Diagnostic accuracy of LiquidArray MTB-XDR VER1.0 for the detection of Mycobacterium tuberculosis complex, fluoroquinolone, amikacin, ethambutol, and linezolid susceptibility
Theron Grant

TL;DR
A new test called LiquidArray MTB-XDR was evaluated for detecting tuberculosis and drug resistance, showing high accuracy for some drugs but needing improvement for others.
Contribution
This study evaluates the diagnostic accuracy of the new LiquidArray MTB-XDR test for detecting TB and drug resistance in a large clinical cohort.
Findings
The test showed high specificity (99%) for detecting Mycobacterium tuberculosis complex.
It had high sensitivity for fluoroquinolone resistance (94%) and ethambutol resistance (88%).
The test had moderate sensitivity for amikacin resistance (64%) and detected 86% of linezolid-resistant cases.
Abstract
Drug susceptibility testing (DST) is essential for effectively starting people on effective tuberculosis (TB) regimens. No accuracy data exists for the new high-throughput LiquidArray MTB-XDR (LA-XDR) test, which detects Mycobacterium tuberculosiscomplex (MTBC) and susceptibility to the fluoroquinolones, amikacin, ethambutol, and linezolid (the latter two drugs have no rapid molecular DSTs available). We enrolled (n=720) people with presumptive TB who provided two sputa for Xpert MTB/RIF Ultra and culture (MTBC reference standard). Phenotypic DST and Sanger sequencing served as a composite reference standard. Manual FluoroLyse and automated GenoXtract-fleXT (fleXT) DNA extraction methods were compared. For MTBC, LA-XDR using fleXT-extracted or FluoroLyse-extracted DNA had similar sensitivities (85–87%; which improved upon eluate retesting) and specificities (99%). Drug susceptibility…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
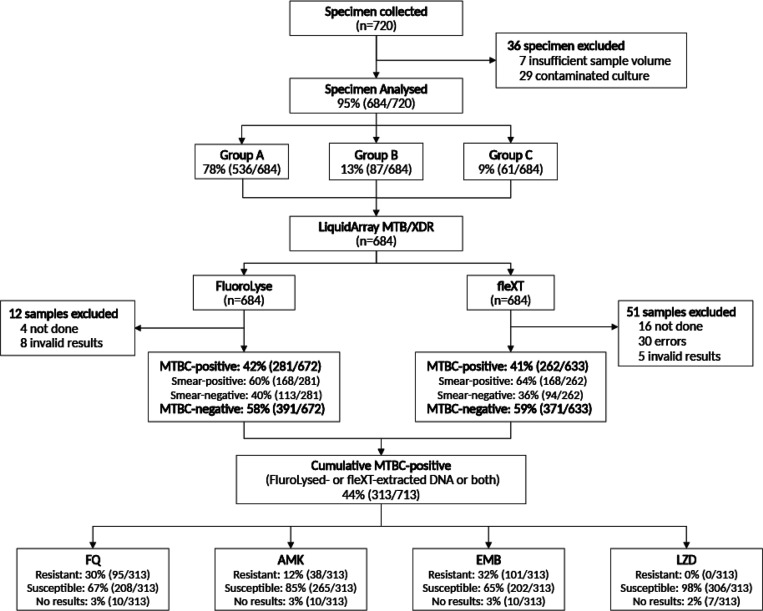 Figure 1
Figure 1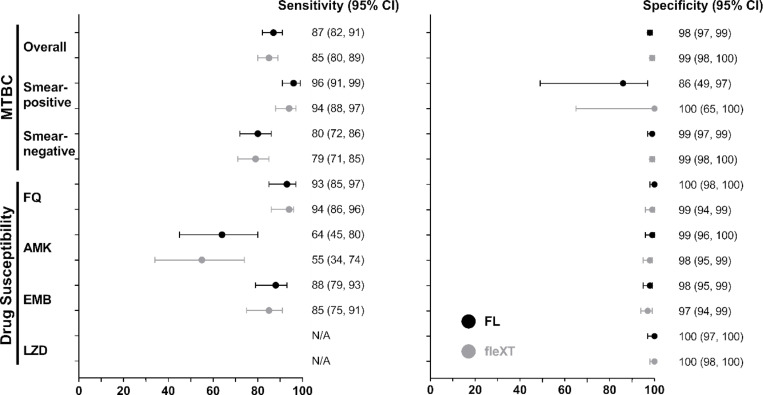 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Tuberculosis Research and Epidemiology · Nephrotoxicity and Medicinal Plants
Introduction
Tuberculosis (TB) remains a devastating global health emergency, with an estimated 7.5 million new cases and 1.3 million deaths in 2022, and an estimated 410,000 multidrug-resistant (MDR) TB cases were reported^1^. The COVID-19 pandemic exacerbated TB management leading to underdiagnosis^1^. Between 2019 and 2022, there was a 15% decrease in drug-resistant (DR)-TB cases potentially obscured by COVID-19^2,3^. In 2022, the World Health Organization (WHO) endorsed a 6-month treatment regimen that incorporates fluoroquinolone (FQ) and linezolid (LZD) for MDR/RR-TB, replacing the longer 9-month or 18-month options^4^.
Current rapid molecular WHO-approved assays face limitations in detecting ethambutol (EMB) resistance, newer and repurposed drugs such as LZD resistance as the two can only be targeted by sequencing or phenotypic drug susceptibility testing (pDST)^5,6^. LiquidArray MTB-XDR VER1.0 (LA-XDR) assay (Bruker/Hain Lifescience GmbH, Nehren, Germany) is a high-throughput (24–94 tests within 3–5 hours) centralised DST. It is a successor to the MTBDRsl line probe assay^7^, integrates within laboratory information systems facilitating rapid results dissemination and, by minimising hands-on manipulation^8^ (only required during initial instrument setup and PCR plate transfer), reduces contamination risk^9^.
LA-XDR utilises the same DNA extraction platform as the WHO-recommended moderate complexity FluoroType MTBDR Ver2.0^10,11^, detects Mycobacterium tuberculosis complex (MTBC), and mutations conferring resistance to FQ in gyrA and gyrB, amikacin (AMK) in rrs, EMB in embB, and LZD in rplC, and rrl genes in both sputum and isolates^5,12–14^. It’s rapid DST, including for drugs for which there are no rapid tests like LZD and EMB offering a crucial component for effective TB management.
Undiagnosed resistance enhances the risk of selection of untreatable strains^13^, in other words, especially as rapid tests for new drugs do not yet exist, one of the best ways to protect them is to maximise the number of effective drugs (for example, fluoroquinolone resistance often precedes bedaquiline resistance^15^). This is the first evaluation of LA-XDR diagnostic performance in MTBC and resistance detection using two distinct DNA extraction methods, the manual FluoroLyse and automated GenoXtract fleXT (fleXT).
Materials and Methods
Study population.
Between 15 January 2020 and 23 May 2022, 720 de-identified sputa from ≥ 18 people with presumptive TB were collected from the National Health Laboratory Services (NHLS), a programmatic government laboratory in Cape Town, South Africa [92% (659/720)] and the FIND Biobank^16^ [8% (61/720)].
Study Samples group.
Group A samples consisted of 87% (572/659) of NHLS samples from individuals with presumptive TB following Xpert MTB/RIF Ultra (Ultra) testing irrespective of smear status (Supplementary Fig. 1). 13% (87/659) of samples from the NHLS were delegated to Group B were Ultra rifampicin-resistant with either FQ-resistance or AMK-resistance confirmed by either Genotype MTBDRsl (MTBDRsl) or pDST at Stellenbosch University (Supplementary Methods). Group C samples (Supplementary Fig. 2) all from FIND consisted of 8% (61/720) of sputa and corresponding isolates with specific resistance confirmed by pDST or whole genome sequencing. Seven LZD phenotypic-resistant isolates from the Stellenbosch University biobank were included.
FluoroLyse and GenoXtract fleXT DNA extraction.
DNA was extracted from sputa sediments and isolates using both the manual FluoroLyse and automated fleXT platform with GenoXtract X2 Extraction VER1.0 (Bruker/Hain Lifescience GmbH, Nehren, Germany) according to the manufacturer’s instructions^17^. A sample consisting of saline was included as a negative control, as well as the provided positive control. At the end of extraction, fleXT reports if the processing was successful or not (reported as an error with code).
LiquidArray MTB-XDR testing.
MTBC and drug susceptibility detection was done using the FluoroCycler XT-96 (Bruker/Hain Lifescience GmbH, Nehren, Germany) instrument. PCRs were set up by the fleXT instrument using DNA extracted using fleXT. A manual PCR reaction was set up with 20 μl of FluoroLyse-extracted DNA added to a pre- mix of 14 μl AM-B and 6 μl AM-A solution per sample. Automated results interpretation was done by the FluoroSoftware XT-IVD (Supplementary Fig. 3). The LA-XDR test results can be categorised into successful (MTBC detected with DST-determinate; MTBC not detected), MTBC detected with DST-indeterminate, invalid and error (applicable to samples extracted with fleXT only).
MGIT960 and phenotypic DST
pDST was done on Group A isolates if the index assay identified resistance. Group B underwent pDST for all drugs for LA-XDR detects resistance, while (Supplementary Methods) Group C only had LZD pDST done (samples were already characterised for FQ, AMK and EMB resistance by either WGS or pDST). pDST used the following WHO critical concentrations of kanamycin 5μg/ml, EMB 5μg/ml, ofloxacin 2μg/ml, moxifloxacin 2μg/ml, AMK 5μg/ml, and LZD 1μg/ml^18^. Negative control was done using the H37Rv (NC_000962) pan-susceptible MTBC strain.
Sanger sequencing.
Sanger sequencing was performed for all LA-XDR DST targets for all isolates from Group B MTBC-positive by LA-XDR. For Group C, sequencing was done on isolates for targets associated with LZD-resistance. Primers (Supplementary Table 1) for all key targets included FQ (gyrA, gyrB), AMK (rrs)^19^, EMB (embB)^20^, and LZD (rrl, rplC)^21^. FASTA files were aligned to the reference sequence of H37Rv (NC_000962) using BioEdit version 7.2.5 (https://bioedit.software.informer.com/7.2/).
Discrepant result analysis.
Repeat testing was done with remnant DNA to resolve result discrepancies, including false-negatives and false-positives detected by LA-XDR using FluoroLyse- or fleXT-extracted DNA. The repeat results were not included in the main analyses but are shown in Supplementary Tables 2–3.
Data Analysis.
Statistical analysis, conducted with Stata 18.0 (StataCorp LP, Texas, USA), involved a two-sample test of proportions. Primary analyses assessed sensitivity and specificity for MTBC using a culture reference standard in Group A and B samples. To assess differences in sensitivity and specificity for the two DNA extraction methods, a McNemar test for paired data was done. P-values ≤ 0.05 were considered significant.
Ethics statement.
This study was done according to relevant guidelines and regulations, approved by the Stellenbosch University Health Research Ethics Committee (N16/04/045 and N09/11/296) and Western Cape Health Research Committee (2016RP18637). Permission was granted to access anonymised to-be-discarded residual samples collected in routine diagnostic practice with waived informed consent.
Results
Study population characteristics.
The median age was 39 years (18, 82) with women constituting 39% (278/713) of participants. 16% (113/713) were people living with HIV, while 41% (295/713) had an unknown HIV status (Table 1). Individuals with a history of previous TB constituted 14% (97/713). Of the samples, 44% (313/713) were culture-positive, with 24% (160/713) smear-positive.
Study samples.
Between 15 January 2020 and 23 May 2022, 720 sputa samples were collected (Fig. 1). 36 sputa were initially excluded because of insufficient volume (n = 7) or contaminated cultures (n = 29).
Error, invalid, and indeterminate results from fleXT and LA-XDR
DNA extraction: Four people did not have sputum extracted using FluoroLyse and 16 people did not have sputa extracted using fleXT. fleXT had an error proportion of 4.5% (30/668) for sputum compared to 2.2% (7/322; p = 0.045) for isolates (Supplementary Tables 4).
Invalid MTBC detection: LA-XDR had a low invalid proportion in sputum testing of 1.3% (8/619) for FluoroLyse and 0.8% (5/607; p = 0.391) for fleXT. On repeat testing using left-over DNA, 100% (8/8) of invalid sputum FluoroLyse extracts became valid while 80% (4/5) by fleXT remained invalid. No invalid results occurred for testing on isolates.
DST Indeterminate: LA-XDR with fleXT DST using sputum, an indeterminate proportion of 38% (25/251) for AMK, 8% (21/251) for FQ and 1% (2/251) for EMB were observed. LZD DST on sputum had a indeterminate proportion of 51% (141/227) for FluoroLyse and 37% (93/251; p = 0.001) for fleXT.
LA-XDR performance compared to the composite reference standard.
MTBC detection: Overall sensitivity was 87% (95% CI: 82, 91) and 85% (80, 89; p = 0.528) by FluoroLyse and fleXT, respectively (Table 2). In smear-positive sputa extracted using FluoroLyse, sensitivity was 96% (91, 99) and specificity 86% (49, 97), compared to fleXT with a sensitivity of 94% (88, 97; p = 0.494) and a specificity of 100% (65, 100; p = 0.305). In smear-negative sputa, sensitivity was 80% (72, 86), with 99% (97, 99) specificity for FluoroLyse, while for the fleXT, sensitivity was 79% (71, 85; p = 0.839) and specificity 99% (97, 100; p > 0.999) (Fig. 2). Retesting false-negative FluoroLyse-extracted DNA eluates detected MTBC in 50% of smear-positive (2/4) and smear-negative (18/36) samples whereas retesting using fleXT-extracted eluates resulted in no MTBC detection in smear-positive (0/6) but 20% of smear-negatives (8/41). Using isolates, sensitivity was 98% (96, 99) by FluoroLyse compared to 99% (97, 100) for fleXT with specificity estimates of 93–100% for both methods. Three out of five isolates missed by LA-XDR were non-tuberculous mycobacteria by sequencing of rrs (Mycobacterium intracellulare, Mycobacterium avium, Mycobacterium elephantis), perhaps indicating mixed infection.
Fluoroquinolones: LA-XDR showed a sensitivity of 93% (95% CI: 85, 97) and 94% (86, 98) using FluoroLyse and the fleXT, respectively, with a specificity of 100% (98, 100) for FluoroLyse and 99% (96, 100) for fleXT (Table 3) on sputa. Using isolates, sensitivity was 92% (85, 94) and 92% (85, 96) for FluoroLyse and fleXT, respectively with a specificity of 100% (97, 99) for both. LA-XDR on FluoroLyse-extracted DNA showed comparable performance to MTBDRsl with a sensitivity of 92% (80, 97) vs 90% (76, 96; p = 0.758) on sputum and 93% (84, 97) vs 88% (77, 94; p = 0.359) on isolates (Supplementary Table 5). Based on successful results, in a hypothetical population of 100 smear-negative FQ resistance cases using fleXT (Supplementary Table 6), 24% (24/100) could be missed due to 1 fleXT error and, for LA-XDR, 2 invalid results, 15 MTBC-negative, 6 FQ-indeterminate, and 1 false-susceptible due to the sensitivity decrement.
Amikacin: LA-XDR showed a sensitivity of 64% (95% CI: 45, 80) and 55% (34, 74) using DNA extracted by the FluoroLyse and the fleXT platform respectively with a specificity of 99% (96, 100) for FluoroLyse versus 98% (95, 99) for fleXT in sputum samples. In isolates, sensitivity improved to 69% (95% CI 54, 81) for FluoroLyse compared to 72% (56, 84; p = 0.771) for fleXT with a specificity of 100% (98, 100) for both platforms. The assay demonstrated comparable performance to MTBDRsl with a sensitivity of 71% (45, 88) on sputum and 74% (54, 88) on isolates. In a hypothetical population of 100 smear-negative AMK resistance cases using fleXT, 53% (53/100) could be missed due to 1 fleXT error and, for LA-XDR, 2 invalid results, 15 MTBC-negative, 31 AMK-indeterminate, and 4 false-susceptible.
Ethambutol: LA-XDR had a sensitivity of 88% (95% CI: 79, 93) with FluoroLyse and 85% (75, 91) for fleXT with a specificity of 98% (95, 99) for FluoroLyse and 98% (95, 99) for fleXT. In isolates, sensitivity was 90% (83, 95) and 91% (76, 92) for the FluoroLyse and fleXT respectively with a specificity of 100% (97, 100) for both DNA extraction methods. In a hypothetical population of 100 smear-negative EMB resistance cases using fleXT, 23% (23/100) could be missed due to 1 fleXT error and, for LA-XDR, 2 invalid results, 15 MTBC-negative, 1 EMB-indeterminate, and 4 false-susceptible.
Linezolid: The assay exhibited a specificity of 100% (95% CI: 97, 100) for both methods. However, sensitivity could not be precisely assessed due to few resistant cases. LA-XDR detected 86% (6/7) of phenotypic-resistant isolates, with one being susceptible. All isolates with resistance detected by LA-XDR had the C-154-R rplC resistance-associated variant^22^.
Discussion
Our data shows that using sputum, LA-XDR has: 1) high sensitivity for MTBC detection using either DNA method, 2) comparable FQ and AMK sensitivity and specificity to MTBDRsl, 3) high sensitivity and specificity for EMB resistance and 4) potential as a rule-in test for LZD resistance detection, particularly in where the rplC C-154-R variant is most frequent. Additionally, LA-XDR has relatively low indeterminate rates, however, due to suboptimal sensitivity for MTBC (~ 80% in smear-negatives), at least 20% of people will not have a susceptibility result generated.
LA-XDR sensitivity for MTBC (87%) is comparable to that of other WHO-approved high throughput, moderate complexity NAAT platforms (Abbott RealTime MTB-RIF/INH, Roche COBAS MTB-RIF/INH, BD MAX MDR-TB and FluoroType MTBDR)^9,23^. As expected, sensitivity in smear-negative specimens was diminished (80% vs. 96% for smear-positives), meaning that 20% (28/137) of smear-negative TB cases will be missed (and therefore, due to non-detection of MTBC DNA by LA-XDR, not have resistance or susceptible results generated, potentially resulting in missed resistance). Our results indicate that retesting smear-negative samples almost half the time leads to successful MTBC detection, which is valuable information for refining diagnostic algorithms. Additionally, if LA-XDR is employed as a reflex test following an initial positive TB screening, we recommend repeating the test using the remaining DNA extract.
Sputum FQ and AMK susceptibility sensitivity and specificity were comparable to those for MTBDRsl and like those for Xpert MTB/XDR^6,24,25^. FQ sensitivity (94%, independent of DNA extraction method) met the WHO target product profile (TPP) of > 90% sensitivity^26^. LA-XDR is promising in detecting EMB resistance, with sensitivity and specificity estimates of 88% and 98%, respectively. This is important because EMB is included in the management of MDR-TB in most clinical settings. The LA-XDR is the only option for programmes to do EMB DST and will fill the existing diagnostic gap as there is a high EMB resistance prevalence among MDR-TB^27^.
LZD is a key WHO group A drug regimen, LA-XDR has 100% specificity which makes it a valuable tool for ruling out LZD resistance. The test accurately detected the rplC mutation^5,28^ in phenotypic-resistant isolates and detected the most resistant specimens, demonstrating its potential for LZD susceptibility testing, especially in the context of no other commercially available molecular tools for susceptibility testing for this drug. On sputa samples, more than half (141/227) had indeterminate LZD results, possibly due to a high detection call threshold or unclear variant significance.
We demonstrated low AMK sensitivity estimates (64%), likely due to selection bias in FIND Biobank samples from Eastern Europe with the prevalent C-14-T eis promoter variant^22^ undetected by LA-XDR. WHO classifies the C-14-T eis promoter mutation as provisionally associated with resistance, it can only confer resistance if linked to a functional eis^22^ A substantial proportion (77/106) of indeterminate AMK results (MTBC-positive) were from smear-negative sputa samples, likely due to low bacillary load or difference detection thresholds.
In summary, our data shows that, while LA-XDR is adept at detecting and ruling in resistance, its potential impact is, like many molecular DSTs, undermined by its ability to detect TB (required to generate a DST result) (Supplementary Table 6). For example, in a hypothetical population of 100 smear-negative cases with FQ resistance, 24% (24/100) will be missed.
Our study had limitations, even though we had a large sample size, our cohort had no clinical specimens with LZD resistance, but we included phenotypic-resistant isolates detected by LA-XDR. Using Ultra test results for selection of Group A and B samples introduces variability, and likely could overestimate MTBC sensitivity, but reflects real-world scenarios where LA-XDR would likely be used in many settings. Lastly, we did not evaluate the utility of repeating LA-XDR on sputum, except for false-negative results.
In conclusion, the LA-XDR meets the criteria WHO TPP for a sputum-based next-generation WHO moderate complexity NAAT technology. The LA-XDR can be a valuable tool for MTBC detection and drug susceptibility profiling, especially for LZD and EMB resistance, for which no other commercial molecular DSTs are presently available. Future work should focus on improving the detection of smear-negative TB cases, ensuring that this technology can be effectively utilised in a broader range of clinical scenarios.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (2023) Global tuberculosis report 2023. World Health Organization, Geneva
- 2Naidoo P, Theron G, Rangaka MX (2017) The South African Tuberculosis Care Cascade: Estimated Losses and Methodological Challenges. J Infect Dis 216(suppl 7):S 702–s 1329117342 10.1093/infdis/jix 335PMC 5853316 · doi ↗ · pubmed ↗
- 3Cox H, Dickson-Hall L, Ndjeka N (2017) Delays and loss to follow-up before treatment of drug-resistant tuberculosis following implementation of Xpert MTB/RIF in South Africa: A retrospective cohort study. P Lo S Med ; 14(2).10.1371/journal.pmed.1002238 PMC 531964528222095 · doi ↗ · pubmed ↗
- 4World Health Organization (2022) WHO Consolidated guidelines on tuberculosis: Module 4: Treatment - Drug-susceptible tuberculosis treatment 35727905 · pubmed ↗
- 5Georghiou SB, de Vos M, Velen K (2023) Designing molecular diagnostics for current tuberculosis drug regimens. Emerg Microbes Infect 12(1):217824336752055 10.1080/22221751.2023.2178243 PMC 9980415 · doi ↗ · pubmed ↗
- 6Theron G, Peter J, Richardson M (2014) The diagnostic accuracy of the Geno Type(®) MTBD Rsl assay for the detection of resistance to second-line anti-tuberculosis drugs. Cochrane Database Syst Rev ; (10): Cd 01070510.1002/14651858.CD 010705.pub 2PMC 444821925353401 · doi ↗ · pubmed ↗
- 7Theron G, Peter J, Richardson M, Warren R, Dheda K, Steingart KR (2016) Geno Type(®) MTBD Rsl assay for resistance to second-line anti-tuberculosis drugs. Cochrane Database Syst Rev 9(9):Cd 01070527605387 10.1002/14651858.CD 010705.pub 3PMC 5034505 · doi ↗ · pubmed ↗
- 8David A, de Vos M, Scott L (2023) Feasibility, Ease-of-Use, and Operational Characteristics of World Health Organization-Recommended Moderate-Complexity Automated Nucleic Acid Amplification Tests for the Detection of Tuberculosis and Resistance to Rifampicin and Isoniazid. J Mol Diagn 25(1):46–5610.1016/j.jmoldx.2022.10.001PMC 983053236243289 · doi ↗ · pubmed ↗