performing the procedure; and (4) outcomes: pain score (assessment tool and target) and adverse event.
Assessment of Risk of Bias
Three reviewers (SY, MH, and CS) independently evaluated the risk of bias (ROB) using the Risk of Bias 2 (The Cochrane Collaboration, London, England, UK) [21]. Disagreements between the two reviewers were discussed; if this failed, a third reviewer (EI) acted as an arbiter, if necessary.
Network Geometry
We demonstrated the network geometry (Figure 1). The numbers above the lines represent the number of RCTs in direct comparisons. The size of the nodes reflects the number of direct comparisons in which the intervention took place.
NMA for pain scores during radial artery puncture-related proceduresThe numbers above the lines represent the number of RCTs in direct comparisons. The size of the nodes reflects the number of direct comparisons in which the intervention took place.EMLA: eutectic mixture of local anesthetic cream of prilocaine and lidocaine, NMA: network meta-analysis, RCTs: randomized controlled trialsImage Credit: Author
Data Synthesis and Statistical Analysis
We pooled the pain scores' MDs and 95% confidence intervals (CIs). We did not perform a quantitative analysis of adverse events because there were no reports of systemic or local severe adverse events, which we were intensely interested in, and few studies described minor local adverse events in detail. All the intervention groups that are relevant to this review were included. For continuous data, we did not impute missing data based on the recommendations of the Cochrane Handbook [22]. We performed a MA of the available data in the original studies. If the original studies did not report pain scores in each group as a combination of the mean and standard deviation, we calculated them based on the method described in the Cochrane Handbook [22]. The validity of these methods was analyzed using sensitivity analysis. We used group-level data. We used the normal likelihood for continuous outcomes. We synthesized the study effect sizes using a random-effects NMA model. We accounted for the correlations induced by multi-group studies by using multivariate distributions. The variance in the random-effects distribution (heterogeneity variance) was used to measure the extent of the across-study and within-comparison variability in treatment effects. To rank the treatments for each outcome, we used the surface under the cumulative ranking curve (SUCRA) [23]. We used MetaInsight for NMA [24].
Subgroup Analysis
To elucidate the influence of effect modifiers on the results, we performed subgroup analyses of the primary outcomes on the reason for RAP: ABG or A-line vs. introducer sheath for coronary angiography (CAG) or percutaneous coronary intervention (PCI).
Sensitivity Analysis
We performed the sensitivity analyses for the primary outcome by excluding studies that used imputation statistics to assess whether the review results were robust to the decisions made during the review process.
Assessment of Reporting Bias
We searched the clinical trial registry system (ClinicalTrials.gov and ICTRP) and performed an extensive literature search for unpublished trials. To assess the outcome reporting bias, we compared the outcomes defined in the trial protocols with those reported in the publications.
Assessment of the Confidence for Each Outcome
Two reviewers (SY and CS) evaluated the confidence for each primary outcome using the CINeMA tool [25,26]. The CINeMA framework includes the following domains: within-study bias, across-study bias, indirectness, imprecision, heterogeneity, and incoherence. For within-study bias and indirectness, CINeMA calculates the contribution of each study in each network estimate and combines these contributions with the study-specific evaluations (low, moderate, or high) to rate the relative effect for each comparison in the network. The domains of imprecision, heterogeneity, and incoherence use a pre-specified clinically important effect size to specify the margin of clinical equivalence between two interventions. Although no study has examined the minimal clinically important difference (MCID) for local anesthesia in RAP pain, based on several studies [27-29], we determined an MCID of 16 for the pain score on a 0-100 scale.
Results
Search Results
A flow diagram of the study selection process is shown in Figure 2. After removing duplicates, we identified 1,523 records from the databases and registers by the January 30, 2023 search, and 36 records were identified from the citation searches and reference checks of the guidelines. We screened the full texts of 51 articles to identify the eligible studies, and we identified 32 eligible studies. We included a total of 28 trials in the qualitative analysis. More details of the excluded reports are provided in Supplemental Material 3 (https://osf.io/eaxrv/?view_only=557f6c09bccf4f5a8e8230f0b974e54b). We excluded four studies from the quantitative analysis because three did not describe the required data (number of participants in each group, mean or median of pain scores, and pain scores on a scale finer than 0-10) [30-32], and one involved interventions that could not be networked with other interventions [33].
PRISMA 2020 flow diagramCENTRAL: Cochrane Central Register of Controlled Trials, Embase: Excerpta Medica Database, ICTRP: World Health Organization International Clinical Trials Platform Search Portal, MEDLINE: Medical Literature Analysis and Retrieval System Online, PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Study Characteristics
The characteristics of the included studies are shown in Tables 1-2. We included 32 studies (n=3,568), in which 16 local anesthesia techniques (lidocaine infiltration, buffered lidocaine infiltration, mepivacaine infiltration, EMLA, tetracaine gel, lidocaine gel, lidocaine ointment, lidocaine jet injection, lidocaine-prilocaine patch, lidocaine-tetracaine patch, lidocaine iontophoresis, lidocaine spray, EMLA + lidocaine infiltration, lidocaine cream + lidocaine infiltration, vapocoolant spray, and ice pack) were performed [2,3,10,14-17,30-54]. The reasons for RAP included ABG in 22 studies [2,3,10,15-17,31-38,41,44,46,49,50,52-54], A-line in six studies [14,30,42,47,48,51], and CAG or PCI in four studies [39,40,43,45]. Only two studies used premedication with sedatives [30,48]. For ABG, A-line, and CAG or PCI (with 5-7 French introducer sheaths), 22-29, 17.5-20, and 18-20 gauge (G) needles, respectively, were used; 24-30 G needles were used for local anesthetic infiltration. The time from local anesthesia to RAP is 0-5 minutes for local anesthetic infiltration, cryotherapy, and lidocaine spray, whereas that for topical anesthesia other than lidocaine spray is longer (20-240 minutes).
Primary Outcome
Pain scores during RAP-related procedures: We conducted an NMA with 1,619 patients from 14 studies on pain scores during RAP-related procedures for 12 interventions (Figure 1) [2,3,14-16,34,39,40,44,46,49,50,52,53]. Supplemental Materials 4, 5, and 6 display each study's results and ROB (https://osf.io/eaxrv/?view_only=557f6c09bccf4f5a8e8230f0b974e54b). A forest plot comparing each intervention with the placebo is shown in Figure 3, and the confidence ratings (CR) for the results are presented in Table 3. Compared with placebo, mepivacaine infiltration and lidocaine spray probably reduce RAP-associated pain (MD: -47.67, 95% CI: -61.45 to -33.89, CR: moderate; MD: -27.38, 95% CI: -37.53 to -17.22, CR: moderate). We present the ranking table and league table details in Table 4 and Supplemental Material 7 (https://osf.io/eaxrv/?view_only=557f6c09bccf4f5a8e8230f0b974e54b), respectively.
Forest plot for all interventions compared with placebo in pain scores during radial artery puncture-related procedureWe conducted an NMA with 1,619 patients from 14 studies on pain scores during radial artery puncture-related procedures for 12 interventions [2,3,14–16,34,39,40,44,46,49,50,52,53].EMLA: eutectic mixture of local anesthetic cream of prilocaine and lidocaine, NMA: network meta-analysis, MD: mean difference, CI: confidence interval
Secondary Outcomes
Pain scores during RAP alone: We conducted an NMA with 3,171 patients from 27 studies on pain scores during RAP alone for 13 interventions [2,3,10,14-17,34-39,41-54]. Supplemental Materials 4, 5, and 6 display each study's results and ROB (https://osf.io/eaxrv/?view_only=557f6c09bccf4f5a8e8230f0b974e54b). A forest plot comparing each intervention with the placebo is shown in Figure 4. Similar trends to the primary outcome were observed, but no intervention significantly reduced pain as compared with the placebo. Among interventions evaluated only as a secondary outcome (ice pack and lidocaine iontophoresis), ice packs may reduce pain (MD: −12.29, 95% CI: −31.87 to 7.30).
Forest plot for all interventions compared with placebo in pain scores during radial artery puncture aloneWe conducted an NMA with 3,171 patients from 27 studies on pain scores during radial artery puncture alone for 13 interventions [2,3,10,14–17,34–39,41–54].EMLA: eutectic mixture of local anesthetic cream of prilocaine and lidocaine, NMA: network meta-analysis, MD: mean difference, CI: confidence interval
Adverse events: Of the 32 studies included, none reported systemic adverse events such as anaphylaxis or local anesthetic systemic toxicity and severe local adverse events [2,3,10,14-17,30-54]. Mild adverse events, such as erythema or hematoma, have been reported and are detailed in Table 5. Many studies excluded patients with allergies to local anesthetics or those with cold-related reactions (e.g., Raynaud’s phenomenon) (Table 1).
Subgroup Analysis
We conducted a subgroup analysis of the RAP-associated pain scores between RAP for CAG or PCI vs. ABG or A-line (Figure 5). In RAP for CAG or PCI, EMLA or lidocaine cream plus lidocaine infiltration may reduce pain associated with RAP compared with lidocaine infiltration alone (MD: −9.00, 95% CI: −16.64 to −1.36, MD: −12.00, 95% CI: −19.31 to −4.69) [39,40].
Forest plot of subgroup analysis in pain scores during radial artery puncture-related proceduresA: Radial artery puncture for CAG or PCI. B: Radial artery puncture for ABG or cannulation for continuous blood pressure monitoring or blood sampling.We conducted a subgroup analysis of the radial artery puncture-associated pain scores between radial artery puncture for CAG or PCI [39,40] vs. ABG or cannulation for continuous blood pressure monitoring or blood sampling [2,3,14–16,34,44,46,49,50,52,53].EMLA: eutectic mixture of local anesthetic cream of prilocaine and lidocaine, ABG: arterial blood gas sampling, CAG: coronary angiography, PCI: percutaneous coronary intervention, MD: mean difference, CI: confidence interval
Sensitivity Analysis
We undertook a sensitivity analysis of RAP-associated pain scores by excluding studies that used imputed statistics (Figure 6) [15,34,39,40,44,46,49,52,53]. However, the results did not significantly differ from the primary outcome results.
Forest plot of sensitivity analysis in pain scores during radial artery puncture-related procedures: exclusion of studies using imputed statisticsA: Interventions forming a network connected by lidocaine infiltration. B: Interventions forming a network connected by placebo.We undertook a sensitivity analysis of radial artery puncture-associated pain scores by excluding studies that used imputed statistics [15,34,39,40,44,46,49,52,53].EMLA: eutectic mixture of local anesthetic cream of prilocaine and lidocaine, MD: mean difference, CI: confidence interval
Discussion
Summary of Results
This SR and NMA included 14 RCTs that compared the efficacy and safety of all interventions on pain scores during RAP-related procedures. Mepivacaine infiltration and lidocaine spray were probably more effective than other local anesthesias. No study reported systemic adverse events such as anaphylaxis, local anesthetic systemic toxicity, or severe local adverse events.
Comparison With the Previous Studies
Our study highlights the efficacy of lidocaine spray, which is a form of topical anesthesia that has not been considered in previous research. The advantage of lidocaine spray is its more rapid effect (within four to five minutes) than other topical anesthetics [55-57]. Physicians can utilize lidocaine spray in situations with time constraints, such as EDs.
Despite using the same route of administration and drugs with similar characteristics [58], our study demonstrated the efficacy of mepivacaine infiltration but not lidocaine infiltration. Although the apparent cause of this phenomenon remains unknown, we can attribute it to several suggested factors.
Firstly, the observed variation may have been influenced by the vasodilatory effects of these drugs. Mepivacaine demonstrated a milder vasodilatory effect than lidocaine [59]. In a SR that compared mepivacaine and lidocaine for local anesthesia in dentistry, mepivacaine with adrenaline was found to be more effective than lidocaine with adrenaline. Conversely, when mepivacaine alone was compared with lidocaine with adrenaline, lidocaine with adrenaline was found to be more effective [60]. This result indicates the potential influence of vasodilatory or vasoconstrictive effects on the analgesic efficacy of mepivacaine and lidocaine. A previous study has suggested that subcutaneous injection-induced pain may intensify in the presence of bleeding [61]. If the milder vasodilatory effect of mepivacaine compared to that of lidocaine contributes to a reduction of RAP-linked bleeding, it may consequently alleviate the associated pain.
Secondly, the observed variation might have been influenced by the size of the needle used for subcutaneous injection. Using thinner needles for subcutaneous injections reduces patient pain scores and minimizes the percentage of patients experiencing pain [61-63]. Moreover, employing smaller needles for subcutaneous injections may not only diminish injection pain but also alleviate the pain from RAP alone because of the potential influence of anxiety about future pain and past pain experiences on subsequent pain scores [64,65]. One study in which mepivacaine was administered used 30 G needles [16]; however, in the five studies in which lidocaine was used, three used 25, 26, and 30 G needles, respectively, and the remaining two did not mention the needle thickness [14,39,40,44,50].
Thirdly, the observed variation may have been influenced by the size of the needle used for the RAP. Earlier reports suggested that using a smaller needle for RAP, irrespective of the presence or absence of prior local anesthesia, is linked to reduced pain [16,66]. Notably, studies using sheath introducers have been included in the RCTs that involved lidocaine infiltration. However, it would be desirable to conduct RCTs by directly comparing mepivacaine and lidocaine to ascertain whether differences in drug characteristics between these drugs influenced the analgesic effects on RAP-procedural pain.
Generalizability
Our results may provide insights that aid in the selection of more suitable local anesthesia methods, depending on the setting. We recommend employing mepivacaine infiltration or lidocaine spray in various settings, including EDs and other urgent situations (approximately five minutes or less). Mepivacaine infiltration may be advantageous in more pressing conditions (approximately one minute or less). Clinicians should take into consideration the pain associated with subcutaneous injections in cases of mepivacaine infiltration. The RCT included in this study used 1 mL of 1% (10 mg/mL) mepivacaine subcutaneously with 30 G needles [16].
If clinicians cannot utilize these options owing to allergies or other reasons, cryotherapy may be considered in time-sensitive settings. In non-urgent situations, such as scheduled blood draws for hospitalized patients or monitoring during planned surgeries, topical anesthesia alone or in combination with infiltration anesthesia is used, using available agents.
Due to the limited number of RCTs that employ sheath introducers for RAP, clinicians should be cautious when extrapolating the current results. The results of our subgroup analysis, which is limited explicitly to RAP for CAG or PCI, suggest that topical and infiltration anesthesia may be more effective than alone. Therefore, although clinicians can use mepivacaine infiltration and lidocaine spray separately, their combination may also be effective. Additional studies are necessary to establish the efficacy of the combination of mepivacaine infiltration and lidocaine spray.
Strengths and Limitations
Strengths: To the best of our knowledge, this is the first NMA to compare any local anesthetic techniques for pain associated with RAP. The primary strength of this NMA lies in its comparison of the efficacy of individual interventions rather than categories. Additionally, we differentiated between the RAP-procedural pain, encompassing local anesthesia, and the pain specifically from RAP alone. Therefore, clinicians can more easily apply the results of this study to their patients than those of the prior SR and MA [1].
Limitations: Nonetheless, this SR and NMA have some limitations. First, we limited the period of our database search to the period after the search period of the previous SR [1]; therefore, we may have missed some essential RCTs before that period. However, we attempted to overcome this limitation by conducting a citation search. Second, utilizing a higher score between the pain scores from local anesthesia and RAP may not replace the composite pain score associated with the entire RAP procedure. Although reports suggest that anxiety about future pain and past pain experiences may affect the perception of subsequent pain, the accurate assessment, overestimation, or underestimation of this influence remains controversial [67-69]. Consequently, the shape of the overall pain score for the procedure based on pain from local anesthesia and pain from RAP remains uncertain.
Conclusions
Mepivacaine infiltration and lidocaine spray probably reduce the pain associated with RAP more than other local anesthesia. No study reported the occurrence of severe adverse events. Even in an emergency setting, such as the ED, clinicians should actively administer these local anesthetics to control pain proficiently. If they use sheath introducers, a combination of topical and infiltration anesthesia may be more effective than infiltration anesthesia alone. We anticipate that researchers will perform RCTs to compare the efficacy of mepivacaine and lidocaine infiltrations and evaluate the combination of lidocaine spray and mepivacaine infiltration against each method, mainly when using sheath introducers.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Interventions to reduce arterial puncture-related pain: a systematic review and meta-analysis Int J Nurs Stud Gonella S Clari M Conti A Simionato L Tassone C Berchialla P Campagna S 10413112620223492222010.1016/j.ijnurstu.2021.104131 · doi ↗ · pubmed ↗
- 2Effectiveness of lidocaine spray on radial arterial puncture pain: a randomized double-blind placebo controlled trial Am J Emerg Med YıldızİU YıldırımÇ Özhasenekler A Şener A GökhanŞ 7247285020213487949310.1016/j.ajem.2021.09.077 · doi ↗ · pubmed ↗
- 310% Lidocaine spray as a local anesthetic in blood gas sampling: a randomized, double-blind, placebo-controlled study Am J Emerg Med Gur A Tekin E 89934920213409833110.1016/j.ajem.2021.05.060 · doi ↗ · pubmed ↗
- 4Simultaneous comparison of multiple treatments: combining direct and indirect evidence BMJ Caldwell DM Ades AE Higgins JP 89790033120051622382610.1136/bmj.331.7521.897PMC 1255806 · doi ↗ · pubmed ↗
- 5A case study of multiple-treatments meta-analysis demonstrates that covariates should be considered J Clin Epidemiol Salanti G Marinho V Higgins JP 8578646220091915777810.1016/j.jclinepi.2008.10.001 · doi ↗ · pubmed ↗
- 6Conceptual and technical challenges in network meta-analysis Ann Intern Med Cipriani A Higgins JP Geddes JR Salanti G 13013715920132385668310.7326/0003-4819-159-2-201307160-00008 · doi ↗ · pubmed ↗
- 7Comparison of the Efficacy of Local Anesthesia for Pain Associated with Radial Artery Puncture: a systematic review and network meta-analysis protocol Yasuo Yasuo S.(2023 January 30 2023 https://osf.io/eaxrv/?view_only=557f 6c 09bccf 4f 5a 8e 8230 f 0b 974e 54b
- 8The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ Page MJ Mc Kenzie JE Bossuyt PM 71372202110.1186/s 13643-021-01626-4PMC 800853933781348 · doi ↗ · pubmed ↗