A Woman with Right Shoulder Pain
Kitan Akinosho, William Weber

TL;DR
An 89-year-old woman with a rare shoulder dislocation and fracture was successfully treated through staged orthopedic procedures.
Contribution
This case report presents a rare inferior shoulder dislocation with a concomitant humeral neck fracture and its management in an elderly patient.
Findings
The patient had an inferior shoulder dislocation (luxatio erecta) with a humeral neck fracture.
A staged reduction approach was used due to the patient's age and osteoporosis.
Successful repair was achieved via arthroplasty within two weeks.
Abstract
We report a case of an 89-year-old female who presented with pain in her right shoulder following a fall onto her outstretched hand. Upon presentation, her right hand was held behind her head and elbow held above her head in flexion. There was obvious deformity seen and felt in her axilla. Radiograph of the shoulder showed an inferior shoulder dislocation and impacted humeral neck fracture. Given her age and comorbid osteoporosis, a bedside reduction was performed by orthopedics where the humeral head was intentionally dislocated from the humeral shaft. Thirteen days after the initial shoulder dislocation, the patient’s shoulder was successfully repaired by open reduction. Luxatio erecta, which means “erect dislocation” in Latin, refers to an inferior shoulder dislocation. It accounts for less than 1% of shoulder dislocations. Our case report highlights an inferior shoulder dislocation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
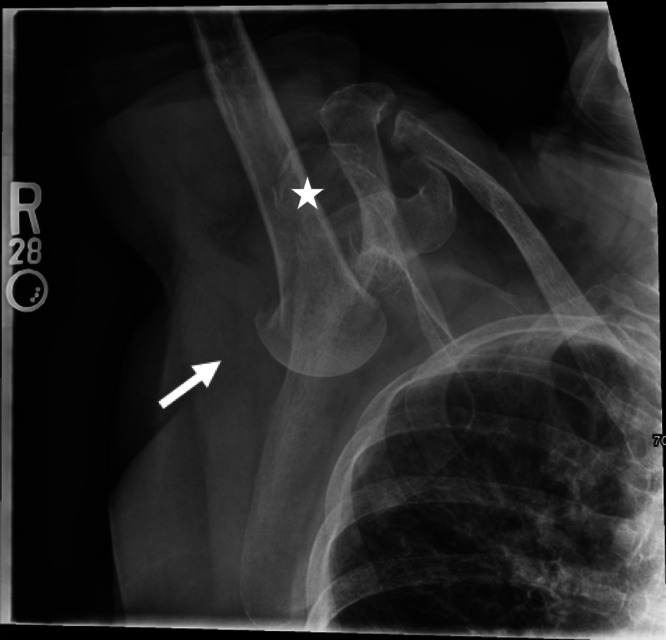 Image 1
Image 1 Image 2
Image 2 Image 3
Image 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder and Clavicle Injuries · Shoulder Injury and Treatment · Trauma Management and Diagnosis
CASE PRESENTATION
An 89-year-old female with a history of osteoporosis presented after a mechanical fall with right shoulder pain. She tripped and fell with her arm raised above her head and in front of her. She reported difficulty moving her right arm from its position above her head. On physical exam, her right arm was neurovascularly intact, but held above her head with palpable inferior displacement of the humeral head in the axilla. Radiograph was performed and is shown below (Image 1).
Initial radiograph of right shoulder shows a right inferior dislocation [luxatio erecta] with a concomitant impacted humeral neck fracture (arrow). A mildly displaced right glenoid fracture is also noted (star).
DISCUSSION
This radiograph shows an inferior shoulder dislocation, also known as luxatio erecta, an uncommon shoulder injury that accounts for less than 1% of shoulder dislocations.1 Luxatio erecta typically results from sudden hyperabduction, which forces the humeral head inferiorly, often tearing the inferior capsule. Patients generally present with the arm fully abducted and their hand near their head for comfort.2 Patients most commonly fracture the greater tuberosity, but this patient with osteoporosis experienced a humeral neck fracture.
Two important approach considerations differentiate inferior shoulder dislocations from typical anterior or posterior dislocations: rate of concomitant injury and vector of reduction. Physicians should pay close attention for neurovascular compromise, with the axillary nerve and axillary artery very susceptible to injury. Studies have found high rates of bony injury (60%), neurologic injury (29%), and vascular injury (10%) associated with the injury.1 ^,^ 3 Reductions for inferior shoulder dislocations typically employ superior and external traction.4 Alternatively, anterior traction can convert an inferior dislocation to an anterior dislocation, which can then be reduced with a variety of methods.
In this case, orthopedics was consulted due to the multiple concomitant fractures. Typically, the remainder of the humerus can be used to distract the humeral head and allow reduction, but in this case the humeral head was separated. In this case, orthopedics chose to use traction-countertraction with a superior and external vector away from the patient to reduce the remainder of the humerus for comfort and neurovascular safety while leaving the humeral head dislocated for open repair (Image 2). The patient was provided a shoulder sling in the interim until cardiac risk evaluation cleared her for operative repair (Image 3). The patient experienced no long-term neurologic compromise from her injury.
Radiograph of right shoulder immediately post-reduction showing humeral fracture (arrow).
Radiograph of right shoulder 13 days post-dislocation following outpatient, right reverse total shoulder arthroplasty.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nambiar M Owen D Moore P et al . Traumatic inferior shoulder dislocation: a review of management and outcome. Eur J Trauma Emerg Surg. 2018;44(1):45–51.28975397 10.1007/s 00068-017-0854-y · doi ↗ · pubmed ↗
- 2Vasiliadis AV Kalitsis C Kantas T et al . Inferior dislocation of shoulder complicated with undisplaced greater tuberosity fracture, rupture of the supraspinatus tendon, and brachial plexus injury in the elderly: case report and literature review. Case Rep Orthop. 2020;2020:9420184.32566341 10.1155/2020/9420184 PMC 7285250 · doi ↗ · pubmed ↗
- 3Ostermann RC Joestl J Hofbauer M et al . Associated pathologies following luxatio erecta humeri: a retrospective analysis of 38 cases. J Clin Med Res. 2022;11(2):453.10.3390/jcm 11020453 PMC 877950235054147 · doi ↗ · pubmed ↗
- 4Nho SJ Dodson CC Bardzik KF et al . The two-step maneuver for closed reduction of inferior glenohumeral dislocation (luxatio erecta to anterior dislocation to reduction). J Orthop Trauma. 2006;20(5):354–7.16766940 10.1097/00005131-200605000-00010 · doi ↗ · pubmed ↗