Identification of causative fungus from sterile abscess using metagenomics followed by in situ hybridization
Hiroya Oki, Ryotaro Niwa, Somboonthum Pranee, Daisuke Motooka, Yoshiyuki Onda, Jun Nakata, Hiroko Nakajima, Yoshihiro Oka, Haruo Sugiyama, Yuka Yoshii, Naoyuki Anzai, Shota Nakamura, Tetsuya Iida

TL;DR
This paper describes using metagenomics and in situ hybridization to identify a fungus causing a sterile abscess when traditional methods failed.
Contribution
The study introduces a novel approach combining deep sequencing and in situ hybridization for fungal identification in sterile abscesses.
Findings
Deep sequencing of the ITS1 region narrowed down candidate fungi in a sterile abscess.
In situ hybridization confirmed the presence of Trichosporon asahii in the specimen.
The method successfully identified the causative fungus when blood culture and biopsy failed.
Abstract
Introduction. Invasive fungal infections require early diagnosis for treatment. Microscopic observation of biopsy and blood culture is the gold standard for the identification of the causative fungus, but it is difficult to identify the causative pathogen by a sterile abscess biopsy. Case Presentation. We present a case report of breakthrough invasive trichosporonosis in a 65-year-old Japanese male with acute myeloid leukaemia receiving antifungal prophylaxis. Blood cultures showed no fungal growth, and a liver biopsy and a removed spleen with abscess showed fragmented fungi, but no fungal identification was possible. This report demonstrates that retrospective analyses were able to identify the causative fungus. Conclusion. We narrowed down the candidate fungi by deep sequencing of the ITS1 region of fungal genome and confirmed that the fungus observed in the specimen was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
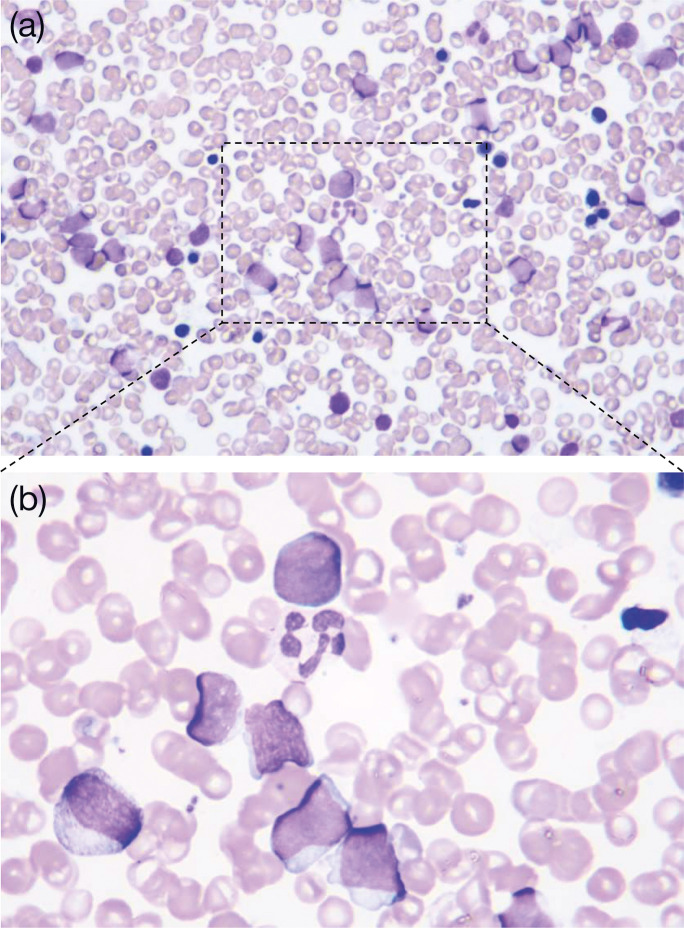 Fig. 1
Fig. 1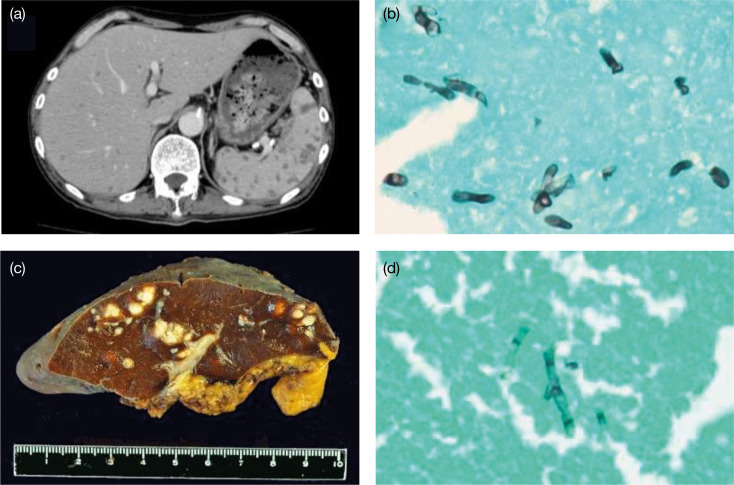 Fig. 2
Fig. 2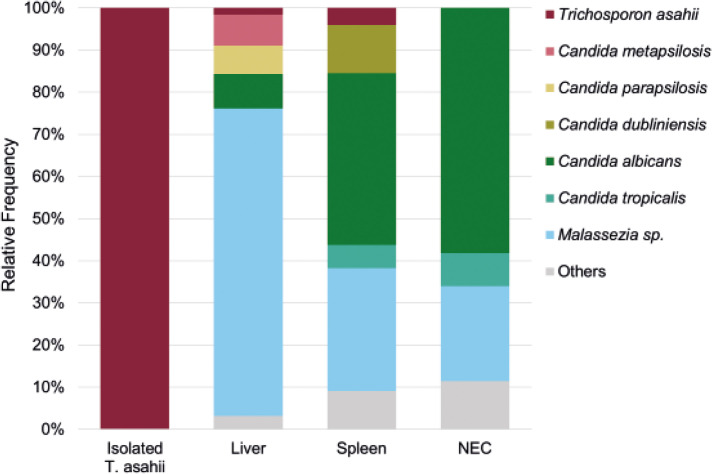 Fig. 3
Fig. 3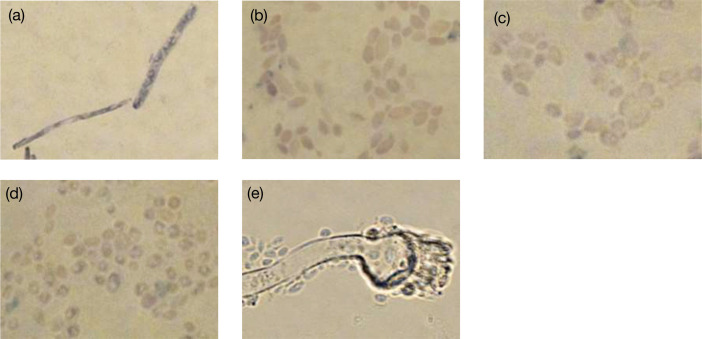 Fig. 4
Fig. 4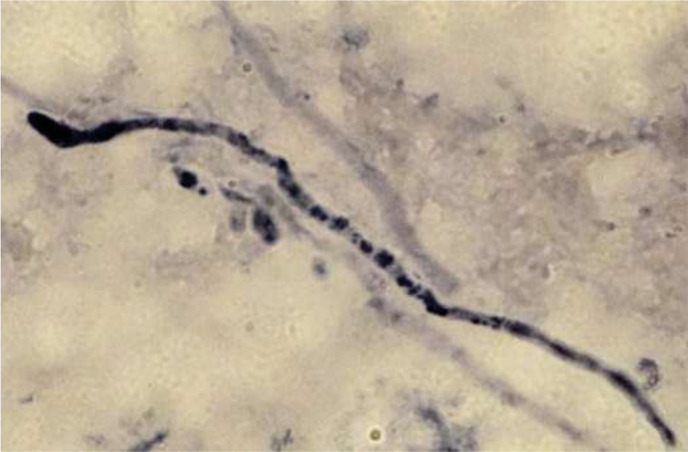 Fig. 5
Fig. 5| Antibiotics | MIC * |
| Amphotericin B | 2.0 |
| 5-Fluorocytosine | 2.0 |
| Fluconazole | 1.0 |
| Itraconazole | 0.12 |
| Miconazole | 0.12 |
| Micafungin | >16 |
| Voriconazole | 0.03 |
| Caspofungin | 8 |
- —JSPS
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Antifungal resistance and susceptibility · Mycobacterium research and diagnosis
Data Summary
The sequencing data were deposited at NCBI (accession number: PRJNA1054341).
Introduction
Abscess formation is sometimes observed in leukaemia patients with febrile neutropenia, and the identification of the causative micro-organism is essential for treatment and prophylaxis against recurrence in subsequent anti-leukaemia therapy. However, when the infection is active, invasive examinations cannot be performed due to severe neutropenia and thrombocytopenia. In most cases, as the infection becomes sterile during neutrophil recovery, an abscess biopsy fails to identify the causative micro-organism [1].
Most abscess-forming invasive fungal infections (IFIs) are caused by Candida or Aspergillus. However, in recent years, with the increasing use of immunosuppressive drugs, infections caused by rare opportunistic fungal pathogens, such as invasive trichosporonosis caused by Trichosporon asahii, are being reported [2]. The mortality rate of patients with deep trichosporonosis is higher than that of patients with IFIs caused by Candida or Aspergillus, at approximately 70 % [3]. As effective antifungal agents differ for each of these causative fungi, prompt identification of the fungus is essential for treatment. Direct observation of fungi in biopsies represents the gold standard for fungal identification [2]. However, due to the limited presence of fungi in biopsy tissue and their complex morphology, distinguishing them can be challenging [245]. While blood cultures are also frequently used, they are less sensitive, and causative fungi may not grow in cases where antifungal drugs are being administered [56]. Advances in molecular biology have introduced techniques such as polymerase chain reaction and sequence-based methods that target specific genes or regions [7]. However, these techniques are limited to the identification of some common pathogenic fungi, and appropriate detection methods for clinical practice have not yet been established for most rare fungi, including T. asahii [7].
The advent of next-generation sequencing (NGS) technology has brought a breakthrough in pathogen identification. NGS-based pathogen identification has led to rapid disease diagnosis, drug resistance profile analysis and identification of novel pathogens. In particular, metagenomic analysis allows for the comprehensive analysis of all DNA present in the genome, allowing for the simultaneous identification of multiple micro-organisms without relying on specific target genes or regions [89]. However, when culture amplifies the number of pathogens, alternative identification methods are employed, making the process less cost-effective. Moreover, biopsy specimens are often contaminated with non-pathogenic pathogens from the body and environmental contaminants (during the collection process), leading to the lack of standardized criteria for pathogen identification [810]. Here, we identified scenarios and methodologies in which NGS-based pathogen identification proves most beneficial in clinical applications.
Case presentation
The patient was a 65-year-old Japanese male with a history of grade 4 chronic kidney failure and benign prostate hyperplasia. He was introduced to our hospital due to neutropenia (white blood cell counts, 1300/µl) and anaemia (red blood cell counts, 334×10^4^/µl). Bone marrow examination revealed 50.5 % myeloblasts with granulocytic differentiation (Fig. 1a, b), and neither leukaemia-causing translocations nor leukaemia-causing gene mutations were detected. Additionally, the mRNA levels of Wilms’ tumour 1 gene, a leukaemia marker, were increased to 420 copies/μg of RNA. Therefore, he was diagnosed with acute myeloid leukaemia (AML) with maturation according to the fourth World Health Organization criteria [11]. The full form of the IA regimen (Idarubicin and cytarabine:AraC) consists of idarubicin 12 mg m^−2^ for 3 days and cytarabine 100 mg m^−2^ for 7 days; however, the dose of idarubicin was reduced to 8 mg m^−2^ for 3 days owing to renal dysfunction. This first induction chemotherapy showed no response. The full form of the MEtA regimen [12] comprises mitoxantrone 8 mg m^−2^ for 2–3 days and etoposide 50 mg/body and cytarabine 30 mg/body for 11–14 days; however, it was modified to mitoxantrone 5 mg m^−2^ for 2–3 days and etoposide 25 mg m^−2^ and cytarabine 15 mg m^−2^ for 10 days owing to renal dysfunction and to avoid severe neutropenia. This second induction therapy reduced myeloblast frequencies and the mRNA levels of Wilms’ tumour 1 gene from 53.3 to 7.8 % and from 230 to 69 copies/μg of RNA, respectively. Therefore, the repeated MEtA regimen was performed 60 days after the second induction chemotherapy, and subsequent hematopoietic stem cell transplantation was planned. However, febrile neutropenia occurred after the chemotherapy. Because the spike fever was not improved by meropenem and vancomycin, fungal infection was suspected. Voriconazole and liposomal amphotericin B were administered instead of oral itraconazole for prophylaxis, but the spike fever continued even after the recovery of neutrophils. Whole-body computed tomography revealed multiple low-density lesions, which were abscesses, in the liver and spleen (Fig. 2a) . To identify the causative micro-organisms, we repeatedly obtained blood cultures, but none revealed any pathogens. No skin lesions were detected throughout the clinical course. Since there have been some cases that show the efficacy of intra-aortic infusion of antifungal agents in patients with hepatosplenic abscesses when neither drainage nor resection of the organs are feasible [1314], we conducted a splenectomy to reduce the fungal load followed by intra-aortic infusion of micafungin 300 mg/day into the hepatic artery combined with oral itraconazole (200 mg). The patient finally defervesced, and the liver abscesses appeared to improve. Gross findings and Grocott staining of the spleen showed multiple fungal abscesses (Fig. 2c, d), which were similar to the findings from the liver biopsy, although they were never cultivated. Since the liver abscesses disappeared and mRNA levels of Wilms’ tumour 1 gene increased from below the detection level to 1600 copies/μg of RNA, suggesting the molecular relapse of AML, allogenic hematopoietic transplantation was performed with the prophylaxis of continued intravenous micafungin infusion. However, 6 days after the transplantation, a high fever occurred, and the patient subsequently died of multiorgan failure. The blood cultures confirmed the presence of fungemia of T. asahii, whose antifungal sensitivity profile showed resistance to micafungin (Table 1).
May–Grunwald–Giemsa stains of the patient’s bone marrow aspirate showing myeloblasts with granulocytic differentiation (a: ×80, b: ×20).
T. asahii infection in the patient with AML. (a) Contrast-enhanced computed tomography scan of hepatosplenic abscesses. (b) Liver biopsy stained using Grocott’s methenamine silver (GMS) showing the fungi. (c) Removed spleen showing abscesses. (d) Removed spleen stained using GMS showing fungi similar to those in the liver biopsy.
Even with repeated blood cultures, we were unable to grow the fungus. This could be attributed to the low numbers of fungi, which exhibited reduced biological activity, observed in the liver biopsy and spleen. Additionally, continuous administration of voriconazole and liposomal amphotericin B to the patient even during blood culture examination may have contributed to this outcome. In this study, we conducted a retrospective metagenomic analysis to determine whether the causative fungus T. asahii could be identified from biopsy specimens that were unsuitable for pathogen identification. DNA was extracted from fungi isolated from various sources, including blood cultures, residual liver biopsies (in storage) and excised spleens. We used distilled water as the negative extraction control (NEC). All of these NGS experiments were performed at the NGS Core Facility at Osaka University. Deep sequencing of the fungal ITS1 region was performed using each extracted sample. T. asahii was detected in all samples except the NEC (Fig. 3). However, more than 80 % of the reads obtained from liver biopsies and spleen specimens corresponded to Candida spp. and Malassezia sp. The inclusion of the NEC to the samples helped narrow down potential pathogenic fungi to three in the liver biopsies and two in the spleen. Of these, Candida spp. were detected only in the liver biopsy or spleen. In the present case, blood samples were always negative for Candida antigen; therefore, Candida spp. were excluded as candidate causative fungi. Notably, T. asahii was the only fungus detected in both the spleen and the liver biopsies but undetected in NEC. To confirm the presence of T. asahii in the observed fungi from the liver and spleen biopsies, we designed a biotinylated DNA probe to target the 26S rRNA sequence of T. asahii (5′-GTCTCCTGGAAAGGAGTAT-3′). The probe did not stain Candida spp. detected in the NGS experiments or Aspergillus sp., a common causative agent of IFIs, but specifically stained cultured T. asahii (Fig. 4). In situ hybridization experiments using the highly specific probe indicated that the fungus observed in the spleen was T. asahii. This definitive outcome confirmed the diagnosis of abscesses caused by T. asahii (Fig. 5).
Relative abundance of the fungal taxon in the T. asahii isolated from blood culture, liver biopsy, removed spleen and an NEC as a working control.
In situ hybridization of cultured fungi using a biotinylated DNA probe targeting the 26S rRNA sequence of T. asahii (5′-GTCTCCTGGAAAGGAGTAT-3′). (a) Trichosporon asahii (NBRC 103889). (b) Candida albicans (NBRC 1385). (c) Candida dubliniensis (NCPF 3949). (d) Candida parapsilosis (NBRC 0708). (e) Aspergillus terreus (NBRC 33026).
In situ hybridization of fungi in an abscess from the spleen using a biotinylated DNA probe targeting the 26S rRNA sequence of T. asahii (5′-GTCTCCTGGAAAGGAGTAT-3’).
Discussion
Metagenomic analysis has great potential for diagnosing infectious diseases because it can detect all potential pathogens with high sensitivity [8]. However, clinical specimens are often contaminated with endemic skin bacteria and fungi during sample collection, which often make up the majority of the data obtained, as was the case in this study [10]. In addition, contaminants ‘kitome’ in DNA extraction kits and DNA library preparation reagents can mask the DNA information of causative pathogens, which are present only in small quantities. To improve the identification accuracy of the causative pathogen, it is important to use negative controls for library preparation [15]. In this study, we were able to narrow down two and three candidates from the liver and spleen samples, respectively. In the present study, negative controls were prepared in the laboratory; however, samples obtained at earlier time points, such as those obtained in the operating room, could be used to further narrow down the candidates.
In this case, the infection of T. asahii was below detection levels by blood cultures and radiology before the transplantation; however, it appeared to be dormant and then resurfaced during neutropenia caused by the transplantation. Therefore, the identification of the causative fungi is essential for determining whether to proceed with the transplantation. IFIs such as those in the present case require early definitive diagnosis and treatment. However, it is often challenging to identify pathogenic fungi from blood cultures or biopsy observations. In addition, the recent heavy use of immunosuppressive agents in the treatment of various diseases has led to an increase in fungal-caused infections. Such patients are susceptible to fungal infections that are rarely seen or reported as human pathogens and may be difficult for even experienced mycologists to identify [2]. Combining metagenome sequencing with in situ hybridization using probes may allow rapid and accurate identification of the causative fungus, even if the fungus has a small number of cells, is fragmented and dead or has no previous cases. This will facilitate the selection of an effective antifungal agent for the causative fungus and the determination of whether or not intensive treatment with antifungal prophylaxis can be continued.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stevens DL Bisno AL Chambers HF Dellinger EP Goldstein EJC et al Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America Clin Infect Dis 201459 e 10e 5210.1093/cid/ciu 44424973422 · doi ↗ · pubmed ↗
- 2Guarner J Brandt ME Histopathologic diagnosis of fungal infections in the 21st century Clin Microbiol Rev 20112424728010.1128/CMR.00053-1021482725 PMC 3122495 · doi ↗ · pubmed ↗
- 3Li H Guo M Wang C Li Y Fernandez AM et al Epidemiological study of Trichosporon asahii infections over the past 23 years Epidemiol Infect 2020148 e 16910.1017/S 095026882000162432703332 PMC 7439294 · doi ↗ · pubmed ↗
- 4Sadamoto S Shinozaki M Nagi M Nihonyanagi Y Ejima K et al Histopathological study on the prevalence of trichosporonosis in formalin-fixed and paraffin-embedded tissue autopsy sections by in situ hybridization with peptide nucleic acid probe Med Mycol 20205846046810.1093/mmy/myz 09631535126 PMC 7261608 · doi ↗ · pubmed ↗
- 5Ibáñez-Martínez E Ruiz-Gaitán A Pemán-García J Update on the diagnosis of invasive fungal infection Rev Esp Quimioter 201730162128882009 · pubmed ↗
- 6Nucci M Perfect JR When primary antifungal therapy fails Clin Infect Dis 2008461426143310.1086/58710118419447 · doi ↗ · pubmed ↗
- 7Yang S Rothman RE PCR-based diagnostics for infectious diseases: uses, limitations, and future applications in acute-care settings Lancet Infect Dis 2004433734810.1016/S 1473-3099(04)01044-815172342 PMC 7106425 · doi ↗ · pubmed ↗
- 8Chiu CY Miller SA Clinical metagenomics Nat Rev Genet 20192034135510.1038/s 41576-019-0113-730918369 PMC 6858796 · doi ↗ · pubmed ↗