Gastroesophageal Disease and Environmental Exposure: A Systematic Review
Daniel Hyun Kim, Sanjiti Podury, Aida Fallah Zadeh, Sophia Kwon, Gabriele Grunig, Mengling Liu, Anna Nolan

TL;DR
This review explores how environmental exposures like air pollution and smoking are linked to upper gastrointestinal diseases.
Contribution
The study highlights waterpipe use as a new risk factor for gastroesophageal reflux and gastric cancer.
Findings
PM exposure increases the risk of upper gastrointestinal diseases.
Smoking is confirmed as a major risk factor for aerodigestive diseases.
Waterpipe use is significantly associated with gastroesophageal reflux and gastric cancer.
Abstract
Environmental exposure-associated disease is an active area of study, especially in the context of increasing global air pollution and use of inhalants. Our group is dedicated to the study of exposure-related inflammation and downstream health effects. While many studies have focused on the impact of inhalants on respiratory sequelae, there is growing evidence of the involvement of other systems including autoimmune, endocrine, and gastrointestinal. This systematic review aims to provide a recent update that will underscore the associations between inhalation exposures and upper gastrointestinal disease in the contexts of our evolving environmental exposures. Keywords focused on inhalational exposures and gastrointestinal disease. Primary search identified n = 764 studies, of which n = 64 met eligibility criteria. In particular, there was support for existing evidence that PM increases…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
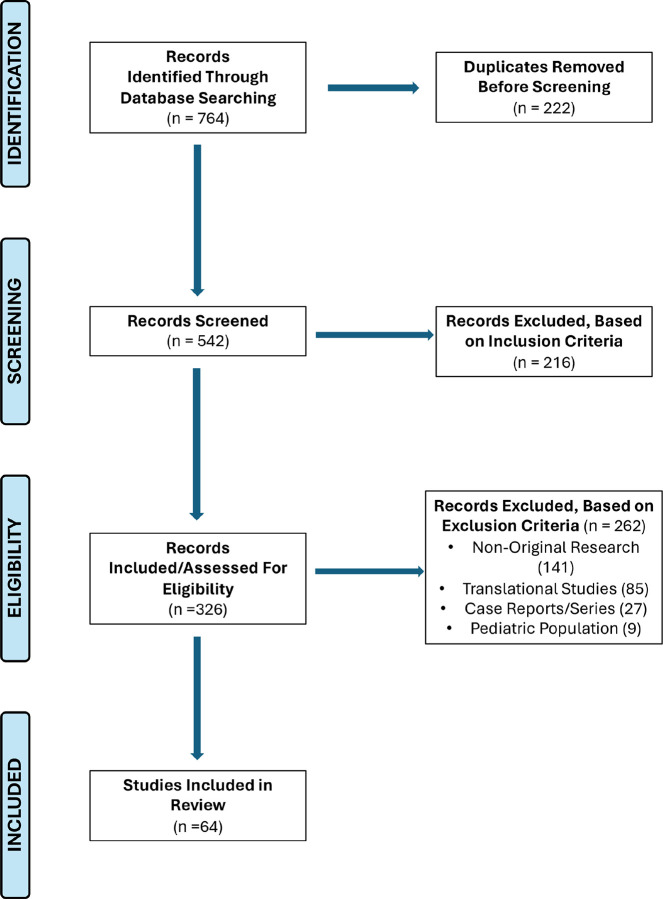 Figure 1
Figure 1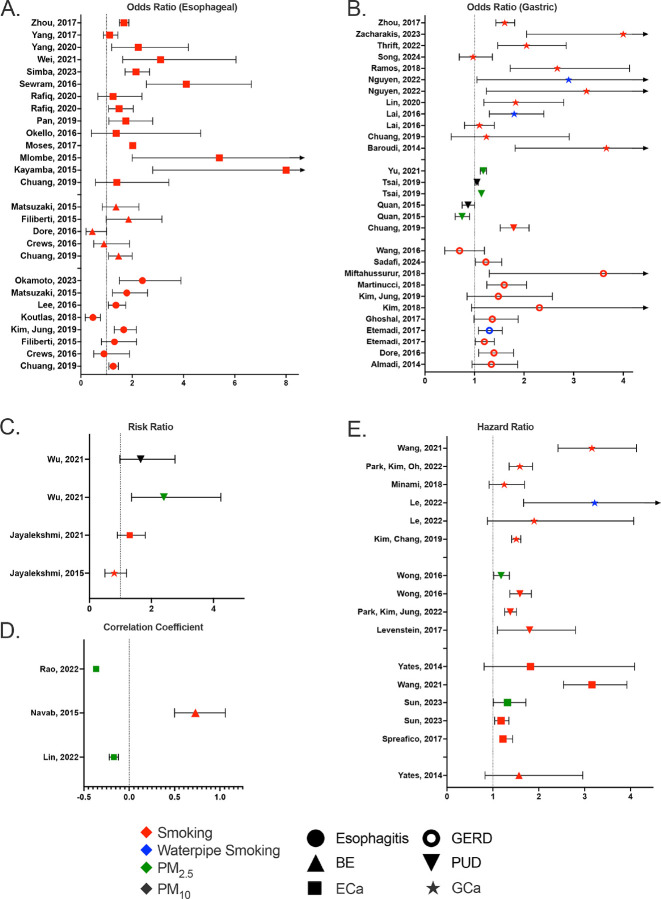 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAir Quality and Health Impacts · Climate Change and Health Impacts · Global Health Care Issues
INTRODUCTION
Exposome-associated morbidity and mortality is a global health concern. Environmental exposures that individuals encounter over their lifetimes include air pollution, water pollution, diet, and radiation. The exposome’s rate, volume, and variety have been linked to heterogenous negative health effects, but mechanisms remain elusive in many disease states. Studying the exposome provides valuable insights into the interplay between environmental factors and human health.^1^ Of the various environmental exposures, inhalational exposure has been of great interest, especially in the context of rising levels of global air pollution due to global warming, wildfires, wars, and population growth.
Studies investigating the link between environmental exposures and disease have the potential to impact millions globally. Air pollution is associated with 7-million premature deaths annually, and levels have steadily risen over the past few decades.^2–3^ Over half of the world’s population are exposed to levels of air pollution that are substantially above the WHO Air Quality Guidelines.^4^ There are a greater proportion of non-communicable disease attributable to environmental exposure in developing countries that utilize industrial production factories, primary contributors to emissions.^5^
Particulate matter (PM) exposure, in particular, is a global cause of significant aerodigestive morbidity and mortality.^6–46^ The destruction of the World Trade Center (WTC) on September 11, 2001 (9/11) led to intense PM exposure of first responders and inhabitants of New York City (NYC).^15–46^ WTC-PM exposure is associated with obstructive airways disease (OAD). PM was also found to have associations with gastroesophageal diseases, such as gastroesophageal reflux disease (GERD) and Barrett’s Esophagus (BE).^47–49^ Approximately 44% of WTC rescue/recovery workers had developed GERD symptoms by 2005.^50^ In contrast, GERD has a prevalence of 20% in the US.^51 53^ There is also evidence of comorbid GERD and OAD, as WTC-exposed firefighters with OAD had 3-fold higher risk of developing GERD.^49,54^
GERD is the most prevalent gastrointestinal disorder affecting at least 20% of the US population, and leading to substantial morbidity.^55^ Globally, GERD prevalence is 10–25%.^55,56^ Aerodigestive complications also include BE, and malignancy such as esophageal adenocarcinoma (EAC).^15,57,58^
Aerodigestive disease can also induce or worsen respiratory disease such as airway hyperreactivity (AHR). This may be explained by the clearing mechanism of the respiratory system and its close proximity to the digestive system at the pharynx. However, this is an area of active investigation.^59^ Prior systematic reviews on the topic have only focused on single inhalational exposures and/or single diseases/outcomes.^60–65^
Our systematic review focuses on the exposome in a more holistic manner in order to assess its effects on the scope of gastroesophageal diseases on a greater scale. We investigated the associations between exposure (particulate matter, smoking, waterpipe smoking) with diseases of the upper gastrointestinal tract (GERD, Barrett’s and malignancy).
METHODS
Review Strategy.
Our systematic review adhered to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) guidelines.^66,67^ Our Population, Exposure, Outcome (PEO) question was to investigate among adult populations (P) whether there is an association between inhalational exposure (e.g., air pollution, cigarette/tobacco smoke, marijuana smoke, vape/e-cigarette aerosols) (E) and esophageal or gastric disorders/disease (O).
PubMed searches were conducted on May 1, 2024 as per the protocol of our systematic review registered on PROSPERO on April 29, 2024 and can be accessed at Prospero ID 536834. The following MeSH Terms were searched for using the MeSH Database:
(“Particulate Matter”[Mesh]) OR (“Vaping”[Mesh]) OR (“Smoking”[Mesh]) OR (“Smoking Devices”[Mesh]) OR (“Tobacco Use”[Mesh]) OR (“Tobacco Use Cessation Devices”[Mesh]) OR (“Electronic Nicotine Delivery Systems”[Mesh]) OR (“E-Cigarette Vapor”[Mesh]) OR (“Inhalant Abuse”[Mesh]) OR (“Marijuana Smoking” [Mesh]) OR (“Marijuana Use”[Mesh]) OR (“Marijuana Abuse”[Mesh]) OR (“Cannabis”[Mesh]) OR (“Cannabinoids”[Mesh])
[AND]
(“Stomach Diseases”[Mesh]) OR (“Esophageal Diseases”[Mesh])
The complete listing of associated terms that were searched for with each of the above Mesh terms, can be found at MeSH Database. For example, when searching for “stomach diseases” under its associated Mesh term, we were able to search for Reflux, Gastritis, Peptic Ulcer, Stomach Neoplasms, Zollinger-Ellison syndrome, etc. Reference-list screening was also used.
For this review, we have defined environmental exposure to include PM_2.5_, PM_10_, tobacco/cigarette smoke, vape/e-cigarette aerosols, and marijuana/cannabinoid inhalation. We have defined esophageal and gastric disease to include the following: gastroesophageal reflux disease (GERD), Barrett’s Esophagus (BE), peptic ulcer disease (PUD), esophagitis, gastritis, esophageal cancer, and stomach cancer.
Study Criteria.
Studies were included if they (1) discussed the environmental/occupational exposure to inhalants, specifically, PM_2.5_, PM_10_, tobacco/cigarette smoke, marijuana smoke, and/or vape/e-cigarette vapor, (2) evaluated effects of exposures on esophageal or gastric diseases, (3) performed on adult human subjects, (4) were written in English, and (5) were published within the last 10 years.
Studies were excluded if they (1) were not original research, (2) consisted of translational research, (3) were case reports or series, or (4) were conducted on a pediatric population.
Data Extraction.
Articles were reviewed and data regarding study design, patient characteristics, sample size, and tool used were extracted. Results from database searches were filtered for full-text articles, human subjects, English language, and publication date and imported into Endnote X9. Original research papers were reviewed for (title, abstract, and full text) to ascertain eligibility. We examined references cited in the relevant articles. All results were screened by DHK and SP and further independently evaluated by AN. Disagreements were resolved by consensus.
Risk of Bias Assessment.
Systematic review inherent bias (selection, detection, performance, and reporting) was addressed through study design/search algorithm. Selection bias was addressed by having predetermined inclusion, exclusion criteria and distinct definitions. Detection and performance bias were addressed by having at least two rounds of screening individually performed by DHK and SP. Reporting bias was minimized by using PubMed search filters for peer-reviewed published articles of human subjects written in English and removing duplicates.
The Newcastle-Ottawa Scale (NOS), a domain-based approach was used to assess the degree of bias.^68^ Scales adapted for case-control and cross-sectional studies were used. Total scores obtained by the scale were converted to AHRQ standards or as done in previous studies to reflect the quality of each paper: “good” (green), “fair” or “satisfactory” (yellow), and “poor” or “unsatisfactory” (red).^69^
Ethics Approval.
This study does not require ethical approval as it involves a review of publicly available research and utilized anonymized original data.
RESULTS
Literature Search.
A total of 764 studies were identified from PubMed and reference-list screening, Fig. 1. After removal of 222 duplicates, 542 articles were screened. Following application of inclusion criteria, 216 articles were excluded and 326 articles were assessed for eligibility based on exclusion criteria. Application of exclusion criteria involved removal of 141 non-original research articles, 85 translational studies, 27 case reports/series, and 9 pediatric studies for a total of 262 articles. N = 64 original research articles were considered eligible and included in this review. Data from screening and extraction are available, Supplemental Tables 1–6.
Risk of bias using NOS was assessed in cohort (N = 20), case-control (N = 23), and cross-sectional studies (N = 18), Supplemental Table 7. Two studies that were case-crossover studies and one study that was an ecological study were unable to be assessed for risk of bias as the NOS and our adaptations did not cover for these types of studies. Scores obtained from the NOS were adapted as in previously published studies to reflect the quality of each paper.^69^ Cutoffs for each risk of bias assessment depending on article type can be found within the footnote of Supplemental Table 7. Among cohort studies, N = 15 articles were of good quality, N = 1 of fair quality, and N = 4 of poor quality. Among case-control studies, N = 15 were of good quality, N = 5 of fair quality, and N = 3 of poor quality. Among cross-sectional studies, N = 14 were of good quality, N = 2 of satisfactory quality, and N = 2 of unsatisfactory quality.
Study Characteristics.
The populations of patients with esophageal or gastric disease included those afflicted with esophagitis (n = 8), BE (n = 8), ECa (n = 24), GERD (n = 11), PUD Fig. 1. Study design per Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Guidelines. PRISMA is an evidence-based minimum set of items for reporting in systematic reviews and meta-analyses.^66,67^
(n = 9), and GCa (n = 16). Studies that focused on any other outcomes did not meet exclusion/inclusion criteria. The exposures that were investigated in particular were smoking, waterpipe smoking, and PM_2.5_/PM_10_ exposure. While there were no studies that focused on marijuana smoking or vaping/e-cigarettes that met our inclusion/exclusion criteria we know from the literature that use of cannabinoids and vaping are linked to the development of gastrointestinal disorders.^134^ One study investigated the role of exposure to second-hand smoke, in addition to direct cigarette smoke exposure.^110^ Most studies produced an odds ratio (OR), risk ratio (RR), correlation coefficient (CC), or hazard ratio (HR) to measure each of the risks associated with their respective exposures for a particular outcome, of which are summarized in Fig. 2 (see raw data in Supplemental Table 8A-E). Among those studies, some reported using adjusted models in their analyses. Additionally, other studies focused on the percent presentation of risk factors;^72,86^ risk by measuring the increase in incidence of the respective disease;^91–93,114^ the differences in mortality with respect to magnitude of exposure^95^, and utilized a novel predictive model to identify risk factors.^115^ Table 1.
Esophagitis.
Current tobacco use was identified as a significant risk factor for reflux esophagitis (RE).^73,77,97,104^ When studying gender-specific differences between smoking and risk of RE, Kim, Jung, et al found that smoking led to greater risks of RE among women compared to men.^84^ Associations between smoking and eosinophilic esophagitis (EE) were also investigated. Some studies found that EE were significantly less likely to have ever smoked cigarettes compared to non-EE controls, but smoking was not significantly associated with increased risk of EE.^74,86^ Lee, et al, however, identified smoking as a significant risk factor for asymptomatic EE (AEE).^89^
Barrett’s Esophagus.
Smoking was identified as a risk factor for BE.^73,97^ Schmidt, et al found that BE cases were significantly more likely to smoke.^114^ Navab, et al found positive correlation between current and prior tobacco use and BE.^102^ Etemadi, et al found associations between smoking and BE that were independent of intensity, age at initiation, and GERD, but dependent on duration and years since cessation.^76^ Other studies, however, produced conflicting results: some studies found that current and former smoking were not significantly associated with BE.^75,130^
Gastroesophageal Reflux Disease.
Multiple studies identified smoking as a risk factor for GERD.^75,78,96,98,113^ Kim, Jang, et al interestingly found that former smoking was significantly associated with risk of GERD, while current smoking was not significantly associated.^83^ When investigating gender-specific differences on the effects of smoking on the risk of GERD, Kim, Jung, et al found that smoking increased risks in both men and women.^84^
One study investigated the effects of waterpipe smoking in addition to traditional cigarette smoking on the risk of GERD. Etemadi, et al found that waterpipe smoking was most strongly associated with “severe and frequent” reflux, and prevalence of the disease was associated with waterpipe use and duration. In addition, they found that cigarette smoking was a significant risk factor of any form of reflux among men.^76^
Conversely, some studies noted no significant association between GERD and smoking. Almadi, et al observed a higher prevalence of GERD among smokers than non-smokers, but found no significant difference.^70^ Wang, Leena, et al also did not find any association between cigarette smoking and risk of GERD.^123^
One study, Seo, et al, developed a prediction model that was significantly able to predict GERD-related medical utilization in the South Korean population and identified PM_2.5_ as a risk factor for GERD.^115^
Peptic Ulcer Disease.
Chuang, et al identified current tobacco use as a significant risk factor for PUD and that higher cumulative amounts of tobacco use were at higher risk for PUD.^73^ Further, Begovic, et al found that more than half of ulcer patients enrolled into their study were smokers, and this difference was significant when compared to the those who were non-smokers.^72^ Levenstein, et al observed that age-, gender-, and socioeconomic status-adjusted associations were significant for smoking.^90^
Park, Kim, Jung, et al investigated the role of changes in smoking status in risk of gastroduodenal ulcer. They observed that changes in smoking status from never smoker, quitter, and current smoker, to current smoker in particular had relatively higher HRs than other groups. When comparing smoking amount levels, they found that smokers who smoked > 20 pack-years had significantly higher risk than lighter smokers.^107^
Other studies had investigated the role of PM exposure in risk of PUD. Tsai, et al found that increases in both PM_2.5_ and PM_10_ were significantly associated with increased risk of PUD hospitalizations on warm days, but only PM_10_ was significantly associated on cold days.^122^ Similarly, Wong, et al found that PUD hospitalization was associated with 10 ug/m^3^ increases in PM_2.5_. When investigating different types of ulcers, they found that associations with PM_2.5_ were significant for gastric ulcers, but not for duodenal ulcers.^126^ Wu, et al observed that cumulative RRs for PM_2.5_ and PM_10_ showed nearly linear adverse effects.^127^ When looking at gender-adjusted differences, significant associations for men and women were only observed for PM_2.5_.
Quan, et al found that when air pollution exposures were assessed over 3-, 5-, and 7-day averages, pollutants were inversely associated with upper gastrointestinal bleeding (UGIB).^109^ Yu, et al observed a potential dose-response relationship between quartile concentrations of PM_2.5_ one month prior to detection of PUD. Subjects in the highest quartile of PM_2.5_ exposure displayed significantly higher risk and the detection of PUD was associated with a 10 ug/m^3^ in PM_2.5_.^131^
Esophageal Cancer.
Many studies found associations between smoking and ECa.^101,116,133^ Other studies focused on esophageal squamous cell carcinoma and also identified smoking as a risk factor and this risk increased with tobacco intensity and smoking duration, but no significant difference with respect to macroscopic type of cancer, as smoking showed similarly increased risks for both ulcerative type and medullary type eosinophilic squamous cell carcinoma (ESCC).^81,85,100,117,125,128^ Jayalekshmi, et al observed higher risks of ESCC for current bidi and cigarette smokers.^80^ Conversely, some studies observed non-significant relationship between inhalational exposures and ECa.^73,105,129^
Some studies looked at how smoking affected survival for those afflicted with ECa. Spreafico, et al found that smoking conferred worse overall survival in the combined Boston-Toronto Cohort for each 20 pack-year increase.^119^ Other observed how current and former smoking contributed to decreased survival with respect to subtype, specifically ESCC and esophageal adenocarcinoma (EADC).^124,130^
One study in particular, Rafiq, et al evaluated both smoking and second-hand smoke as a risk factor for ECa, with increased risks associated with either exposure.^110^ Another study, Pan, et al focused on associations between smoking and esophageal precancerous lesions (EPL) and found that consuming more than 30 cigarettes/day or having 40 or more pack-years of cumulative smoking was significantly associated with EPL.^106^
Other studies investigated the relationship between PM_2.5_ exposure and ECa. Li, Guo, et al observed a significantly positive association between PM_2.5_ and ECa incidence. When investigating the corresponding lag effects on ECa incidence, they found that a lag effect of 4 years showed the greatest risk for males and females.^91^ Li, Jing, et al examined the modifying effects of urbanization and socioeconomic factors and found a stronger association between PM_2.5_ and incidence for low urbanization groups, and this association was stronger for females than males.^92^ Li, He, et al identified long-term exposure to black carbon, organic carbon, nitrate, and ammonium to be significantly associated with ECa.^93^ Rao, et al found that although spatial distributions of hospitalization rate of ECa in 2016 were not consistent with that of PM_2.5_ concentration in the same year, concentrations of PM_2.5_ in 2003 and 2004 had the strongest correlations with hospitalization rate in 2016.^112^ Sun, et al observed a linear concentration-response relationship between long-term PM_2.5_ and ECa.^120^ Conversely, Lin, Shih, et al observed that the average number of deaths due to ECa decreases with increasing average PM_2.5_ concentration.^95^
Gastric Cancer.
As with the previous outcomes, most studies identified smoking as a risk factor for GCa.^71,111,132,133^ Current cigarette smoking status was found to be attributed to increased risk of GCa and this risk increased among those with longer durations of smoking or later starting ages of smoking.^94^ Current smoking was also found to have increased risk of stomach cancer death.^99^ When assessing changes in smoking status, one study found that those who changed to their current status to “smoking” showed increased risk of GCa and this risk was the highest in heavier smokers.^108^ One study found that smoking was only significantly associated with single GCa and synchronous multiple gastric cancer (SGMCa) in advanced gastric cancer (AGCa) patients.^118^ Current smoking also showed increased risk for gastric adenocarcinoma (GAC) and gastric non-cardia adenocarcinoma (GNCA).^124^ Interestingly, Jayalekshmi, et al found that bidi smoking was significantly associated with GCa risk, but cigarette smoking was not. This risk increased with the number of bidis smoked daily and with duration of bidi smoking.^79^ Conversely, Chuang, et al found that tobacco use was a non-significant risk factor for GCa.^73^ Other studies found that current smoking increased risks of intestinal metaplasia for both men and women. Further, this risk increased with increasing duration and total dose.^82,121^
Some studies investigated the role of waterpipe smoking in GCa risk. Several studies in Vietnam showed that water pipe smoking was positively associated with GCa risk, but there was no significant interaction between the effects of water pipes and cigarette smoking on GCa risk.^87,88,103^ Li, He, et al found that long-term exposure to black carbon, organic carbon, nitrate, ammonium, and sulfate was significantly associated with stomach cancer.^93^
DISCUSSION
In this systematic review, we investigated the associations between environmental exposures and diseases of the upper gastrointestinal tract. Through a comprehensive review of the available literature, we identified complex relationships between environmental exposures and upper gastrointestinal diseases. Most of the studies showed that exposures including particulate matter, smoking, and waterpipe were significantly associated with higher risk of aerodigestive diseases.
Particulate matter (PM) exposure is a global cause of significant pulmonary morbidity and mortality.^6–46^ Our review supports existing evidence suggesting that exposure to PM may also increase the risk of diseases affecting the upper gastrointestinal tract. Studies included in this review demonstrated links between PM exposure and an increased risk of ECa and PUD, although the underlying mechanisms remain to be fully explained. These findings highlight the importance of considering environmental factors, such as air pollution, in the context of upper gastrointestinal health. PM consists of various harmful compounds which can trigger inflammatory responses, oxidative stress and DNA damage that contribute to the development of cancer and ulceration. Moreover, studies showed that PM may disrupt the gut microbiota, leading to increased risk of gastrointestinal inflammation and cancers.^135^
Cigarette smoking has been recognized as a major risk factor for various cancers, including those of the gastrointestinal tract. Consistent with previous research, our review highlights the detrimental effects of smoking on the upper gastrointestinal tract, with a notable association observed between smoking and an elevated risk of Barrett’s esophagus, GCa, ECa and PUD. The carcinogenic effect of smoking is attributable to mutations in critical genes caused by tobacco metabolites and chemicals. Smoking is also associated with progression, aggressiveness, and reduced survival rates of existing gastrointestinal cancers. Smoking may be associated with exacerbation of GERD symptoms due to reducing esophageal sphincter tone and increasing gastric acid production.^136^
Waterpipe smoking has increased worldwide due to a perception that it is less harmful than cigarette smoking. However, waterpipe smoke contains tobacco and several toxicants that may increase the risk of developing aerodigestive disease, as identified in our review. Numerous carcinogens have been identified in waterpipe smoke including polycyclic aromatic hydrocarbons (PAHs), volatile aldehydes, and heavy metals, which can cause DNA damage and develop cancer over time.^137^ Moreover, emerging evidence suggests that vaping and marijuana use may also impact gastrointestinal health, although further investigation is warranted to better understand the nature of these associations.
Gastrointestinal symptoms associated with vaping can occur in more than half of exposed patients.^138,139^ The gastrointestinal symptoms are thought to be directly related to the inhalation of nicotine; users of novel nicotine delivery products (vapers) usually take in higher doses of nicotine than tobacco smokers.^140^ Nausea, vomiting, diarrhea and abdominal pain are also signs of with E-cigarette or Vaping Product Use-Associated Lung Injury (EVALI), as indicated in several case reports.^141^ In a survey of UK vapers (that met our exclusion criteria), the incidence of the new symptom vomiting amongst “current vapers” was 13.0% and 21% for nausea. Current vapers using cannabinoid-based substances reported nausea significantly more frequently than other groups. Respondents reporting vomiting/nausea were given the diagnosis of gastritis or gastroenteritis. The incidence of nausea and vomiting was not increased in exclusive vapers compared to concurrent smokers and vapers.^142^
In tobacco smokers, due to the burning process, nicotine can be transformed into nitrosamines via nitrosation, and many of these nitrosamines, such as nicotine-derived nitrosamine ketone (NNK) and N-nitrosonornicotine (NNN), are potent carcinogens linked to esophageal and stomach cancer.^143,144^ Novel delivery devices such as e-cigarettes produce 5% as much nitrosamines compared to standard burning tobacco products, leading to an assumption that e-cigarettes are safer than cigarettes and could be used as cessation aids. However, translational in vitro and murine studies showed that nicotine from e-cigarette induced carcinogenic DNA-adducts and inhibited DNA repair just like nicotine-derived nitrosamine ketone (NNK). Because it often takes over two decades for tobacco smokers to develop cancer, mice were exposed to e-cigarette vapors for one year and had their organs examined. While cancers were detected in the lungs of the mice due to e-cigarette exposure, cell hyperplasia also occurred in the bladder epithelium, raising the possibility that although e-cigarette exposure is inhalational, it can cause systemic cancers.
Furthermore, the nicotinic acetylcholine receptor (nAChR), a genetic variant of which is consistently linked to lung cancer in large genetic studies, might mediate carcinogenesis through directly binding nicotine (and nitrosamines) in airway epithelium. This mechanism could provide direct carcinogenesis of nicotine and nicotine-metabolites to all cells that express the nAChR, particularly in carriers of the variants that are associated with tobacco smoking and cancer.^145–148^ Following the idea that inhaled nicotine could produce carcinogenic molecules in human users, an untargeted metabolomics analysis of urine demonstrated a trend of increased carcinogen biomarkers in the samples of a relatively small cohort of vapers (n = 34 vs. n = 45 non-users).^149^
Limitations
While this systematic review provides valuable insights into the associations between environmental exposures and upper gastrointestinal diseases, the included studies vary in design, methodology, and population characteristics, which may introduce heterogeneity and bias. Some studies used adjusted models when calculating ORs or HRs (aOR; aHR). It is possible that these adjustments are complex and vary widely across these studies, further contributing to heterogeneity. Additionally, the majority of studies are observational in nature limiting causal inference and necessitating further research, including prospective cohort studies and mechanistic investigations. This study only relied on the PubMed database for the identification of potentially eligible studies. Our risk of bias assessment (NOS) was able to evaluate the majority but not all studies assessed in this review.
Other limitations revolved around how we defined environmental exposure and aerodigestive disease as a whole. Our study defined environmental exposures as air pollution in the form of particulate matter, cigarette/tobacco smoke, marijuana smoke, vape/e-cigarette aerosols. Due to this, it was not possible to completely cover the entire scope of environmental exposures that afflict society. In addition, our definition of aerodigestive disease focused on diseases of the upper gastrointestinal tract, which comprised of esophagitis, Barrett’s esophagus, GERD, PUD, and esophageal/gastric cancer based on the articles we found. It is very likely that there are other aerodigestive diseases that interact strongly with environmental exposures that were not covered by this paper. Due to these definitions and our inclusion/exclusion criteria, we also found no eligible articles that investigated the interactions of marijuana smoke and vape/e-cigarette aerosols with aerodigestive disease.
Future Research
Currently, there are no human studies available to clearly define the cancer-inducing potential of non-burning nicotine delivery products such as e-cigarettes. However, this could be due to the very extensive lag time between carcinogen exposure and clinical cancer diagnosis in humans. Future studies could expand our definitions to account for interactions not present within this review, such as those of marijuana smoking, vaping, and those of the lower intestinal tract. Additionally, future studies could assess the contribution of specific occupational exposures to aerodigestive health, as this study only focused on exposures commonly experienced by the general population. Such additional exposures include asbestos, synthetic fiber dust, chrysotile dust, nephrite, and potentially harmful elements (PHEs) which are all commonly present in mining or textile industries and in developing societies in general. Such investigations could yield valuable insights for those whose occupation or geographic location puts them at risk for such diseases, as aerodigestive disease is often not recognized for those working/living under such conditions. In addition, this could identify how specific exposures incite disease in various cohorts.
Conclusion
The implications of these findings are significant from both a public health and clinical perspective. Efforts to reduce exposure to environmental pollutants, such as particular matter, could potentially mitigate the burden of upper gastrointestinal diseases in affected populations. Similarly, targeted interventions aimed at reducing smoking behavior and promoting smoking cessation may help reduce the incidence of BE and malignancy. Furthermore, continued research into the potential health effects of emerging trends, such as vaping and marijuana use, is crucial for informing preventive strategies and improving patient outcomes.
This review provides support for the connection between environmental exposures and digestive health, which is especially important considering that those who have been exposed to environmental/occupational inhalants are generally not covered for their digestive health. We hope that this review will promote further recognition of treatment of digestive disease with inhalational exposure.
In conclusion, this systematic review contributes to our understanding of the interplay between exposure to inhalational exposures and diseases of the upper gastrointestinal tract. By synthesizing existing evidence and identifying knowledge gaps, this study highlights the need for approaches to address environmental risk factors and promote gastrointestinal health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Exposure Science, Available online: https://www.niehs.nih.gov/health/topics/science/exposure. (Accessed on 22 November 2022).
- 2Air Pollution, Available online: https://www.who.int/health-topics/air-pollution#tab=tab_1. (Accessed on 22 November 2022).
- 3Orru H., Ebi K. L. & Forsberg B. The Interplay of Climate Change and Air Pollution on Health. Curr Environ Health Rep 2017, 4, 504–513, doi:10.1007/s 40572-017-0168-6.29080073 PMC 5676805 · doi ↗ · pubmed ↗
- 4Shaddick G., Thomas M. L., Mudu P., Ruggeri G. & Gumy S. Half the world’s population are exposed to increasing air pollution. npj Climate and Atmospheric Science 2020, 3, 23, doi:10.1038/s 41612-020-0124-2. · doi ↗
- 5Landrigan P. J., Sly J. L., Ruchirawat M., Silva E. R., Huo X., Diaz-Barriga F., Zar H. J., King M., Ha E. H., Asante K. A., Ahanchian H. & Sly P. D. Health Consequences of Environmental Exposures: Changing Global Patterns of Exposure and Disease. Ann Glob Health 2016, 82,10–19, doi:10.1016/j.aogh.2016.01.005.27325064 · doi ↗ · pubmed ↗
- 6Peters A., Dockery D. W., Muller J. E. & Mittleman M. A. Increased particulate air pollution and the triggering of myocardial infarction. Circulation 2001, 103, 2810–2815.11401937 10.1161/01.cir.103.23.2810 · doi ↗ · pubmed ↗
- 7Peters A., von Klot S., Heier M., Trentinaglia I., Hormann A., Wichmann H. E. & Lowel H. Exposure to traffic and the onset of myocardial infarction. The New England journal of medicine 2004,351,1721–1730.15496621 10.1056/NEJ Moa 040203 · doi ↗ · pubmed ↗
- 8Wellenius G. A., Schwartz J. & Mittleman M. A. Air pollution and hospital admissions for ischemic and hemorrhagic stroke among medicare beneficiaries. Stroke; a journal of cerebral circulation 2005,36, 2549–2553.10.1161/01.STR.0000189687.78760.4716254223 · doi ↗ · pubmed ↗