Endomyocardial involvement in asymptomatic Latin American migrants with eosinophilia related to helminth infection: A pilot study
Abiu Sempere, Fernando Salvador, Laia Milà, Guillem Casas, Xavier Durà-Miralles, Elena Sulleiro, Rosa Vila-Olives, Pau Bosch-Nicolau, Maria Luisa Aznar, Juan Espinosa-Pereiro, Begoña Treviño, Adrián Sánchez-Montalvá, Núria Serre-Delcor, Inés Oliveira-Souto, Diana Pou

TL;DR
This pilot study found early signs of heart changes in Latin American migrants with eosinophilia caused by parasitic infections, suggesting possible cardiac risks.
Contribution
The study is the first to investigate cardiac involvement in Latin American migrants with helminth-related eosinophilia using echocardiography.
Findings
Eosinophilic patients showed greater right ventricle thickness and left atrial area and volume index.
Lower left atrial strain and E-wave deceleration time were observed in patients with eosinophilia.
Thickening of mitral valve leaflets was found in those with eosinophilia, suggesting early diastolic dysfunction.
Abstract
Hypereosinophilic syndrome can produce cardiac involvement and endomyocardial fibrosis, which have a poor prognosis. However, there is limited information regarding cardiac involvement among migrants from Latin America with eosinophilia related to helminthiasis. We conducted a pilot observational study where an echocardiography was performed on migrants from Latin America with both eosinophilia (>450 cells/μL) and a diagnosis of helminth infection, and on migrants from Latin America without eosinophilia or helminth infection. Microbiological techniques included a stool microscopic examination using the Ritchie’s formalin-ether technique, and a specific serology to detect Strongyloides stercoralis antibodies. 37 participants were included, 20 with eosinophilia and 17 without eosinophilia. Twenty (54.1%) were men with a mean age of 41.3 (SD 14.3) years. Helminthic infections diagnosed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
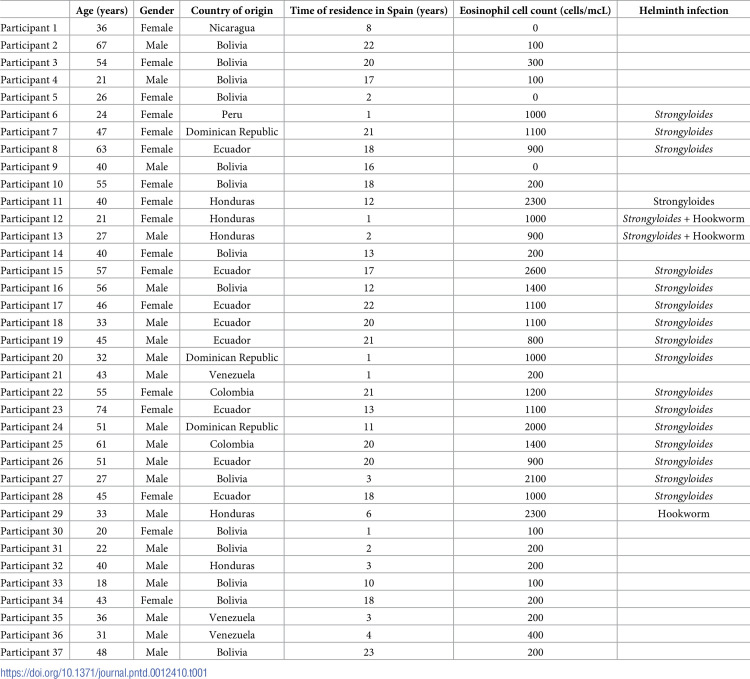 Figure 1
Figure 1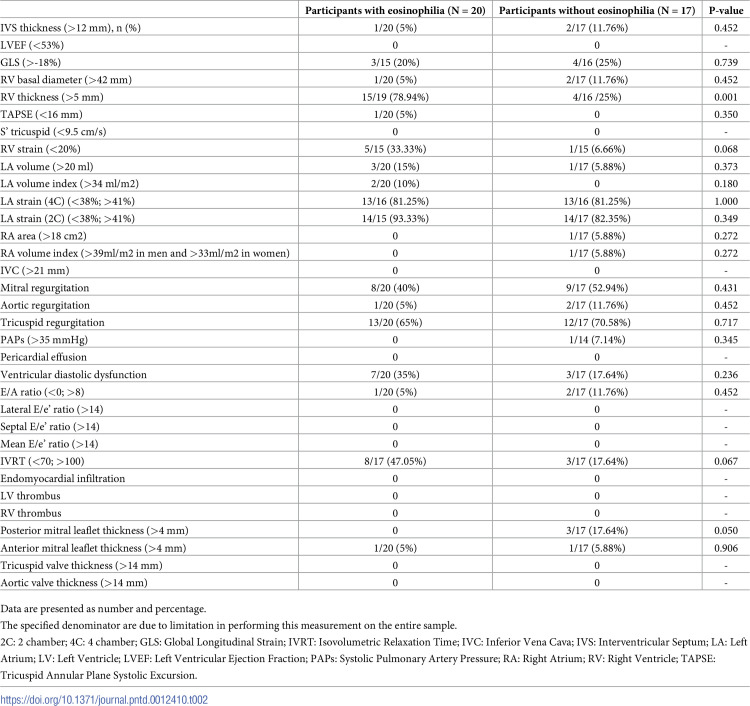 Figure 2
Figure 2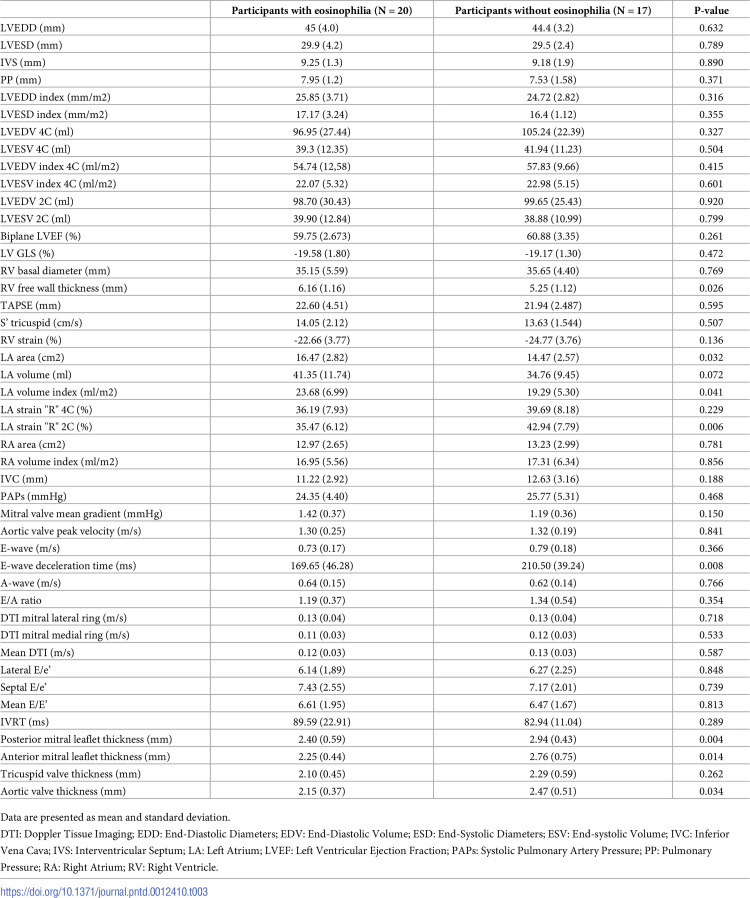 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Disorders and Syndromes · Eosinophilic Esophagitis · Trypanosoma species research and implications
Introduction
Eosinophilia is the expansion of an eosinophilic lineage with an absolute eosinophil count (AEC) > 450 cells/μL that can be developed through three different routes: 1) primary or neoplastic, 2) secondary (helminth, drug or allergen exposure, underlying disease), and 3) idiopathic [1,2]. Hypereosinophilia is considered when AEC is greater than 1500 cells/μL, while hypereosinophilic syndromes (HES) are a group of disorders marked by the sustained overproduction of eosinophils, in which eosinophilic infiltration and mediator release cause damage to multiple organs. HES can produce a wide variety of symptoms ranging from fatigue to life-threatening endomyocardial fibrosis (EMF) and thromboembolic events which are associated with high morbidity and mortality [3,4]. Despite endomyocardial involvement being more frequent in HES of neoplastic origin [5,6], it is also associated with eosinophilia related to helminth infections diagnosed mostly in tropical and subtropical areas in Latin America, Sub-Saharan Africa and Asia, or in migrants to non-endemic countries. Although the exact physiopathology is unknown, It is suggested that proinflammatory mediators, such as eosinophil cationic proteins, may directly damage cardiac cells by affecting plasma membranes and enzyme complexes involved in the mitochondrial process [7,8].
This damage could result in regurgitation, primarily due to thickening of the posterobasal left ventricular walls, and impaired (or absent) posterior mitral leaflet motion. Furthermore, endomyocardial thickness accompanied by thrombus in the left ventricle can lead to obstruction or restriction of blood flow during filling, resulting in a restrictive filling pattern [9,10].
Research indicates that patients in Sub-Saharan Africa with helminth-induced eosinophilia exhibit cardiac alterations similar to those seen in eosinophilia from other causes, despite limited data on cardiac involvement [11,12]. A recent study describes initial findings on cardiac ultrasound in the form of thickening of the posterior leaflet of the mitral valve, but with no clinical manifestations, representing the early stage of the endomyocardial fibrosis process [13].
To the best of our knowledge, no data regarding cardiac alterations have been reported in the tropical and subtropical regions of Latin America on patients with helminth-related eosinophilia. These patients might present with different parasitic infections and carry genetic backgrounds that confer unique susceptibilities to eosinophilia. Hence, this study aims to evaluate the relationship between eosinophilia secondary to helminth infection and cardiac involvement in Latin American patients. Our goal is to enhance understanding of the risk factors and mechanisms underlying cardiac eosinophilia in this population.
Material and methods
Ethics statement
Procedures were performed in accordance with the ethical standards laid down in the Declaration of Helsinki as revised in 2013. The protocol for this study was approved by the Clinical Research Ethics Committee of the Vall d’Hebron University Hospital (PR-AG-357/2018). Written informed consent was obtained from all included patients.
Patients and setting
This is a pilot observational study conducted between September 2019 and October 2021 at the International Health Unit Vall d’Hebron-Drassanes (Barcelona, Spain). Inclusion criteria were adults (> 18 years old) from Latin America, classified in two groups: participants with peripheral eosinophilia (>450 cells/μL) and a diagnosis of helminthiasis, which is considered as the presence of helminth eggs/larvae in the coproparasitological study, or positive serology for Strongyloides stercoralis; and participants without eosinophilia, and absence of helminth infection (negative coproparasitological study and negative serology against S. stercoralis). Exclusion criteria were: previous anthelmintic treatment, ischemic heart disease, known structural heart disease (heart valve disease), diabetes mellitus, arterial hypertension, and Chagas disease. The included individuals underwent a transthoracic echocardiogram by a cardiologist who was blind to the presence or absence of eosinophilia. Demographic, clinical, and microbiological data were collected from electronic medical records, and entered anonymously into a database, specifically created for the study.
Because the International Health Unit Vall d’Hebron-Drassanes is a referral center for tropical diseases, recruited patients were migrants referred from various primary care centers, mostly to screen for imported diseases, or to evaluate laboratory alterations (such as eosinophilia). All patients attended to at the unit fulfilling the inclusion criteria were asked to participate in the study, and were included if they consented.
Microbiological techniques
Stool microscopic examination was performed using the Ritchie’s formalin-ether technique. The serology technique used was the SciMedx Strongyloides serology microwell ELISA (SciMedx Corporation, Denville, NJ, United States). A positive serology was considered as when the optical density index was equal or greater than 2.5 [14].
Echocardiographic study
A two-dimensional transthoracic echocardiographic (TTE) study was performed by a single experienced cardiologist certified by the European Association of Cardiovascular Imaging (EACVI), who was blinded to the patients’ status at the time of image acquisition and analysis. TTE images were acquired using a Vivid S70 (GE Healthcare, Norway), and were analyzed with the GE Echopach software v204 (GE Healthcare, Norway). Acquired TTE images included two-dimensional, M-mode, and Doppler and Tissue Doppler Imaging (TDI) in parasternal longitudinal and short axis, and apical 4, 3, and 2-chamber views, following standard protocols of acquisition. For strain analysis, only images with appropriate quality were used. Among others, the analysis variables were: left ventricular (LV) and right ventricular (RV) dimensions and systolic function (LV ejection fraction (LVEF) and TAPSE/S’, respectively), E/A waves, septal and lateral E’ waves, left atrium (LA) diameter, area, and indexed volume (LAVi), systolic pulmonary artery pressure (PAP), and thickness of valvular leaflets. Left ventricular global longitudinal strain (LV-GLS) was obtained as the average value for the 4, 3 and 2-chamber views. Right ventricle (RV) GLS was measured exclusively in the free wall, and left atrial (LA) GLS assessment was conducted in 4 and 2-chamber analysis, in accordance with previously published methods [15]. Aortic and mitral leaflet thickness were measured at the parasternal long-axis view, while tricuspid valve thickness was measured at the apical 4-chamber view. Specifically, valve thickness was measured at the body of the leaflets. Normal reference values were used to compare groups [16].
Statistical analysis and ethical aspects
Considering the percentage of echocardiographic findings shown in a previous study (48% of the patients in the group with eosinophilia) [13]—a one-sided α value of 5%, a power of 80%, and a maximum of 15% non-evaluable subjects—we estimated the sample size at 22 assessable subjects per group: 22 participants with eosinophilia, and 22 participants without eosinophilia.
Categorical data were presented as absolute numbers and proportions, and continuous variables were expressed as means and standard deviations (when normal distribution is demonstrated using the Kolmogorov-Smirnov test), or as medians and interquartile ranges. The χ^2^ test, or Fisher exact test, when appropriate, was used to compare the distribution of categorical variables, and the Student’s t test or Mann-Whitney U test for continuous variables. Results with a P value of <0.05 were considered statistically significant. SPSS software for Windows (Version 19.0; SPSS Inc, Chicago, IL, USA) was used for statistical analyses.
Results
During the study period, 51 participants were included (25 participants with eosinophilia and 26 without eosinophilia). Fourteen patients (27.4%) failed to attend their appointment for echocardiographic study; hence, 37 participants (20 with eosinophilia, and 17 without eosinophilia) were evaluated for the study. The mean age was 41.3 (SD 14.3) years, and 20 (54.1%) were men. The countries of origin of the participants were as follows: Bolivia (14, 37.8%), Ecuador (8, 21.6%), Honduras (5, 13.5%), Dominican Republic (3, 8.1%), Venezuela (3, 8.1%), Colombia (2, 5.4%), Nicaragua (1, 5.4%) and Peru (1, 5.4%). Median time of residence in Spain was 13 (IQR 3–20) years. Among the participants with eosinophilia, median eosinophil count was 1100 (IQR 1000–1850) cells/mcL, and the helminth infections diagnosed were: 17 cases of S. stercoralis infection, 1 case of hookworm infection, and 2 cases of S. stercoralis and hookworm coinfection. There were no differences regarding sex (50% of men versus 58.8%, p = 0.591) or age (mean age 44.4 years versus 37.6 years, p = 0.157) between thegroups with and without eosinophilia [1]. See Table 1 for demographic and laboratorial information of each participant.
Table 1: Demographic and laboratorial characteristics of the 37 included participants.
All patients had optimal imaging techniques, and all were in sinus rhythm. All qualitative and quantitative measures are compiled in Tables 2 and 3. When comparing the main quantitative echocardiographic findings between the two groups, participants with eosinophilia presented a significantly greater LA area (16.47 cm2 vs 14.47 cm2; p = 0.03), LA volume index (23.68 ml/m2 vs 19.29 ml/m2; p = 0.04), and a decrease in LA strain (35.47% vs 42.94%; p = 0.006) compared to those without eosinophilia. We also observed a greater right ventricle thickness (6.16 mm vs 5.25 mm; p = 0.02), and shorter E-wave deceleration time (169.65 ms vs 210.50 ms; p = 0.008). Of note, a decrease in both anterior and posterior mitral leaflet thickening was observed (p = 0.0014 and p = 0.004, respectively).
Table 2: Qualitative echocardiographic findings.
Table 3: Quantitative echocardiographic findings.
Regarding the main qualitative findings, we observed a trend of a higher proportion of individuals with right ventricular thickness (78.94% vs 25%, p = 0.001), abnormal values of right ventricular free wall strain (33.33% vs 6.66%; p = 0.068), and an impaired isovolumetric relaxation time (IVRT) (47.05% vs 17.64%; p = 0.067) among patients with eosinophilia, although these differences were not statistically significant.
Discussion
Our data revealed an increase in the area and indexed volume of the left atrium, as well as a decrease in the E-wave deceleration time and IVRT in Latin American patients with eosinophilia secondary to helminth infection. All these parameters are associated with the LV diastolic function, probably traducing an early diastolic dysfunction [17]. Interestingly, contrary to previous studies on patients with eosinophilia related to helminth infection which reported an increase in thickness [10–12], our data show a decrease in the thickness of both the anterior and posterior mitral valve leaflets. However, this finding aligns with what has been documented in cases of EMF [18]. Carranza et al. [13] reported an increase in thickness only of the posterior leaflet. However, both the geographical area (sub-Saharan Africa) and the type of helminthiasis (filariasis and/or schistosomiasis) were different from our study (of participants from Latin America mainly infected with S. stercoralis), which might be distinguishing factors.
Of note, left atrial reservoir strain was also decreased in cases compared to controls. Interest in LA strain assessment has been growing in recent years, and guidelines for the standardization of acquisition and analysis are already available [15]. It has become a promising marker of LV diastolic function, with accurate correlations with LV filling pressures and important prognostic implications, particularly in patients with preserved LVEF [19,20]. In this study, the lower LA strain observed in cases may correspond to an early or subclinical diastolic dysfunction. This could hypothetically be an initial stage of a subsequent restrictive filling pattern secondary to the eosinophilic inflammatory response. Additionally, cases presented with a greater RV thickness, which had already been reported in this pathology [18]. It is worth noting that none of the patients presented with symptoms, indicating that all these alterations are early signs of a pathology that might require additional factors to progress, such as genetic and nutritional factors, or geographical region.
EMF is the most common restrictive cardiomyopathy, and an important cause of heart failure in tropical areas of Africa, Latin America, and Southeast Asia. Its overall estimated prevalence could reach 20% of cases in endemic areas of Africa, and it has a poor prognosis [18]. Although its etiology is certainly not known, it is postulated that a combination of factors such as diet, poverty, parasitic infections, genetic predisposition, and ethnicity have been implicated in its pathogenesis [21–23]. Echocardiographic criteria for its diagnosis and assessment were defined by Mocumbi et al. in a rural area of Mozambique [18], and should meet some of the following major criteria: 1) endomyocardial plaques >2 mm in thickness or <1 mm patches affecting more than one ventricular wall; 2) obliteration of the RV or LV apex; 3) thrombi or spontaneous contrast without severe ventricular dysfunction; 4) retraction of the RV apex; 5) atrioventricular (AV)-valve dysfunction due to its adhesion to ventricular wall. Also, the minor criteria are: restrictive flow pattern across AV valves, pulmonary-valve diastolic opening, diffuse thickness of the anterior mitral leaflet, enlarged atrium with normal-size ventricle, M-movement of the interventricular septum, and flat posterior wall and enhanced density of the moderator, or other intraventricular bands.
Helminth infections have been associated with EMF [24], although they may be more strongly associated with filarial infections [25–27] than with Schistosoma spp [28], S. stercoralis [29], and hookworm. However, Carranza-Rodríguez et al. failed to find a correlation between cardiac involvement and any type of parasitic infection among Sub-Saharan migrants, probably due to the low number of patients included in the study [13]. Currently, echocardiographic studies on patients with eosinophilia related to parasitic infection have been primarily conducted in Africa [11–13]. This study marks the first of its kind to be performed on individuals from Latin America. Spain is a country where many migrants from Latin American countries reside, reaching numbers of 2,553,037 people [30]. One of the most frequent helminth infection-causing eosinophilia in this population is S. stercoralis, which is consistent with the findings of our study [31].
Our study has some limitations that should be acknowledged. Firstly, a total of 14 patients were lost to follow-up as they did not attend their scheduled echocardiography appointment, resulting in a reduced sample size. Additionally, the participants may not be fully representative of the general population of Latin America since most of them have been living in Spain for many years, making it likely that some helminth infections have been eliminated from the host after years of leaving the endemic area. Moreover, other nutritional and environmental factors could be involved. Some parameters could not be measured in all participants, due to technical limitations.
In summary, these data suggest that Latin American patients with eosinophilia due to helminthiasis might present incipient echocardiographic alterations suggestive of early diastolic dysfunction, which could be related to eosinophilia-induced changes in the endomyocardium. Future research should consider larger and more diverse samples to confirm our findings and further explore the relationship between eosinophilia and diastolic dysfunction.
Supporting information
S1 ChecklistSTROBE Checklist.(DOC)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Valent P, Klion AD, Horny HP, Roufosse F, Gotlib F, Weller PF et al. Contemporary consensus proposal on criteria and classification of eosinophilic disorders and related syndromes. J Allergy Clin Immunol. 2012;130(3):607–612.e 9. doi: 10.1016/j.jaci.2012.02.019 22460074 PMC 4091810 · doi ↗ · pubmed ↗
- 2Salas-Coronas J, Ramírez-Olivencia G, Pérez-Arellano JL, Belhassen-García M, Carranza-Rodríguez C, García-Rodríguez M et al. Diagnóstico y tratamiento de la eosinofilia importada en viajeros e inmigrantes: recomendaciones de la Sociedad Española de Medicina Tropical y Salud Internacional (SEMTSI) [Diagnosis and treatment of imported eosinophilia in travellers and immigrants: Recommendations of the Spanish Society of Tropical Medicine and International Health (SEMTSI)]. Rev Esp Quimioter. 2017;30(1):62 · pubmed ↗
- 3Weller PF, Bubley GJ. The idiopathic hypereosinophilic syndrome. Blood. 1994 May 15;83(10):2759–79 8180373 · pubmed ↗
- 4Ogbogu PU, Rosing DR, Horne MK 3rd. Cardiovascular manifestations of hypereosinophilic syndromes. Immunol Allergy Clin North Am. 2007;27(3):457–475. doi: 10.1016/j.iac.2007.07.001 17868859 PMC 2048688 · doi ↗ · pubmed ↗
- 5Legrand F, Renneville A, Mac Intyre E, Mastrilli S, Ackermann F, Cayuela JM et al. The Spectrum of FIP 1L 1-PDGFRA-Associated Chronic Eosinophilic Leukemia: New Insights Based on a Survey of 44 Cases. Medicine (Baltimore). 2013;92(5):e 1–e 9. doi: 10.1097/MD.0b 013e 3182 a 71eba 23982058 PMC 4553979 · doi ↗ · pubmed ↗
- 6Bondue A, Carpentier C, Roufosse F. Hypereosinophilic syndrome: considerations for the cardiologist. Heart. 2022;108(3):164–171. doi: 10.1136/heartjnl-2020-317202 34172539 · doi ↗ · pubmed ↗
- 7Moosbauer C, Morgenstern E, Cuvelier SL, Manukyan D, Bidzhekov K, Albrecht S et al. Eosinophils are a major intravascular location for tissue factor storage and exposure. Blood. 2007;109(3):995–1002. doi: 10.1182/blood-2006-02-004945 17003379 · doi ↗ · pubmed ↗
- 8Tai PC, Ackerman SJ, Spry CJ, Dunnette S, Olsen EG, Gleich GJ. Deposits of eosinophil granule proteins in cardiac tissues of patients with eosinophilic endomyocardial disease. Lancet. 1987;1(8534):643–647. doi: 10.1016/s 0140-6736(87)90412-0 2882081 · doi ↗ · pubmed ↗