Outcomes of a hydroxyapatite ceramic-coated femoral stem in primary total hip arthroplasty: a report of excellent survivorship from a single United Kingdom centre
Karim M. Abdelghafour, Sherif A. Khaled, Khaled F. M. Abdel-Kader, Hazem A. Azeem, Nirav N. Shah

TL;DR
A study found that a hydroxyapatite ceramic-coated femoral stem used in hip replacements had excellent long-term survival and full integration with bone in patients.
Contribution
The study provides long-term clinical and radiological evidence of excellent survivorship and osseointegration of a specific hydroxyapatite ceramic-coated femoral stem in primary total hip arthroplasty.
Findings
The HAC-coated femoral stem had a 100% survival rate at 14 years with aseptic loosening as the endpoint.
Radiological assessments showed full osseointegration of all stems.
Patient-reported outcome scores indicated good functional outcomes.
Abstract
Background: Hydroxyapatite (HA) coated femoral stems were introduced to enhance the biological fixation at the implant-bone interface, aiming to increase the longevity and survival of the prostheses. We aimed to assess the long-term outcomes of an HA ceramic (HAC) coated stem in primary total hip arthroplasty (THA), assess the stem survival, and clinically evaluate the patients using patient-reported outcome measures (PROMs) and radiological evaluation of stem osseointegration. Patients and methods: This was a prospective evaluation of a retrospective cohort of 385 patients (442 hips) who underwent primary THA between June 2008 and December 2018. The mean age was 63.83 years (range, 30–82 years). During the follow-up duration, 23 patients died, and 36 patients (38 hips) were lost to follow-up. Prospective data collected for 326 patients (381 hips) was used to evaluate stem survival with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 1
Figure 1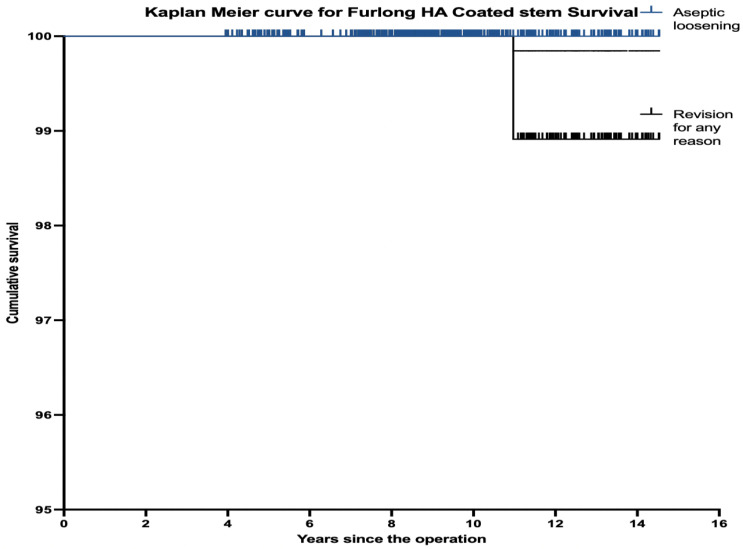 Figure 2
Figure 2 Figure 2
Figure 2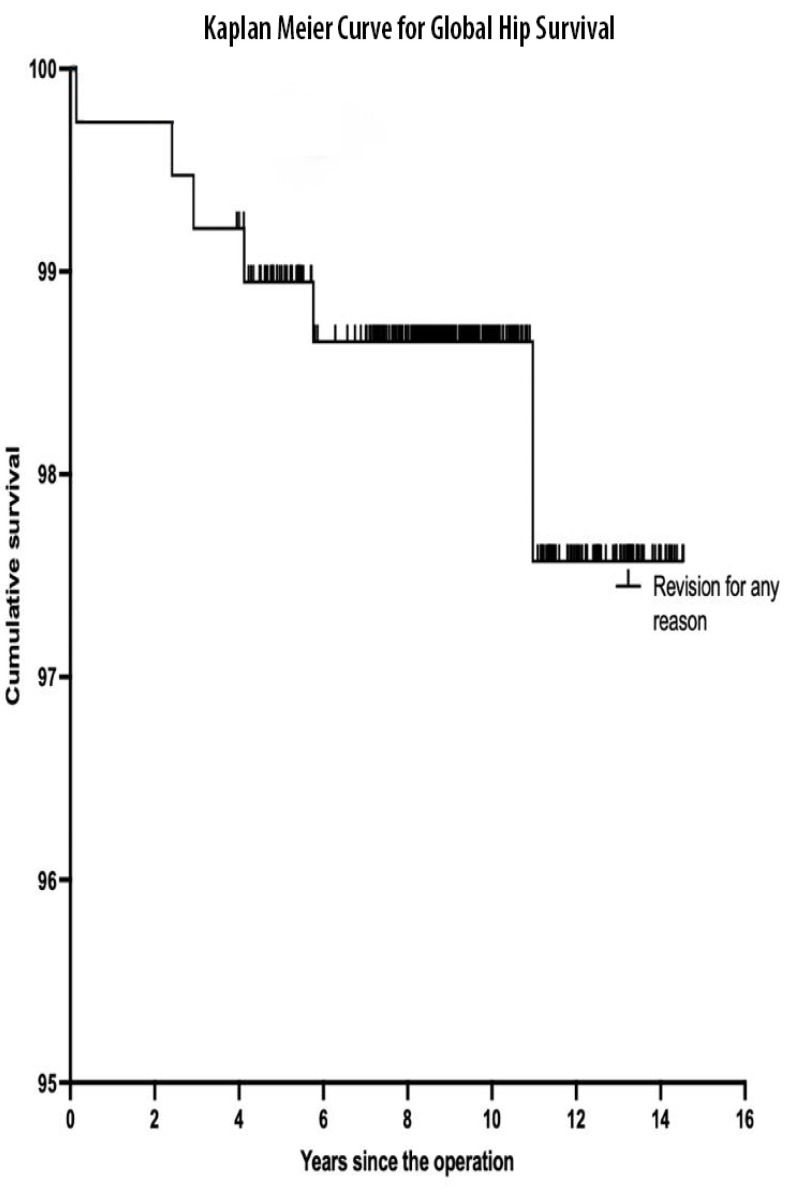 Figure 3
Figure 3 Figure 3
Figure 3 Figure 4
Figure 4 Figure 4
Figure 4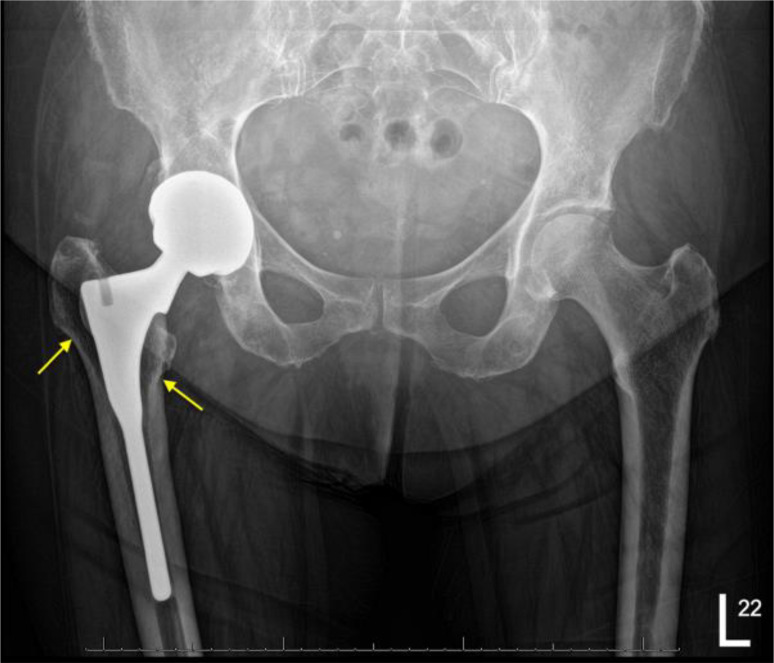 Figure 5
Figure 5 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopaedic implants and arthroplasty · Total Knee Arthroplasty Outcomes · Orthopedic Infections and Treatments
Introduction
The dramatic pain relief and restoration of function achieved by total hip arthroplasty (THA) make the procedure life-changing for patients with degenerative hip disease, owing to the impact on the patient’s quality of life. However, THA can carry a risk of complications such as loosening, wear, periprosthetic fractures, and dislocation [1, 2]. With the increasing life expectancy among the population and younger patients requiring THA, there is an increased use of uncemented prostheses for THA. The longevity of the femoral stem used in THA has become crucial to ensure excellent outcomes and patient satisfaction [3, 4].
Hydroxyapatite (HA) coatings were introduced to enhance the biological fixation of hip prostheses owing to the osteoconductive and osteoinductive properties [5]. HA promotes bone growth at the implant-bone interface without intervening fibrous tissue formation. Another key characteristic of HA is crystallinity, which is associated with increased bioactivity, bone growth, and decreased bone resorption [6].
The Furlong hydroxyapatite ceramic (HAC) femoral stem (JRI Orthopaedics Ltd, London, UK) was the first-ever HAC stem used in THA in 1985. It is manufactured from a titanium alloy (Ti-6Al-4V), with its surface plasma-sprayed with a 200-μm thick layer of HA with high crystallinity. The stem is collared and designed to achieve primary stability by proximal metaphyseal fit (Figure 1), and the rectangular cross-section of the proximal body provides rotational stability under dynamic loading. The cone-shaped geometric transition between the proximal body and cylindrical distal stem is intended to discourage subsidence [7].
Figure 1. Furlong HAC stem design.
We aimed to assess the long-term results of this HAC-coated femoral stem in primary THA. We assessed the survival of the stem at 14 years by using aseptic loosening or any revision as the endpoint, with clinical evaluation and radiological evaluation of the osseointegration of the stem.
Patients and methods
Between June 2008 and December 2018, a cohort of 385 patients (442 hips) had THA performed using the Furlong HAC-coated femoral stem. Evaluation of data for this retrospective series was done. We included all patients who had primary THA during this period with at least 4 years of follow-up. Patients who lacked the mental capacity, revision arthroplasty cases, and patients with <4 years of follow-up were excluded.
Surgical technique
The surgical procedure was standardised, and all procedures were performed by or under the direct supervision of a single surgeon via a posterior approach to the hip with the patient in the lateral position. The CSF Plus HAC-coated cup (JRI Ltd, London, UK) was used in all cases. A modular 36 mm fourth-generation ceramic head (Biolox Delta) was used in all hips on a ceramic liner.
Prophylactic antibiotics were administered according to the local guidelines. Venous thromboprophylaxis in the form of low molecular weight heparin was given postoperatively. Patients were allowed full weight bearing postoperatively, and all patients had physiotherapy before discharge.
Clinical and radiological evaluation
Follow-ups were performed at 6 weeks, 12 weeks, 6 months and 12 months postoperatively, and 5 years. During the Coronavirus disease 2019 pandemic, some follow-ups were done using telephone consultations to avoid patient exposure to infection risk. Patients who were unable to attend follow-ups completed postal questionnaires.
Patient-reported outcome measures (PROMs) were collected, and clinical assessments of pain, mobility, and function were performed using the Merle d’Aubigné and Postel (MDP) scoring system and Oxford Hip Score (OHS) assessing pain and functional ability from the patient’s perspective [8]. We assessed health-related quality of life using the EuroQol-5D visual analogue score, which ranges from 0 to 100 [9]. We assessed the presence of anterior thigh pain, any dislocation events, or periprosthetic fractures. The incidence of infection, thromboembolic complications, and any bearing-related complications were also recorded.
Radiological evaluation was carried out by two independent reviewers to provide inter-observer reliability. Gruen zones for the femur and DeLee and Charnley zones for the acetabulum were used for the assessment of any migration, subsidence, and stress shielding. Stability and osseointegration were assessed using the Engh radiological criteria for uncemented stems [10]. Heterotopic ossification (HO) was identified and graded according to Brooker classification [11].
Data analyses were performed using the Statistical Package for Social Sciences (SPSS) version 28.0 (SPSS Inc., Chicago, Illinois). Cumulative survival analysis using the Kaplan–Meier method was done with corresponding 95% confidence intervals. The endpoint was the revision of the femoral component for any reason or aseptic loosening, and the date of the latest follow-up was defined as a censored event. A P-value ≤0.05 was considered statistically significant.
Results
From 385 patients (442 hips) who met the inclusion criteria, 23 patients (23 hips) died from causes unrelated to the THA. By tracking those patients’ general practitioner records, none of the patients reported any clinical problems with their hips within 1 year of their death. In total, 33 patients (38 hips) were excluded because of cognitive impairment, dementia, or being lost to follow-up. The number of patients who participated in the study was 326 patients, of which 55 had bilateral THAs, and the number of hips available for final follow-up was 381 hips.
The mean follow-up duration was 9.39 years (range, 4–14.5 years). The mean age at the time of the procedure was 63.83 years (range, 30–82 years). Surgical indications and patient demographics are detailed in Table 1.
Table 1. Patient demographics.Characteristic n Patients, n326THA, n381Sex Women, n (%)174 (53.4) Men, n (%)152Mean age, years (range)63.83 (30–82)Mean follow-up duration, years (range)9.39 (4–14.5)BMI, kg/m^2^ (range)27.73 (16.5–49)Indication for THA, n (%) OA314 (82.6) AVN24 (6.2) Dysplasia26 (6.8) Rheumatoid arthritis12 (3.1) Trauma4 (1) Ankylosing spondylitis1 (0.3)THA, total hip arthroplasty; BMI, body mass index; OA, osteoarthritis; AVN, avascular necrosis.
Clinical evaluation and stem survival
The mean visual analogue score (VAS) of the EuroQol-5D was 83.46 (range, 40–100), with 348 (91.3%) hips having a score ≥70. The mean MDP score for the 381 hips was 15.87 (range, 10–18). The mean OHS was 44.5 (range, 30–48), with improvement compared to the mean pre-operative OHS, which was 19.31 (P = 0.02). We found a correlation between the OHS and comorbidities affecting mobility, such as spinal pathology, stroke, or adjacent joint arthritis. There were 25 patients with an OHS < 39; 16 of them (64%) had these comorbidities. For the patients with an OHS ≥39, 89% did not have these comorbidities with a statistically significant difference (P = 0.018).
The cumulative survival for the HAC-coated femoral stem was 100% (95% CI, 96.7–100%) with aseptic loosening used as the endpoint, and 98.9% (95% CI, 96.7–100%) with revision for any reason as the endpoint (Figure 2). The survival for the whole THA was 97.6% (95% CI, 95.2–100%) with a mean follow-up duration of 9.39 years using any revision as an endpoint (Figure 3).
Figure 2. Kaplan–Meier survival curve for HA-coated stem survival.
Figure 3. Kaplan–Meier curve for whole THA survival.
Radiological evaluation
Radiological evaluation was done for 301 patients (356 hips) who were able to attend for radiographs at the final follow-up*,* with a mean Engh score of 18.425 (range, 7–27), revealing osseointegration of all stems (Figure 4). Two hips (0.5%) showed subsidence of 3 mm within 1 year postoperatively, but subsequent serial radiographs showed no further subsidence, with radiological evidence of complete osseointegration. There were 17 stems (4.4%) that showed some bone remodelling in the form of stress shielding, particularly at Gruen zones 1, 2, and 7. None of these patients complained of any pain, and by following their radiographs, there were no signs of stem migration (Figure 5).
Figure 4. Pelvis anterior-posterior radiographs 12 years postoperatively with evidence of full osteointegration of the stems with spot welds.
Figure 5A 10-year post-operative radiograph with lucency at Gruen zones 1 and 7 (arrows) with no clinical signs or pain reported.
Complications and secondary surgeries
In total, seven patients required revision arthroplasty, one patient underwent stem revision due to deep prosthetic joint infection (PJI), and six patients required acetabular revisions. Among the acetabular revisions, one was performed for PJI, two due to failure of osseointegration, two cups were revised due to malpositioning, and one cup was revised following a periprosthetic acetabular fracture. Other complications included two cases that required abductor repair for abductor dysfunction, two cases that developed early post-operative infection treated by washout and implant retention, and one patient that required open reduction and internal fixation for periprosthetic fracture Vancouver type B1. There were eight intra-operative fractures (2%) (seven calcar splits and one greater trochanter fracture) that required cabling or cerclage wires, and none of the cases required the use of revision implants instead of the planned HAC-coated stem. Two cases experienced Vancouver AG periprosthetic fractures that were treated conservatively.
There were two dislocations (0.5%) in our study; one patient had dislocation 4 weeks postoperatively, and the hip was relocated with no instability issues afterwards, the second case required revision of the acetabular component. Seven cases (1.8%) had deep venous thrombosis (DVT), and two patients (0.5%) developed pulmonary embolism (PE); all were treated with anticoagulation and none of the cases had mortality. Despite the radiological findings of HO in 139 hips, the patients who complained of stiffness from the HO were 10 (2.6%), with two patients only requiring surgical excision of the HO. Four cases (1%) complained of iliopsoas impingement, 13 patients (3.4%) were diagnosed with trochanteric bursitis for lateral hip pain, and two (0.5%) patients complained about thigh pain (Table 2).
Table 2. Incidence of complications in the study.ComplicationNumber%Revision arthroplasty71.8Infection30.8Fractures: Femoral/acetabular(intra-operative/periprosthetic)123.1Dislocation20.5Subsidence20.5Heterotopic ossification102.6DVT/PE92.3Iliopsoas impingement41Lateral hip pain (trochanteric bursitis)133.4Thigh pain20.5DVT/PE, deep vein thrombosis/pulmonary embolism.
Discussion
Our study showed excellent survival rates for this HAC-coated femoral stem with a mean follow-up duration of 9.39 years, with 100% survival with aseptic loosening as the endpoint and 98.9% with stem revision due to any reason. These findings are comparable with other studies assessing this HAC-coated stem [4, 12, 13]. To our knowledge, this is the largest study assessing the outcomes of this stem, wherein we unified the bearing system to limit the bias from using different bearing systems on the survival rates, and ceramic on ceramic bearings were used owing to the superior wear properties and lower wear and osteolysis rates than traditional bearing surfaces [14].
The survival results were comparable to other studies assessing different HA-coated stems [15–17]. The stem used in our study now has the highest Orthopaedics Device Evaluation Panel (ODEP) rating, which is 15A*. The ODEP was set up to evaluate the outcomes of arthroplasty prostheses and ensure compliance with the benchmarks set by the National Institute of Clinical Excellence (NICE) [18].
The clinical evaluation revealed significant improvement in the OHS and MDP scoring systems and improvement in the quality of life following the procedure. The results are comparable with other studies that used the same scoring systems [4, 12, 16] and other scoring systems for hip function [13, 15, 17]. The decline of OHS reported over the years by some patients may be explained by advancing age, medical problems, or mobility issues such as degeneration of the spine or other joints.
Our radiological evaluation revealed osseointegration of all femoral stems in our study. The radiolucent lines suggestive of stress shielding were non-progressive throughout the follow-up with no pain or limitation of function. Calcar atrophy caused by stress shielding in uncemented THA has shown slow progressive recovery over the years, without significant clinical relevance [19]. The low degree of proximal bone loss in our study indicates no significant net transfer of stress from proximal to distal, but rather a physiological weight distribution from the stem to the femoral bone after osseointegration.
There were eight (2%) intra-operative femoral fractures, all secured by a cerclage wire. The prevalence of intra-operative femoral fractures increases in advanced age groups, females, and conditions such as osteoporosis [20]. The risk is higher in uncemented stems and can be related to stem design, with one study showing a relation between the size of this HAC stem and the occurrence of intra-operative fractures. Furthermore, a systematic review showed a higher risk of fractures with uncemented prostheses, especially single and double-wedged tapered stems [21, 22]. There was no statistical significance in our study between the occurrence of intra-operative fractures and age or sex.
Our study had two (0.5%) dislocations, with one requiring revision for component malalignment. The fourth-generation ceramic head 36 mm was used in all cases, which may explain the low dislocation rate, due to the biomechanical advantages of the large head with increased range of motion and jumping distance [23]. The dislocation rates were lower than in other studies evaluating the same stem; this can be attributed to the use of different bearings and smaller head sizes in those studies [4, 13, 15]. The head diameter may not achieve stability alone; implant alignment and soft tissue tension are equally or even more important than head diameter [24].
Our patients were asked specifically about thigh pain; two patients (0.5%) reported thigh pain, describing it as intermittent, mild, and not interfering with their activities of daily living. Their radiographs showed no evidence of loosening or stress shielding. The low prevalence of thigh pain can be explained by the rapid osseointegration of the stem, the stem design that relies on metaphyseal fitting without the need for stem-fitting in the diaphysis, and the lower modulus of elasticity of the titanium implant [25].
We acknowledge some limitations in our study. First, the few pre-operative MDP scores for patient activity. However, there was an accurate record of scores from the time of surgery with a mean pre-operative and post-operative OHS. The VAS and PROM scores were consistently used as patient-reported tools to augment our clinical data. Second, there was a lack of reports on wear measurements. In long-term studies, wear measurements are vital to understanding the prognosis of the prosthesis.
In conclusion, our study had 100% survival with full osseointegration at the final follow-up, no stem failures due to aseptic loosening, and excellent PROMs at a mean follow-up of 9.39 years (range, 4–14.5 years). We assessed the hips with a unified bearing surface with the same femoral head size and the same acetabular component to avoid any variability in wear patterns and rates. Radiological evaluations showed complete osseointegration with minimal stress shielding.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Scott CH, Mac Donald DJ, Howie CR (2019) “Worse than death” and waiting for a joint arthroplasty. Bone Joint J 101, 941–950.31362549 10.1302/0301-620X.101B 8.BJJ-2019-0116.R 1PMC 6681678 · doi ↗ · pubmed ↗
- 2Johnsen SP, Sørensen HT, Lucht U, Søballe K, Overgaard S, Pedersen AB (2006) Patient-related predictors of implant failure after primary total hip replacement in the initial, short- and long-terms. A nationwide Danish follow-up study including 36,984 patients. J Bone Joint Surg Br 88, 1303–1308.17012418 10.1302/0301-620X.88B 10.17399 · doi ↗ · pubmed ↗
- 3Chandler HP, Reineck FT, Wixson RL, Mc Carthy JC (1981) Total hip replacement in patients younger than thirty years old: a five-year follow-up study. J Bone Joint Surg Am 63-A, 1426–1434.7320033 · pubmed ↗
- 4Syed MA, Hutt NJ, Shah N, Edge AJ (2015) Hydroxyapatite ceramic-coated femoral components in young patients followed up for 17 to 25 years: an update of a previous report. Bone Joint J 97-B, 749–754.26033053 10.1302/0301-620X.97B 6.35278 · doi ↗ · pubmed ↗
- 5Rahbek O, Overgaard S, Søballe K (2004) Calcium phosphate coatings for implant fixation. In: Fifteen years of clinical experience with hydroxyapatite coatings in joint arthroplasty,Springer, Paris, pp. 35–51. 10.1007/978-2-8178-0851-2_4. · doi ↗
- 6Overgaard S, Bromose U, Lind M, Bünger C, Søballe K (1999) The influence of crystallinity of the hydroxyapatite coating on the fixation of implants. J Bone Joint Surg Br 81-B, 725–731.10.1302/0301-620x.81b 4.928210463753 · doi ↗ · pubmed ↗
- 7Karia M, Logishetty K, Johal H, Edwards TC, Cobb JP (2023) 5 year follow up of a hydroxyapatite coated short stem femoral component for hip arthroplasty: a prospective multicentre study. Sci Rep 13, 17166.37821511 10.1038/s 41598-023-44191-7PMC 10567683 · doi ↗ · pubmed ↗
- 8Ahmad MA, Xypnitos FN, Giannoudis PV (2011) Measuring hip outcomes: common scales and checklists. Injury 42, 259–264.21163481 10.1016/j.injury.2010.11.052 · doi ↗ · pubmed ↗