The effect of convalescent plasma therapy on the rate of nucleic acid negative conversion in patients with persistent COVID-19 test positivity
Yixuan Wang, Zhe Xu, Xue Xu, Shuwen Yang, Yuanyuan Li, Hanwen Zhang, Yufeng Zhang, Fu-Sheng Wang, Ying Wang, Jingfeng Bi

TL;DR
This study found that convalescent plasma therapy does not significantly speed up the clearance of SARS-CoV-2 in patients with prolonged positive test results.
Contribution
The study provides evidence against the effectiveness of convalescent plasma in accelerating viral clearance for patients with persistent COVID-19 positivity.
Findings
Convalescent plasma therapy did not significantly increase the negative conversion rate on day five, ten, or fifteen post-therapy.
The hazard ratios for negative conversion were not statistically significant in any of the time points analyzed.
Findings do not support the hypothesis that convalescent plasma accelerates viral clearance in patients with prolonged positivity.
Abstract
This study investigates the association between convalescent plasma therapy and the negative conversion rate in patients with persistent COVID-19 test positivity. A retrospective analysis was conducted on patients with severe or mild to moderate COVID-19 whose viral nucleic acid tests remained positive for over 30 days. Patients were categorized into two groups: those who administered convalescent plasma therapy and those who were not. Data collected included information on therapy strategies used (convalescent plasma, corticosteroids, interferons, etc.), patients’ demographic characteristics, comorbidities, therapeutic medications, and nucleic acid testing results. Patients in the convalescent plasma therapy group were matched 1:2 ratio with those in the non-convalescent plasma therapy group. Cumulative negative conversion rates on the fifth, tenth, and fifteenth days post-therapy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
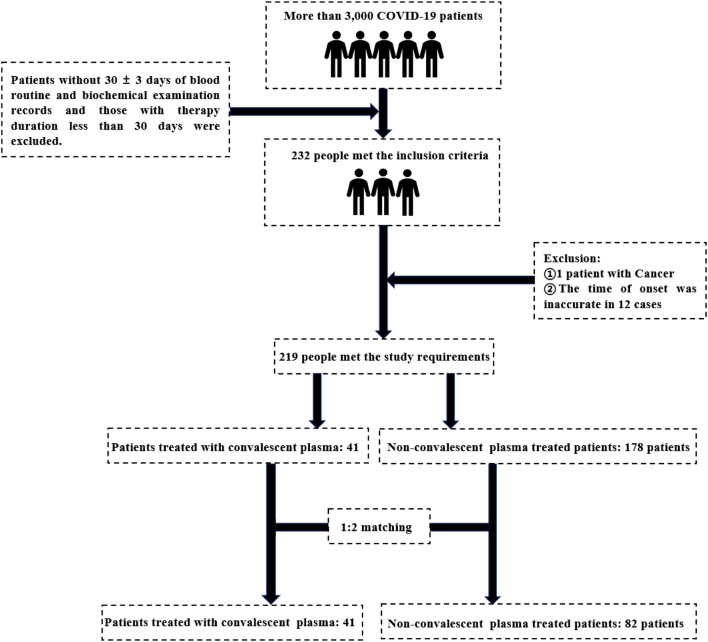 FIGURE 1
FIGURE 1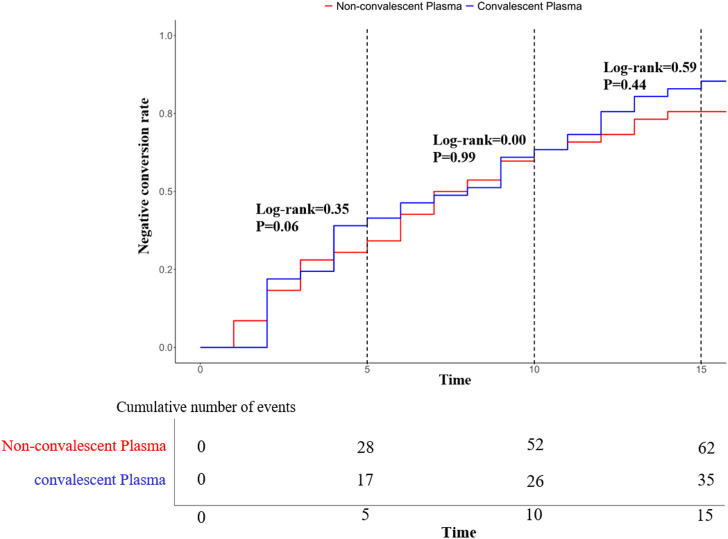 FIGURE 2
FIGURE 2| Trail | Convalescent plasma therapy group (N = 41) | Non-convalescent plasma therapy group (N = 82) |
|
|---|---|---|---|
| Age | 57 (51, 69) | 62 (51, 68) | 0.18 |
| Sex (n, %) | 0.42 | ||
| Male | 33 (40.24%) | 22 (53.66%) | |
| Female | 49 (59.76%) | 19 (46.34%) | |
| Severe or mild to moderate | 0.99 | ||
| Severe | 16 (26.23%) | 45 (73.77%) | |
| Mild to moderate | 16 (26.23%) | 45 (73.77%) | |
| Fever (n, %) | 64 (78.50%) | 28 (68.29%) | 0.24 |
| Clearance time (n, %) | 55.6 (48.0, 63.0) | 57.0 (47.0, 60.0) | 0.68 |
| Blood routine examination | |||
| WBC (109/L) | 5.5 (4.5, 7.0) | 5.7 (4.4, 7.1) | 0.95 |
| RBC (1012/L) | 3.8 ± 0.6 | 3.8 ± 0.6 | 0.76 |
| HGB (g/L) | 116.5 ± 17.0 | 118.1 ± 20.1 | 0.65 |
| PLT (109/L) | 228.6 ± 68.3 | 196.8 ± 62.5 | 0.01 |
| NE (109/L) | 3.3 (2.6, 4.0) | 3.4 (2.5, 4.6) | 0.81 |
| LYM (109/L) | 1.5 (1.1, 1.9) | 1.5 (1.1, 2.0) | 0.81 |
| MON (109/L) | 0.5 (0.3, 0.6) | 0.4 (0.3, 0.6) | 0.86 |
| Blood biochemical examination | |||
| ALT (IU/L) | 18.4 (11.9, 34.2) | 20.9 (13.4, 40.4) | 0.42 |
| AST (IU/L) | 18.2 (14.3, 23.0) | 18 (14.4, 24.8) | 0.85 |
| TP (g/L) | 65.4 (62.2, 71.0) | 65.9 (61.3, 68.7) | 0.66 |
| ALB (g/L) | 37.7 (35.0, 40.3) | 38.0 (36.2, 39.2) | 0.99 |
| GLO (g/L) | 27.3 (25.2, 30.5) | 28 (24.9, 30.4) | 0.54 |
| A/G | 1.4 ± 0.2 | 1.4 ± 0.3 | 0.29 |
| EOS (109/L) | 0.2 (0.02, 0.85) | 0.2 (0.01, 0.6) | 0.91 |
| BASO (109/L) | 0.03 (0.01, 0.12) | 0.03 (0.01, 0.05) | 0.97 |
| LDH (IU/L) | 186.2 (107.0, 325.9) | 218.0 (118.9, 637.9) | 0.89 |
| CK (IU/L) | 61.6 (11.8, 316.8) | 57.5 (12.7, 133.7) | 0.95 |
| BUN (mg/dL) | 4.8 (1.7, 12.7) | 4.9 (2.0, 12.3) | 0.87 |
| TBIL (umol/L) | 9.7 (8.2, 12.9) | 9.7 (8.0, 13.5) | 0.82 |
| DBIL (umol/L) | 2.9 (2.3, 3.4) | 3.5 (2.6, 4.9) | 0.07 |
| BUN (mmol/L) | 4.2 (3.5, 5.2) | 4.3 (3.9, 5.5) | 0.44 |
| CR (umol/L) | 58.6 (51.2, 72.1) | 62.0 (52.5, 74.3) | 0.48 |
| ALP (IU/L) | 68.3 (57.9, 82.7) | 70.3 (58.8, 81.6) | 0.51 |
| GGT (IU/L) | 26.5 (17.1, 49.8) | 26.1 (19.5, 49.8) | 0.57 |
| Concomitant disease (n, %) | |||
| Hypertension | 27 (32.93%) | 16 (39.02%) | 0.51 |
| Diabetic | 6 (7.41%) | 11 (26.83%) | 0.003 |
| Cardiovascular disease | 7 (8.54%) | 9 (21.95%) | 0.04 |
| Therapeutic strategy (n, %) | |||
| Thymosin | 41 (50.00%) | 24 (58.54%) | 0.37 |
| INF | 3 (3.75%) | 7 (8.40%) | 0.33 |
| Glucocorticoid | 13 (15.85%) | 13 (33.33%) | 0.03 |
| Fifth day | Tenth day | Fifteenth day | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Trait | Non-negative conversion (N = 82) | Negative conversion (N = 41) |
| Non-negative conversion (N = 82) | Negative conversion (N = 41) |
| Non-negative conversion (N = 82) | Negative conversion (N = 41) |
|
| Age | 63 (51, 69) | 63 (55, 69) | 0.60 | 63 (49, 69) | 62 (54, 69) | 0.75 | 66.5 (52, 70) | 61 (51, 69) | 0.54 |
| Sex (n, %) | 0.42 | 0.14 | 0.54 | ||||||
| Male | 37 (47.44%) | 18 (40.00%) | 24 (53.33%) | 31 (39.74%) | 13 (50.00%) | 42 (43.30%) | |||
| Female | 41 (52.56%) | 27 (60.00%) | 21 (46.67%) | 47 (60.26%) | 13 (50.00%) | 55 (56.70%) | |||
| Fever (n, %) | 64 (78.50%) | 28 (68.29%) | 0.24 | 31 (68.89%) | 61 (78.21%) | 0.25 | 18 (69.23%) | 74 (76.29%) | 0.46 |
| Blood routine examination | |||||||||
| WBC (109/L) | 5.5 (4.5, 7) | 5.7 (4.4, 7.1) | 0.95 | 5.6 (4.0, 5.7) | 5.6 (4.5, 7.1) | 0.89 | 5.7 (4.5, 7.2) | 5.6 (4.5, 7.0) | 0.76 |
| RBC (1,012/L) | 3.8 ± 0.6 | 3.8 ± 0.5 | 0.80 | 3.9 ± 0.6 | 3.8 ± 0.6 | 0.48 | 3.9 ± 0.6 | 3.8 ± 0.6 | 0.48 |
| HGB (g/L) | 117.2 ± 19.1 | 116.7 ± 16.3 | 0.89 | 119.8 ± 17.4 | 115.4 ± 18.3 | 0.19 | 121.3 ± 18.4 | 115.9 ± 17.8 | 0.18 |
| PLT (109/L) | 217.8 ± 68.7 | 218.3 ± 67.1 | 0.97 | 209.3 ± 74.3 | 223.0 ± 63.8 | 0.28 | 216.0 ± 77.2 | 218.6 ± 65.5 | 0.86 |
| NE (109/L) | 3.3 (2.4, 4.2) | 3.4 (2.9, 4.5) | 0.17 | 3.2 (2.2, 4.0) | 3.4 (2.6, 4.5) | 0.24 | 3.2 (2.4, 4.2) | 3.4 (2.6, 4.3) | 0.67 |
| LYM (109/L) | 1.6 (1.1, 1.9) | 1.5 (1.1, 2.3) | 0.90 | 1.7 (1.3, 1.9) | 1.4 (1.1, 2.0) | 0.28 | 1.6 (1.3, 1.9) | 1.5 (1.1, 2.0) | 0.66 |
| MON (109/L) | 0.4 (0.3, 0.6) | 0.5 (0.4, 0.6) | 0.33 | 0.4 (0.3, 0.5) | 0.5 (0.4, 0.6) | 0.26 | 0.4 (0.3, 0.6) | 0.5 (0.4, 0.6) | 0.44 |
| Blood biochemical examination | |||||||||
| ALT (IU/L) | 18.4 (12.1, 37.0) | 15.9 (11.7, 30.7) | 0.19 | 27.3 (13.4, 8.0) | 16.7 (11.4, 32.4) | 0.11 | 29.2 (12.3, 38.6) | 17.6 (12.3, 38.6) | 0.30 |
| AST (IU/L) | 18.6 (15.2, 25.0) | 16.7 (13.5, 22.4) | 0.07 | 18.7 (15.2, 25.0) | 17.5 (1,400, 23.5) | 0.28 | 20.8 (14.5, 26.4) | 18.0 (14.3, 3.2) | 0.40 |
| TP (109/L) | 66.0 ± 6.9 | 65.7 ± 5.1 | 0.79 | 65.7 ± 5.9 | 66.0 ± 6.5 | 0.80 | 65.7 ± 5.9 | 66.0 ± 6.4 | 0.88 |
| ALB (109/L) | 37.6 ± 4.4 | 37.6 ± 3.1 | 0.97 | 37.9 ± 3.9 | 37.4 ± 4.0 | 0.46 | 37.3 ± 4.0 | 37.6 ± 4.0 | 0.64 |
| GLO (109/L) | 28.0 (25.2, 30.5) | 27.1 (24.9, 30.4) | 0.49 | 27.3 (25.2, 30.1) | 27.5 (25.0, 31.6) | 0.54 | 27.6 (25.5, 29.2) | 27.5 (24.9, 30.5) | 0.86 |
| A/G | 1.4 ± 0.3 | 1.4 ± 0.3 | 0.51 | 1.4 (1.3, 1.6) | 1.4 (1.2, 1.5) | 0.17 | 1.4 ± 0.3 | 13.7 ± 0.2 | 0.98 |
| EOS (109/L) | 0.2 (0.04, 0.4) | 0.2 (0.01, 0.6) | 0.58 | 0.2 (0.04, 0.9) | 0.2 (0.01, 0.6) | 0.64 | 0.2 (0.04, 0.9) | 0.2 (0.01, 0.6) | 0.69 |
| BASO (109/L) | 0.03 (0.01, 0.1) | 0.03 (0.01, 0.05) | 0.68 | 0.03 (0.01, 0.1) | 0.03 (0.01, 0.05) | 0.69 | 0.03 (0.01, 0.1) | 0.03 (0.01, 0.05) | 0.72 |
| LDH (IU/L) | 183.3 (120.1, 325.0) | 218.6 (118.9, 493.8) | 0.78 | 186.7 (120.1, 325.0) | 218.6 (118.9, 493.8) | 0.77 | 186.7 (120.1, 325.0) | 217.9 (118.9, 637.9) | 0.97 |
| CK (IU/L) | 63.2 (19.1, 316.8) | 57.3 (12.7, 133.7) | 0.91 | 61.5 (11.8, 316.8) | 57.3 (12.7, 316.8) | 0.89 | 61.5 (11.8, 316.8) | 56.7 (12.7, 133.7) | 0.87 |
| BUN (mg/dL) | 4.5 (2.63, 5.85) | 4.7 (4.1, 8.5) | 0.88 | 4.5 (2.6, 5.9) | 4.7 (3.4, 8.5) | 0.65 | 4.5 (2.6, 10.5) | 4.8 (3.4, 8.5) | 0.88 |
| TBIL (umol/L) | 9.8 (8.1, 12.9) | 9.4 (8.0, 13.5) | 0.99 | 9.6 (8.1, 12.6) | 9.7 (8.0, 13.5) | 0.99 | 10.6 (8.6, 12.6) | 9.5 (8.0, 13.4) | 0.55 |
| DBIL (umol/L) | 3.2 (2.4, 4.2) | 3 (2.5, 4.5) | 0.86 | 3.3 (2.4, 4.2) | 3.0 (2.5, 4.3) | 0.43 | 3.6 (2.5, 4.6) | 3.0 (2.3, 3.9) | 0.17 |
| BUN (umol/L) | 4.4 (3.8, 5.5) | 4.06 (3.5, 5.1) | 0.22 | 4.3 (3.9, 5.5) | 4.3 (3.7, 5.2) | 0.62 | 4.6 (3.9, 5.9) | 4.3 (3.7, 5.2) | 0.25 |
| CR (umol/L) | 60.4 (51.2, 73.3) | 58.7 (52.5, 70.1) | 0.51 | 59.4 (52.1, 76.7) | 60.4 (51.3, 72.5) | 0.82 | 59.2 (51.2, 81.3) | 60.3 (51.4, 72.5) | 0.58 |
| ALP (IU/L) | 70.0 (57.9, 91.9) | 68.6 (58.8, 79.6) | 0.53 | 69.6 (54.4, 85.1) | 68.7 (58.0, 81.6) | 0.87 | 70.6 (54.4, 81.9) | 68.8 (58.0, 82.7) | 0.85 |
| GGT (IU/L) | 28.0 (19, 47.4) | 24.9 (17.8, 53.8) | 0.83 | 27.4 (16.2, 44.0) | 25.6 (18.4, 53.7) | 0.50 | 28.1 (16.2, 44.0) | 25.6 (18.4, 53.7) | 0.58 |
| Concomitant disease (n, %) | |||||||||
| Hypertension | 28 (35.90%) | 15 (33.33%) | 0.77 | 13 (28.89%) | 30 (38.45%) | 0.28 | 9 (34.62%) | 34 (35.05%) | 0.97 |
| Diabetes | 11 (14.10%) | 6 (16.64%) | 0.94 | 5 (11.11%) | 12 (15.58%) | 0.49 | 3 (11.54%) | 14 (14.58%) | 0.99 |
| Cardiovascular Disease | 13 (16.67%) | 3 (6.67%) | 0.11 | 7 (15.56%) | 9 (11.54%) | 0.52 | 4 (15.38%) | 12 (12.37%) | 0.74 |
| Therapeutic strategy (n, %) | |||||||||
| Thymosin | 41 (51.28%) | 25 (55.56%) | 0.65 | 25 (55.56%) | 40 (51.28%) | 0.65 | 16 (61.54%) | 49 (505.2%) | 0.32 |
| INF | 16 (20.51%) | 7 (15.56%) | 0.50 | 9 (20.00%) | 14 (17.95%) | 0.78 | 5 (19.23%) | 18 (18.54%) | 0.99 |
| Glucocorticoid | 16 (21.05%) | 10 (22.22%) | 0.88 | 16 (21.05%) | 10 (22.22%) | 0.88 | 6 (23.08%) | 20 (21.05%) | 0.82 |
| Convalescent plasma | 28 (62.22%) | 17 (37.78%) | 0.43 | 52 (66.67%) | 26 (33.33%) | 0.99 | 62 (63.92%) | 35 (36.08%) | 0.21 |
| Trait | HR | 95% CI |
| |
|---|---|---|---|---|
| Fifth day | NE (109/L) | 0.99 | 0.83–1.17 | 0.89 |
| ALT (IU/L) | 1.00 | 0.98–1.03 | 0.76 | |
| AST (IU/L) | 1.00 | 0.93–1.07 | 0.94 | |
| Convalescent plasma | 1.72 | 0.82–3.61 | 0.15 | |
| Cardiovascular Disease | 0.31 | 0.08–1.22 | 0.09 | |
| Tenth day | HGB (g/L) | 1.00 | 0.98–1.02 | 0.95 |
| ALT (IU/L) | 0.99 | 0.98–1.01 | 0.28 | |
| A/G | 0.45 | 0.10–2.10 | 0.31 | |
| SEX | 0.90 | 0.46–1.77 | 0.76 | |
| Convalescent plasma | 1.25 | 0.69–2.26 | 0.46 | |
| Fifteenth day | HGB (g/L) | 0.99 | 0.98–1.01 | 0.43 |
| DBIL (umol/L) | 1.02 | 0.83–1.24 | 0.88 | |
| Convalescent plasma | 1.19 | 0.72–1.97 | 0.51 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Clinical Research Studies · SARS-CoV-2 and COVID-19 Research · Long-Term Effects of COVID-19
1 Introduction
Coronavirus disease 2019 (COVID-19) is a severe atypical respiratory infection first reported in Wuhan, China, in December 2019. COVID-19 is an infectious disease caused by the coronavirus COVID-19, which can cause a variety of respiratory diseases, colds, fever, and other symptoms, with a high infection rate, rapid mutation rate, low blood oxygen in the human body (Ar Gouilh et al., 2018; Gattinoni et al., 2021; Ochani et al., 2021; Rahman et al., 2021). The disease has rapidly spread around the world, causing a great impact on the global economy and serious damage to human health, resulting in millions of confirmed cases and hundreds of thousands of deaths (Gavriatopoulou et al., 2021).
In the face of the sudden onset of COVID-19, clinicians have adopted a variety of aggressive therapy strategies, including the use of Chinese medicine, thymosin, interferon, and convalescent plasma therapy (Dai et al., 2020; Chen et al., 2021; Huang et al., 2021; Smith et al., 2022; Bellet et al., 2023). Convalescent plasma therapy is an important means of therapy that has many benefits for patients, can effectively shorten the discharge time and improve the symptoms of patients (Janiaud et al., 2021). In the previous outbreak of severe acute respiratory syndrome (SARS) caused by SARS-CoV-1 coronavirus, studies have shown that convalescent plasma therapy can effectively shorten the course of disease, accelerate recovery, and reduce mortality (Zhou X. et al., 2003; Berger et al., 2004; Cheng et al., 2005).
At present, there have been several clinical studies on convalescent plasma therapy, and there have been some controversies. For example, some studies have found that there is no significant correlation between convalescent plasma therapy and the mortality of COVID-19 patients, and the survival and discharge rates of patients in the convalescent plasma therapy group and the non-convalescent plasma therapy group are similar (RECOVERY Collaborative Group, 2021). However, one study found that convalescent plasma therapy can effectively reduce the mortality of patients (Liu Z, 2020), and another study has shown that convalescent plasma therapy can improve the rate of negative conversion in COVID-19 patients over 60 days (Duan et al., 2022; Pan et al., 2022). Therefore, we conducted this study to investigate the relationship between convalescent plasma therapy and the viral clearance rate in patients with prolonged COVID-19 positivity.
2 Materials and methods
2.1 Research overview
This study included all patients with severe or mild to moderate COVID-19 diagnosed in 2020 at Huo Shenshan Hospital and Taikang Tongji Hospital in Wuhan, Hubei Province, China. It has been reviewed and approved by the Medical Ethics Committee of the Fifth Medical Center of the PLA General Hospital (approval number: 2020075D).
2.2 Inclusion criteria
(1) Age >18 years old, gender unlimited; (2) All patients included in the study met the diagnostic criteria for COVID-19 (Lin and Li, 2020); (3) Severe or mild to moderate cases, the manifestations of fever and respiratory symptoms, imaging findings of pneumonia; (4) Nucleic acid positive duration more than 30 days; (5) Nucleic acid testing was performed every 1–3 days after 30 days in all patients to determine whether the nucleic acid turned negative; (6) COVID-19 detection is to extract nucleic acid from specimens using an automatic nucleic acid extraction instrument (KingFisher Flex, Thermo Company), collect purified nucleic acid for real-time fluorescent RT-PCR detection, and the period threshold (CT) value of 40 or greater is considered negative; (7) All patients had blood routine and biochemical examination records for 30 ± 3 days.
2.3 Exclusion criteria
(1) Patients with malignant tumors and malignant blood diseases; (2) Acquired immune deficiency syndrome (AIDS) patients; (3) Patients with liver failure or renal failure; (4) Patients with incomplete clinical information (see “Section 2.5”) (Lin and Li, 2020); (5) Other diseases that researchers believe may affect this study, such as lupus erythematosus.
2.4 Standard for negative conversion
Refer to “Diagnosis and Therapy Protocol for COVID-19 (Trial Fifth Revised Version)”, and negative nucleic acid tests of respiratory pathogens were performed two consecutive times with a time interval of 24 h or more.
2.5 Clinical Information collection
The following data were obtained from clinical records: (1) demographic data (gender, age); (2) concomitant diseases (such as diabetes, hypertension, cardiovascular and cerebrovascular diseases, respiratory diseases, chronic liver diseases, hematopoietic diseases, etc.); (3) The status of therapeutic drugs; (4) nucleic acid test negative time (see negative criteria); (5) 30 ± 3 days blood routine and blood biochemical test results; (6) Other therapy strategies.
2.6 Case matching method
The convalescent plasma therapy group and the non-convalescent plasma therapy group were matched in ratio of 1:2 by therapy time (date of convalescent plasma therapy minus date of onset). The matching method was as follows: The convalescent plasma therapy group was sorted according to the time interval between onset and convalescent plasma therapy. Patients in the convalescent plasma therapy group with the longest time interval between the therapy date and the onset date were first selected, and the patients with a negative conversion time longer than this interval were chosen from the non-convalescent plasma therapy group, and twice as many patients from the non-convalescent plasma therapy group over this were randomly selected for matching. The remaining patients entered the matching process with the second patient in the convalescent plasma therapy group, and so on. Until the last patient in the convalescent plasma therapy group was matched.
2.7 Statistical analysis
They were divided into two groups: the convalescent plasma therapy group, which received convalescent plasma therapy, and the non-convalescent plasma therapy group, which did not receive convalescent plasma therapy. The baseline conditions of the two groups were analyzed. mean ± SD was used to represent measurement data when they met normality, and a T-test was used for comparison between groups. When the measurement data did not conform to normality, the median (IQR) was used, and the Wilcoxon rank sum test was applied for inter-group comparison. The patients were grouped according to whether they turned negative on the fifth day, tenth day, or fifteenth day after receiving convalescent plasma therapy, and univariate analysis was conducted to explore the relationship between the respective variables and the dependent variables under univariate conditions and to provide a basis for the selection of independent variables. The statistical analysis method is the same as above. With whether or not the nucleic acid turned negative on the fifth day, tenth day, and fifteenth day as the dependent variable, variables with P < 0.20 in the above univariate analysis were selected as independent variables. The Cox proportional risk model was used to analyze the relationship between convalescent plasma therapy and nucleic acid turning negative after adjusting for the influence of other independent variables. All the above statistical analysis processes were completed based on SAS 9.4, and both were adopted by a two-sided test (α = 0.05).
3 Result
The initial sample size was 3,000 patients. After excluding the patients without 30 ± 3 days of routine blood and biochemical examination records and the therapy time was less than 30 days, a total of 232 patients meeting the inclusion criteria were enrolled in the study. Excluding tumor patients and 12 patients with inaccurate specific onset time, 219 patients met the requirements of this study, of which 41 patients received convalescent plasma therapy. After 1:2 matching, 123 patients were finally included, including 41 patients in the convalescent plasma therapy group and 82 patients in the non-convalescent plasma therapy group (see Figure 1).
The process of case matching.
3.1 Baseline data of patients in the convalescent plasma therapy group and non-convalescent plasma therapy group
The results showed that there were significant differences in platelet (PLT, P = 0.01), diabetes (P = 0.003), cardiovascular and cerebrovascular diseases (P = 0.04), interferon use (INF, P = 0.009), and glucocorticoid therapy (P = 0.03) between the two groups, suggesting that the baseline of the two groups was unbalanced (see Table 1).
3.2 Univariate analysis related to negative nucleic acid transformation on the fifth day, tenth day, and fifteenth day
The results showed that when the fifth-day cumulative conversion rate was used as the dependent variable, the independent variables with P < 0.20 were neutrophil (NE, P = 0.17), Glutamic-pyruvic transaminase (ALT, P = 0.19), Glutamic oxalacetic transaminase (AST, P = 0.07) and cardiovascular and cerebrovascular diseases (P = 0.11). When the tenth day cumulative conversion rate was used as the dependent variable, the independent variables with P < 0.20 were sex (P = 0.14), hemoglobin (HGB, P = 0.19), Glutamic-pyruvic transaminase (ALT, P = 0.11) and the ratio of albumin to globulin (A/G, P = 0.17). On the fifteenth day, when cumulative conversion rate was a factor variable, the self-variability of P < 0.20 was HGB (P = 0.18) and direct bilirubin (DBIL, P = 0.17) (see Table 2).
3.3 Multi-factor analysis related to negative nucleic acid transformation on the fifth day, tenth day, and fifteenth day
The Cox proportional risk model was applied to stratify the matched groups, with cumulative conversion rate on the fifth day as the dependent variable, and indexes with P < 0.20 in Table 2, including NE, ALT, AST, cardiovascular and cerebrovascular diseases, as the adjusting variables. There was no statistical significance between the convalescent plasma therapy group and the non-convalescent plasma therapy group (HR: 1.72, 95% CI: 0.82–3.61, P = 0.15). With the cumulative conversion rate on the tenth day as the dependent variable and the indexes with P < 0.20 in the results in Table 2, including HGB, ALT, A/G, and gender as the adjusting variables, there was no significant statistical significance between the convalescent plasma therapy group and the non-convalescent plasma therapy group (HR: 1.25, 95% CI: 0.69–2.26, P = 0.46); With the cumulative conversion rate on the fifteenth day as the dependent variable and the indexes with P < 0.20 in the results of Table 2, including HGB and DBIL as the adjusted variables, there was no significant statistical significance between the convalescent plasma therapy group and the non-convalescent plasma therapy group (HR: 1.19, 95% CI: 0.72–1.97, P = 0.51) (see Table 3).
3.4 Comparison of Kaplan-Meier curve of negative conversion rate between the two groups
The Kaplan-Meier curve of negative conversion rate between the convalescent plasma therapy group and the non-convalescent plasma therapy group showed that log-rank = 0.35, P = 0.56 cumulative conversion rate on the fifth day was taken as the dependent variable. When the cumulative conversion rate on the tenth day was taken as the dependent variable, log-rank = 0.00, P = 0.99; When the cumulative conversion rate on the fifteenth day was taken as the dependent variable, log-rank = 0.59, P = 0.44. These results showed that there was no statistical significance in Kaplan-Meier negative conversion rate curves between the convalescent plasma therapy group and the non-convalescent plasma therapy group on day 5, day 10, and day 15 (see Figure 2).
Kaplan-Meier curve of negative conversion rate in two groups.
4 Discussion
The COVID-19 pandemic represents one of the most significant public crises in recent years. Determining the efficacy of convalescent plasma therapy in converting consistently COVID-19 positive patients to negative status is of paramount importance. To address this issue, we conducted a retrospective analysis and performed a cohort study on two groups of patients: those who received convalescent plasma therapy and those who did not receive convalescent plasma therapy. The convalescent plasma therapy group and the non-convalescent plasma therapy group were matched in 1:2 by therapy time (date of convalescent plasma therapy minus date of onset). The matching method was as follows: The convalescent plasma therapy group was sorted according to the time interval between onset and convalescent plasma therapy. Patients in the convalescent plasma therapy group with the longest time interval between the therapy date and the onset date were first selected, and the patients with a negative conversion time longer than this interval were chosen from the non-convalescent plasma therapy group, and twice as many patients from the non-convalescent plasma therapy group over this were randomly selected for matching. The remaining patients entered the matching process with the second patient in the convalescent plasma therapy group, and so on. Until the last patient in the convalescent plasma therapy group was matched. Initially, we performed univariate analysis on all independent variables. Factors with a P < 0.20 from the univariate analysis were then included in the Cox proportional hazards model for multivariate analysis. The results showed that after adjusting for other factors (NE, ALT, AST, cardiovascular and cerebrovascular diseases), we still did not find a statistical difference between therapy with convalescent plasma and therapy without convalescent plasma.
Our study does not support the association between convalescent plasma therapy and acceleration of SARS-CoV-2 conversion among COVID-19 patients with persistent positive RT-PCR tests. During the 2002 outbreak of Severe Acute Respiratory Syndrome (SARS), convalescent plasma therapy was shown to significantly facilitate the conversion of patients who continued to test positive for the SARS virus to negative (Berger et al., 2004). Therefore, during the current COVID-19 pandemic, many clinicians have also employed convalescent plasma therapy to expedite viral clearance in patients. Recent years have seen numerous randomized clinical trials indicating that convalescent plasma therapy shows no significant association with clinical outcomes (Discharge, death, etc.) in patients with persistent positive COVID-19 test results (Agarwal et al., 2020b; Li et al., 2020; AlQahtani et al., 2021; Balcells et al., 2021; O’Donnell et al., 2021; Simonovich et al., 2021; Iannizzi et al., 2023). This aligns with the findings in the WHO COVID-19 Therapy Guidelines regarding convalescent plasma therapy (Agarwal et al., 2020a). However, these studies have not specifically investigated whether convalescent plasma therapy is related to the transition to negative test results in these patients. Our study further supplemented the evidence, demonstrating that convalescent plasma therapy is ineffective in accelerating viral clearance in patients who remain persistently positive for COVID-19. This finding is significant for the therapy of COVID-19 patients, as it suggests that convalescent plasma may not effectively shorten the recovery period or promote patient recuperation. We recommend incorporating these findings into current therapy protocols, which may lead clinicians to use convalescent plasma prudently when treating patients with persistent COVID-19 test positivity, not only to avoid the risk of donation from donors, but also to reduce the risk of ineffective therapy for patients.
Previous research on convalescent plasma therapy for COVID-19 has highlighted its potential benefits and limitations, warranting further investigation into its clinical efficacy and safety. Some studies have shown that administering convalescent plasma from recovered patients to severely ill individuals can rapidly provide immunoglobulins, allowing for timely therapy and potentially becoming an important therapeutic measure, especially for those with compromised immunity (Ouyang et al., 2020; Senefeld et al., 2023). Additionally, early-stage administration of convalescent plasma therapy has been suggested to offer clear clinical benefits due to the rapid viral replication and high viral load in patients (Sun et al., 2020). Our data included both severe patients with COVID-19 and those with early-stage COVID-19 infection, but in neither case did convalescent plasma therapy demonstrate a positive effect on clinical outcomes. Moreover, convalescent plasma therapy remains an “experimental therapy” in clinical practice (Zeller et al., 2015). Its composition, which includes various components, can lead to serious medical complications such as allergic reactions in recipients (Shu et al., 2021; Wood et al., 2021; Sullivan et al., 2022; Senefeld et al., 2023). Compared to small molecule drugs, convalescent plasma therapy is less safe and lacks sufficient clinical research (Chai et al., 2020). Therefore, extensive prospective clinical trials are necessary to further explore its efficacy and safety.
The advantage of this study is that we used data from Wuhan, where all COVID-19 patients were systematically and centrally isolated and treated, and comprehensive patient data were obtained. Each patient was continuously observed until they tested negative for nucleic acid and discharged, providing a complete and continuous dataset from admission to discharge. However, this study also has several limitations: 1) Although the initial sample size was large, with over 3,000 cases, only 219 cases met the study criteria, and after matching, only 123 cases were included, making it a small retrospective cohort study; 2) Due to the inherent limitations of retrospective studies, the measured factors included in the analysis may not be complete, and some unknown factors may lead to bias in the results.
5 Conclusion
This study does not support that convalescent plasma therapy is associated with acceleration of negative conversion in COVID-19 patients with persistent positive RT-PCR tests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agarwal A.Hunt B.Stegemann M.Rochwerg B.Lamontagne F.Siemieniuk R. A. (2020 a). A living WHO guideline on drugs for covid-19. BMJ Clin. Res. ed. 370, m 3379. 10.1136/bmj.m 3379 32887691 · doi ↗ · pubmed ↗
- 2Agarwal A.Mukherjee A.Kumar G.Chatterjee P.Bhatnagar T.Malhotra P. (2020 b). Convalescent plasma in the management of moderate covid-19 in adults in India: open label phase II multicentre randomised controlled trial (PLACID Trial). BMJ (Clinical research ed.) 371, m 3939. 10.1136/bmj.m 3939 PMC 757866233093056 · doi ↗ · pubmed ↗
- 3Al Qahtani M.Abdulrahman A.Almadani A.Alali S. Y.Zamrooni A. M. A.Hejab A. H. (2021). Randomized controlled trial of convalescent plasma therapy against standard therapy in patients with severe COVID-19 disease. Sci. Rep. 11, 9927. 10.1038/s 41598-021-89444-5 33976287 PMC 8113529 · doi ↗ · pubmed ↗
- 4Ar Gouilh M.Puechmaille S. J.Diancourt L.Vandenbogaert M.Serra-Cobo J.Lopez Roïg M. (2018). SARS-Co V related Betacoronavirus and diverse Alphacoronavirus members found in western old-world. Virology 517, 88–97. 10.1016/j.virol.2018.01.014 29482919 PMC 7112086 · doi ↗ · pubmed ↗
- 5Balcells M. E.Rojas L.Le Corre N.Martínez-Valdebenito C.Ceballos M. E.Ferrés M. (2021). Early versus deferred anti-SARS-Co V-2 convalescent plasma in patients admitted for COVID-19: a randomized phase II clinical trial. P Lo S Med. 18 (3), e 1003415. 10.1371/journal.pmed.1003415 33657114 PMC 7929568 · doi ↗ · pubmed ↗
- 6Bellet M. M.Renga G.Pariano M.Stincardini C.D’Onofrio F.Goldstein A. L. (2023). COVID-19 and beyond: reassessing the role of thymosin alpha 1 in lung infections. Int. Immunopharmacol. 117, 109949. 10.1016/j.intimp.2023.109949 36881979 PMC 9977614 · doi ↗ · pubmed ↗
- 7Berger A.Drosten C. h.Doerr H. W.Stürmer M.Preiser W. (2004). Severe acute respiratory syndrome (SARS)--paradigm of an emerging viral infection. J. Clin. virology 29 (1), 13–22. 10.1016/j.jcv.2003.09.011 14675864 PMC 7128705 · doi ↗ · pubmed ↗
- 8Chai K. L.Valk S. J.Piechotta V.Kimber C.Monsef I.Doree C. (2020). Convalescent plasma or hyperimmune immunoglobulin for people with COVID-19: a living systematic review. Cochrane database Syst. Rev. 10, CD 013600. 10.1002/14651858.CD 013600.pub 3 32648959 PMC 7389743 · doi ↗ · pubmed ↗