Atrial Fibrillation Occurring After Smoking Marijuana: A Case Report and Review of the Literature
Mary Unanyan, Christopher Colbert, Wesley Eilbert

TL;DR
A young woman developed atrial fibrillation after smoking marijuana, with no other known risk factors, suggesting a possible link between cannabis use and heart rhythm issues.
Contribution
This case report highlights a potential causal relationship between marijuana use and new-onset atrial fibrillation in young, otherwise healthy individuals.
Findings
A 38-year-old woman with no significant medical history developed atrial fibrillation after smoking marijuana.
No other cardiac or metabolic conditions were identified to explain the atrial fibrillation.
The atrial fibrillation resolved within three hours without treatment.
Abstract
Atrial fibrillation (AF) is the most common cardiac arrhythmia, occurring primarily in individuals with known risk factors such as advanced age, heart failure, and coronary artery disease. Cannabis use produces several cardiovascular changes resulting in proarrhythmic effects on the heart. A 38-year-old woman with no significant past medical history presented to the emergency department (ED) complaining of palpitations with associated shortness of breath occurring after smoking marijuana. She was found to be in AF. Evaluation in the ED and during hospitalization found no cardiac or metabolic conditions that predisposed to AF. The AF resolved within three hours of onset without intervention. Cannabis use should be considered as a possible etiology of new-onset AF, especially in relatively young patients with no other predisposing risk factors.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Image
Image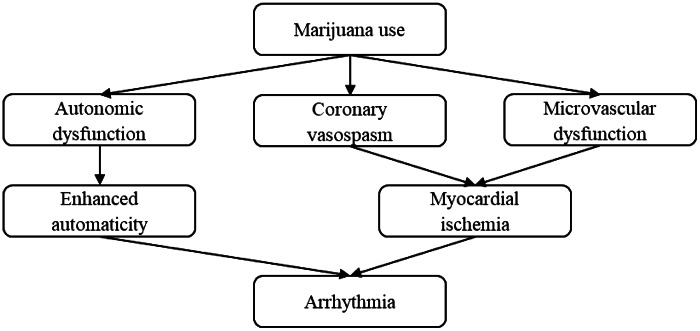 Figure
Figure| Supraventricular arrhythmias | Ventricular arrhythmias |
|---|---|
| Atrial fibrillation | Ventricular tachycardia |
| Atrial flutter | Ventricular fibrillation |
| Ectopic atrial tachycardia | Asystole |
| Supraventricular tachycardia | |
| Junctional rhythm | |
| Sinus bradycardia | |
| Sinus arrest | |
| First degree AV block | |
| Second degree AV block | |
| Third degree AV block |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCannabis and Cannabinoid Research · Substance Abuse Treatment and Outcomes · Smoking Behavior and Cessation
INTRODUCTION
Atrial fibrillation (AF) is the most common cardiac arrhythmia, occurring in 1–3% of the general population and in up to 17% of individuals >80 years in age.1 The majority of AF cases occur in patients with known risk factors such as advanced age, heart failure, and coronary artery disease.1 We report a case of paroxysmal AF in a 38-year-old woman with no associated risk factors after smoking marijuana.
CASE REPORT
A 38-year-old woman with a history of obesity presented to the emergency department (ED) complaining of palpitations with associated shortness of breath, dizziness, and chest discomfort. The symptoms had begun abruptly approximately one hour earlier while she was a patient in a nearby dental clinic. She admitted to recreational marijuana use and reported she had smoked marijuana just prior to her dental appointment to alleviate her related anxiety.
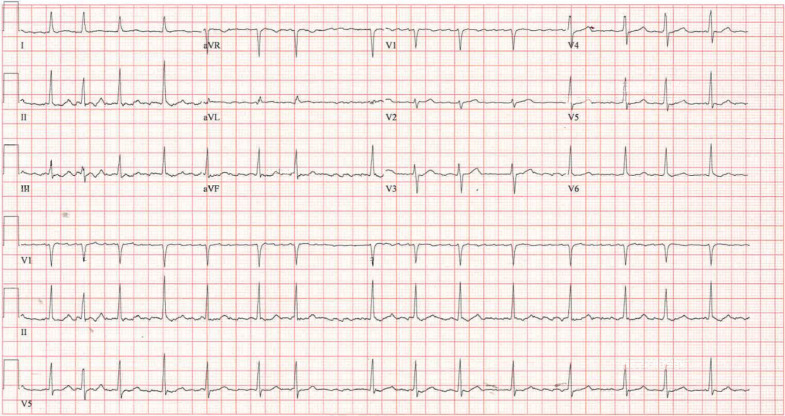
On physical examination, she had a pulse of 93 beats per minute with an irregular rhythm, and her blood pressure was 123/90 millimeters of mercury. Her lungs were clear to auscultation. An electrocardiogram revealed an irregular rhythm with a narrow QRS complex and an absence of P waves, consistent with AF (Image). No ischemic changes were present.
The patient’s electrocardiogram showing atrial fibrillation.
Laboratory testing in the ED was remarkable for a minimally elevated serum high-sensitivity troponin I level of 15 nanograms per liter (ng/L) (reference range: 0–15 ng/L) and a serum thyroid stimulating hormone level in the normal range. Approximately 90 minutes after ED arrival, the patient spontaneously converted to a normal sinus rhythm. She was admitted to the hospital for evaluation of new-onset AF.
The patient remained in a sinus rhythm while in the hospital. Serial serum high-sensitivity troponin I levels were not indicative of myocardial damage. Her serum magnesium level was found to be just below the normal range at 1.7 milligrams per deciliter (mg/dL) (1.8–2.4 mg/dL). Her urine toxicological screening was positive only for cannabinoids. Her transthoracic echo revealed no structural abnormalities of the heart and normal left ventricular function. The patient was discharged home on hospital day two on no new medications as her AF was felt to be paroxysmal in nature.
DISCUSSION
Cannabis is the most widely used illicit drug in the United States (US).2 The percentage of US adults that use marijuana has more than doubled since 2001, and cannabis in various forms for recreational or medicinal use is now legal in 46 states.3 ^,^ 4 The potency of cannabis has also increased significantly in the past 20 years in the US.5 As of 2021, approximately 75% of US adults believed cannabis use was as safe or safer than tobacco use.6
Paroxysmal AF following marijuana use was first reported in 2000.7 Since then, several similar cases have been described, often in young people with structurally normal hearts and no other risk factors for AF.8 It is possible that AF after marijuana use is under-reported because patients are reluctant to seek medical care while under the influence of the drug due to legal concerns. Also, palpitations suggestive of AF experienced by users may be interpreted as simply an expected cardiovascular effect of cannabis use. Atrial fibrillation following use of synthetic cannabinoids has also been described.9
Various cardiac arrhythmias have been reported with marijuana use, with AF and ventricular fibrillation the most common (Table).10 ^–^ 12 The mechanisms by which marijuana induces cardiac arrhythmias is unknown, although several mechanisms have been proposed (Figure).8 ^–^ 10 Autonomic dysfunction begins within minutes after smoking marijuana, causing a biphasic and dose-dependent effect. Sympathetic stimulation is predominant at lower doses, leading to tachycardia and enhanced cardiac automaticity. At higher doses, parasympathetic activation leads to bradycardia and hypotension.8 ^,^ 13 Cannabis may also induce coronary vasospasm and have a detrimental effect on the coronary microcirculation, leading to myocardial ischemia.8 ^,^ 10 All of these cardiovascular changes result in proarrhythmic effects on the heart.
Proposed mechanisms of marijuana-induced cardiac arrhythmias.
The incidence of AF related to marijuana use is difficult to estimate, although the prevalence of cannabis use disorder among patients admitted for AF is increasing, with the greatest increase in percentage prevalence among younger patients.14 Atrial fibrillation related to marijuana use at this point seems to be a transient and relatively benign phenomena, leading some authors to compare it to “holiday heart” occurring with ethanol use.15 Screening for cannabis use by history or laboratory testing should be considered in patients with new-onset AF, especially in those otherwise young and healthy.
CONCLUSION
Atrial fibrillation associated with marijuana use has been increasingly described in the past 20 years. The exact mechanism by which marijuana induces AF is unknown. This phenomenon is typically transient and relatively benign in patients that are otherwise young and healthy. Cannabis use should be considered as a possible etiology of new onset AF, especially in young patients with no other predisposing risk factors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Freedman B Hindricks G Banerjee A et al . World Federation Roadmap on Atrial Fibrillation - a 2020 update. Glob Heart. 2021;16(1):41.34211827 10.5334/gh.1023 PMC 8162289 · doi ↗ · pubmed ↗
- 2Centers for Disease Control and Prevention . Marijuana and Public Health. 2021. Available at: https://www.cdc.gov/marijuana/data-statistics.htm. Accessed December 28, 2023.
- 3Hasin DS Saha TD Kerridge BT et al . Prevalence of marijuana use disorders in the United States between 2001–2002 and 2012–2013. JAMA Psychiatry. 2015;72(12):1235–42.26502112 10.1001/jamapsychiatry.2015.1858 PMC 5037576 · doi ↗ · pubmed ↗
- 4DISA Global Solutions . Marijuana legality by state. 2023. Available at: www.disa.com/marijuana-legality-by-state. Accessed December 29, 2023.
- 5Chen M Lu YL Chen XF et al . Association of cannabis use disorder with cardiovascular diseases: a two-sample Mendelian randomization study. Front Cardiovasc Med. 2022;9:966707.36277767 10.3389/fcvm.2022.966707 PMC 9582269 · doi ↗ · pubmed ↗
- 6Chambers J Kehani S Ling PM et al . Perceptions of daily cannabis vs tobacco smoking and secondhand smoke exposure, 2017–2021. JAMA Netw Open. 2023;6(8):e 2328691.37566411 10.1001/jamanetworkopen.2023.28691 PMC 10422186 · doi ↗ · pubmed ↗
- 7Kosior DA Filipiak KJ Solarz P et al . Paroxysmal atrial fibrillation in a young healthy female patient following marijuana intoxication-a case report a possible association. Med Sci Monit. 2000;6(2):386–9.11208344 · pubmed ↗
- 8Korantzopoulos P Liu T Papaioannides D et al . Atrial fibrillation and marijuana smoking. Int J Clin Prac. 2008;62(2):308–13.10.1111/j.1742-1241.2007.01505.x 18031530 · doi ↗ · pubmed ↗