Transient Urinothorax Following Nephrostomy Tube Placement and Percutaneous Nephrolithotomy: A Case Report
Zhaoqian Zhang, Xiao Li, Mei Yang

TL;DR
A patient developed a rare condition called urinothorax after a kidney procedure but recovered without surgery.
Contribution
This case report highlights a successful conservative management of urinothorax without surgical intervention.
Findings
Urinothorax occurred immediately after nephrostomy tube placement.
The condition resolved within a few days using chest tube and Foley catheter.
Conservative management was sufficient, avoiding the need for surgery.
Abstract
Urinothorax is a rare complication of urological procedures. This report presents a case of a patient who developed urinothorax following nephrostomy tube placement and percutaneous nephrolithotomy (PCNL). The patient was managed conservatively with chest tube and Foley catheter placement, without the need for surgery. Computed tomography (CT) and chest tube output indicated that the urinothorax occurred immediately after nephrostomy tube placement but resolved within a couple of days without further intervention. Unlike some other cases that required surgical intervention due to persistent urine leakage, this case underscores the importance of prompt identification and tailored management of this rare condition based on clinical judgment.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1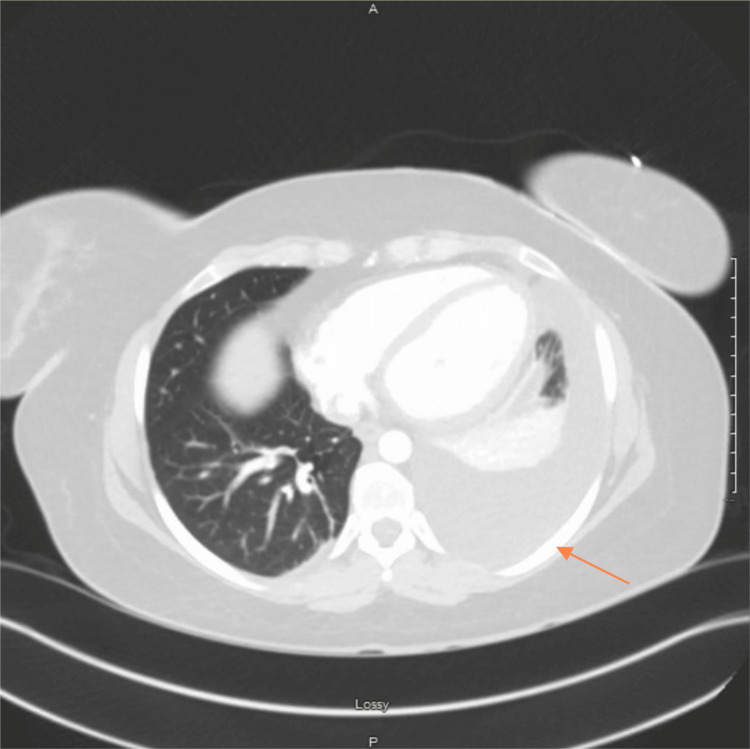 Figure 2
Figure 2 Figure 3
Figure 3| Test | Result | Reference range |
| WBC (K/uL) | 12.2 | 4-11 |
| Neutrophil% | 80% | 40-60 |
| Neutrophil (K/uL) | 9.8 | 1.5-8 |
| Hemoglobin (g/dL) | 12 | 12-18 |
| Platelet (K/uL) | 331 | 130-400 |
| Sodium (mmol/L) | 137 | 135-145 |
| Potassium (mmol/L) | 4 | 3.5-5 |
| Chloride (mmol/L) | 108 | 95-105 |
| Creatinine (mg/dL) | 0.72 | 0.6-1.2 |
| NT-proBNP (pg/mL) | 357 | <125 |
| Pleural fluid analysis | Result | Reference range |
| RBC | 75000 | <100 |
| Glucose (mg/dL) | 49 | Similar to plasma |
| LD (U/L) | 124 | N/A |
| PH | 7.41 | 7.60–7.66 |
| Protein (g/dL) | <2 | <2 |
| Triglyceride (mg/dL) | <10 | <10 |
| Creatinine (mg/dL) | 3.57 | N/A |
| Pleural/serum creatinine ratio | 5.1 | <1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPleural and Pulmonary Diseases · Abdominal Surgery and Complications · Congenital Diaphragmatic Hernia Studies
Introduction
Urinothorax is a rare clinical condition characterized by the presence of urine in the pleural space. This condition usually arises from urinary tract obstructions, trauma, or surgical procedures that permit urine to escape into the retroperitoneal or peritoneal cavity and subsequently reach the pleural space, either directly through diaphragmatic defects or indirectly via lymphatic pathways [1-3]. Accurate diagnosis and timely treatment are vital for patient outcomes, as the clinical presentation can closely resemble other causes of pleural effusions, such as infections, malignancies, or heart failure. Previously reported cases of urinothorax have often been treated with invasive surgical interventions, such as nephrostomy or surgical repair of the urinary tract. In contrast to this, we present a case of transient urinothorax where the patient was managed conservatively with chest tube placement and careful monitoring of pleural fluid drainage [4].
Case presentation
A 34-year-old female with a history of recurrent nephrolithiasis presented to the emergency room (ER) with shortness of breath (SOB) after undergoing nephrostomy tube placement and PCNL.
The patient had a long-standing history of cystinuria and cystine kidney stones, which were well-controlled until her pregnancy when she had to discontinue tiopronin. Her bilateral kidney stones recurred and worsened, causing severe back pain. An ultrasound revealed an echogenic staghorn calculus in the left renal pelvis. She underwent successful nephrostomy tube placement and PCNL, followed by the removal of the nephrostomy tube. A post-procedural CT scan of the abdomen and pelvis revealed a left pleural effusion (Figure 1). On the following day, she developed worsening SOB and was admitted to the ER.
CT abdomen/pelvis without contrastThe right arrow indicates left-sided pleural effusion.
On admission, her labs revealed leukocytosis (Table 1).
A CT angiogram PE protocol and a CT abdomen/pelvis with contrast revealed no acute pulmonary embolus but showed a moderate to large left pleural effusion with compressive atelectasis that was worse than the previous CT. In addition, a posterior defect was identified in the upper pole of the left kidney, corresponding to the percutaneous access site for PCNL. There were no signs of active urine leak on the CT (Figure 2 and Figure 3).
CT angiogram pulmonary embolism (PE) per protocolThe orange arrow indicates worsened left-sided pleural effusion.
CT abdomen/pelvis with contrast.The green arrow indicates a posterior defect in the left kidney
Following consultation with urology and pulmonology, a chest tube and Foley catheter were placed. Pleural fluid analysis revealed elevated red blood cells, likely resulting from trauma during the PCNL procedure, along with a creatinine level of 3.57 and a pleural/serum creatinine ratio of 5.1, which is diagnostic for urinothorax (Table 2).
Due to the absence of active urine leakage into the pleural cavity, the patient was managed conservatively with chest tube placement and Foley catheter placement. The chest tube output was 1.6 L on the first day, 0.7 L on the second day, and 0.1 L on the third day. As the patient’s symptoms improved significantly, the chest tube was removed on the fourth day without complications. Cytological analysis of the pleural fluid showed reactive mesothelial cells with acute and chronic inflammation, no malignancy or infection. The patient was discharged without issues. During a three-month follow-up, the patient's kidney stones were found to be predominantly cystine, and she experienced a bilateral recurrence of kidney stones.
Discussion
Urinothorax, the presence of urine in the pleural space, is an unusual condition [1-5]. The common causes include obstructive uropathy with hydronephrosis and diaphragmatic disruption due to blunt abdominal trauma. Other causes include percutaneous endoscopic renal procedures, retroperitoneal inflammatory processes, polycystic kidney disease, ureteral valves, extracorporeal lithotripsy, and intra-abdominal compression from a gravid uterus or lymphomatous masses [6-8]. The proposed mechanisms for urinothorax include direct extraperitoneal urine collection into the pleural space or lymphatic drainage of urine [8-10]. In this case, urinothorax likely developed from urine extravasation during and after the procedure, evidenced by the pinkish appearance of the urine and pleural fluid, and the high RBC levels in pleural analysis.
Diagnosis of urinothorax is confirmed via thoracentesis, revealing fluid with a urine-like odor and transudative nature with a pH lower than 7.30. A pleural fluid-to-serum creatinine ratio greater than 1 is diagnostic of urinothorax [11-14]. Other diagnostic tests may include renal scans, pyelograms, and contrast-enhanced CT scans to locate urinary system defects. Renal ultrasound and CT abdomen can show hydroureteronephrosis, and contrast-enhanced CT can reveal a reno-pleural fistula. Technetium-99m renal scintigraphy can demonstrate the translocation of 99Tc-labeled albumin from the genitourinary tract into the pleural space [11-18].
In this case, the pleural/serum creatinine ratio of 5.1 confirmed the diagnosis of urinothorax. The contrast-enhanced CT abdomen/pelvis showed no reno-pleural fistula, suggesting that the urine leak occurred shortly after nephrostomy tube removal. The chest tube outputs (1.6 L on the first day, 0.7 L on the second day, and 0.1 L on the third day) indicated a cessation of urine leakage within one to two days. Current management of urinothorax as cited in the literature often includes invasive surgical interventions, such as nephrostomy or surgical repair, to address the underlying cause and prevent recurrence. By contrast, our case highlights a successful conservative approach, utilizing chest tube placement and careful monitoring of pleural fluid drainage. The successful resolution of the patient's symptoms and subsequent discharge highlight the effectiveness of conservative management for transient urine leakage, indicating that non-invasive methods may suffice in similar clinical scenarios [18-20].
Conclusions
This case report highlights the significance of recognizing urinothorax as a rare but potential complication following nephrostomy tube placement and percutaneous nephrolithotomy. Timely identification and appropriate management are crucial, as conservative treatment with chest tube and Foley catheter placement may suffice in cases of transient urine leakage. This case emphasizes the need for individualized clinical judgment to guide patient management, avoiding unnecessary surgical interventions. Increased awareness and understanding of urinothorax can lead to better diagnostic accuracy and patient outcomes in similar clinical scenarios.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Urinothorax, an unusual cause of pleural effusion [Article in French]Rev Pneumol Clin Rakotoarivelo HN Rondeau-Lutz M Groza M Kuhnert C Roy C Weber JC 3723747120152619511510.1016/j.pneumo.2015.01.002 · doi ↗ · pubmed ↗
- 2Urinothorax: a rare pleural effusion Acta Chir Belg Hendriks J Michielsen D Van Schil P Wyndaele JJ 27427510220021224491010.1080/00015458.2002.11679314 · doi ↗ · pubmed ↗
- 3Urinothorax: a new approach Curr Opin Pulm Med Garcia-Pachon E Romero S 2592631220061682587710.1097/01.mcp.0000230628.65515.86 · doi ↗ · pubmed ↗
- 4Unilateral urinothorax can occur contralateral to the affected kidney Scand J Urol Dimitriadis G Tahmatzopoulos A Kampantais S Ioannidis S Radopoulos D Katsikas V 2422434720132272563310.3109/00365599.2012.695391 · doi ↗ · pubmed ↗
- 5Urinothorax: an unexpected cause of severe dyspnea Emerg Radiol Tortora A Casciani E Kharrub Z Gualdi G 1891911220061673893210.1007/s 10140-006-0468-x · doi ↗ · pubmed ↗
- 6Defying gravity: subdiaphragmatic causes of pleural effusions Clin Chest Med Bramley K Puchalski JT 39463420132341105510.1016/j.ccm.2012.12.004 · doi ↗ · pubmed ↗
- 7Urinothorax as a manifestation of nondilated obstructive uropathy following renal transplantation Am J Kidney Dis Carcillo J Jr Salcedo J 21121351985388376210.1016/s 0272-6386(85)80053-6 · doi ↗ · pubmed ↗
- 8Urinothorax-an underdiagnosed cause of acute dyspnea: report of a bilateral and of an ipsilateral urinothorax case Case Rep Emerg Med Laskaridis L Kampantais S Toutziaris C Chachopoulos B Perdikis I Tahmatzopoulos A Dimitriadis G 395653201220122332671310.1155/2012/395653 PMC 3542903 · doi ↗ · pubmed ↗