Concurrent papular and dyshidrotic mycosis fungoides: A case report in a patient with skin of color
Bryan Ma, Brian D. Rankin, Melissa Yanitski, Xiu Y. Jiang, Lesley Street, Jori Hardin

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3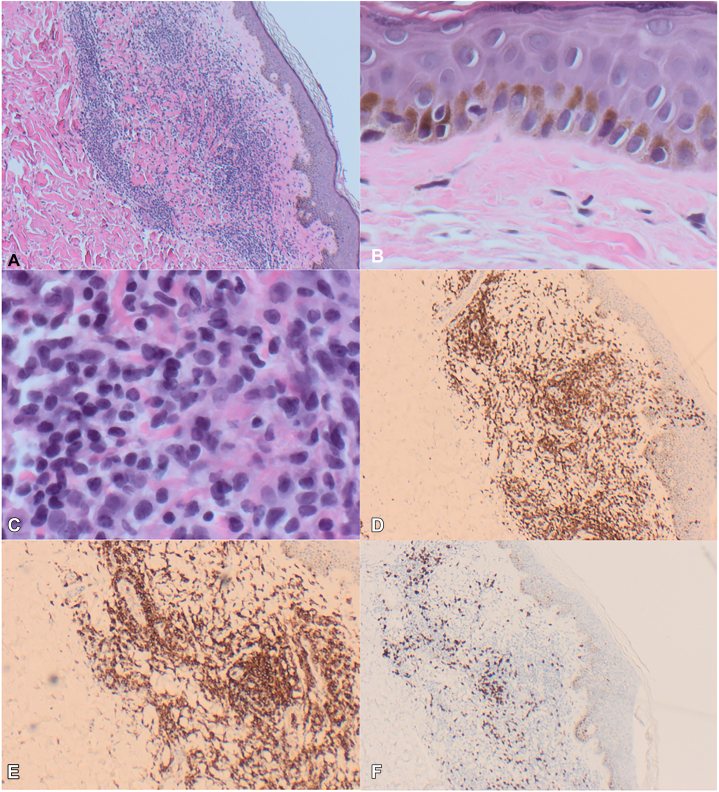 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · Vascular Tumors and Angiosarcomas · Nail Diseases and Treatments
Introduction
Mycosis fungoides (MF) is the most common form of cutaneous T-cell lymphoma (CTCL).1 MF classically presents as variably scaly, atrophic, erythematous patches distributed on sun-protected sites with the potential to progress to plaques and tumors. Several clinical variants of MF have been described,2^,^3 but there have been limited reports of multiple clinical morphologic forms of MF appearing simultaneously, especially a combination of uncommon variants like papular or dyshidrotic MF. Furthermore, with the exception of hypopigmented MF, clinical variants in skin of color have been lacking.4 Therefore, we present a case report and literature review of a unique presentation of mycosis fungoides in a Black individual.
Case report
A 57-year-old male who self-identified as Canadian with Ethiopian ancestry presented with a 2-year history of scattered intensely pruritic papules and vesicles that started on the flexor aspect of his forearms and progressively spread to include his posterior calves, thighs, and the palmar aspects of his hands bilaterally. He applied betamethasone valerate 0.1% cream and 0.1% ointment to affected areas intermittently to no effect.
On examination, there were erythematous lichenoid papules coalescing into plaques across the upper and lower extremities bilaterally. The palms of both hands had groups of clustered vesicles with a solitary tense bulla. Total affected body surface area was approximately 10%. There was no palpable lymphadenopathy (Fig 1, Fig 2, Fig 3).Fig 1. Papular mycosis fungoides of the bilateral ventral forearms.Fig 2. Papular mycosis fungoides of the right posterior thigh. Site of punch biopsy circled in black ink.Fig 3. Vesicular and dyshidrotic mycosis fungoides of the right palmar surface.
Biopsy of the right lateral palmar surface from May 2022 showed spongiotic dermatitis with vesiculation and eosinophils. An initial biopsy of the left superior dorsal forearm showed spongiosis with a dense dermal lymphoeosinophilic infiltrate with abundant Langerhans cells. The infiltrate was composed of atypical monoclonal CD2/CD3/CD4/CD5 positive T cells. Repeat biopsy in 2023 of the right superior dorsal forearm showed an atypical monoclonal CD3/CD4 positive T-cell proliferation, an expansile superficial dermal and perivascular infiltrate of small and intermediate size lymphoid cells with convoluted nuclear contours, and cytologic atypia. The epidermis showed Pautrier’s microabscesses with subtle and focal dermo-epidermotropism affecting the basal layer. Immunohistochemistry showed a preponderance of CD2/CD3/CD4/CD5 positive T-cells with near total loss of CD7 expression.
Given the clinical papular appearance, another punch biopsy was performed of the right posterior thigh. This showed rare exocytosis of lymphocytes into the epidermis and an infiltration of lymphoid cells in the upper dermis. Lymphocytes were small with slightly irregular nuclear contours and hyperchromatic nuclei. A monoclonal TCR beta and gamma gene rearrangement was identified, and this matched rearrangements found in previous biopsies extending back 1 year from the right palm and bilateral forearms, as well as in circulating lymphocytes in the blood. Immunohistochemistry showed CD2/CD3/CD4/CD5 positive T-cells that were negative for CD25 (Fig 4) with a CD4:CD8 ratio of approximately 8:1. Peripheral blood flow cytometry done twice showed atypical CD4+/CD7-/CD26- and CD4+/CD7-/CD26- clonal T-cell populations accounting for 18% and 24% of all lymphocytes (absolute count 540 and 720 cells per mm^3^), respectively. There was no follicular infiltration. Human T-lymphotropic virus 1 serology was negative. Serum lactate dehydrogenase was within normal limits.Fig 4. Representative pathology and immunohistochemistry slides. A, 4× magnification of the upper dermis showing a lymphocytic infiltrate (H&E); (B) 40× magnification showing rare lymphocyte exocytosis (H&E); (C) 40× magnification of small and medium atypical lymphoid cells (H&E); (D) CD3 positive T-cells (CD3 IHC); (E) CD4 positive T-cells (CD4 IHC); and (F) Minimal CD8 positive T-cells (CD8 IHC).
Consequently, a final diagnosis of stage IB (T2N0M0B1b) papular and dyshidrotic mycosis fungoides was made. The patient declined escalation of treatment with phototherapy, systemic retinoids, and/or interferon. He improved dramatically with betamethasone valerate 0.1% ointment twice daily within 2 months and at 9 months of follow-up, his disease remains improved much with <1% affected BSA.
Discussion
To the best of our knowledge, this is not only the first reported case of papular MF with concurrent dyshidrotic MF, but also the first description of a unique combination of MF morphologies in a patient with skin of color.
Papular MF was initially reported by Kodama et al5 in a case series of 6 patients. Since then, there have been less than 20 cases reported (Table I). Based on the reported cases, the median age of onset is 57 years with a slight male predominance (1.42:1). The most common presentation is discrete erythematous papules that are <1 cm in size distributed symmetrically across the trunk and extremities. Despite the unique clinical presentation, the histologic and immunohistochemical features of papular MF are generally similar to that of classic disease with epidermotropic, pleomorphic lymphocytic infiltrates. Numerous effective treatment regimens have been attempted including topical corticosteroids, phototherapy, psoralen with ultraviolet A, and extracorporeal photopheresis; most cases demonstrate a complete response, though relapsing and recurring lymphoma has been reported.5 Based on published case reports, this entity appears to have indolent clinical behavior with a 100% disease specific survival rate at a median of 36 months of follow-up. Only 2 cases were reported to have more than one clinical MF morphology. Therefore, this is only the third case of reported papular MF appearing simultaneously with another morphology, and the first case in combination with dyshidrotic MF, an even rarer morphology with only two other published reports of dyshidrotic disease in the literature (Table I).Table IDemographics, clinical presentation, and histopathology of previously reported cases of papular and dyshidrotic mycosis fungoidesStudy and yearPatient numberAge and sexLocationConcurrent or prior MFTreatmentBest responseFollow-up durationKodama et al 2005157 MTrunkNoPUVAComplete response18 mo258 FTrunk and upper extremitiesNoPUVA and ECPPartial response51 mo341 MLower extremitiesYes, patch stage disease detected months after diagnosis of papular MF with pathology confirming the diagnosis. Present concurrently.PUVAComplete response132 mo459 MTrunk and extremitiesNoPUVAComplete response24 mo561 MBack, flanks, and shouldersNoPUVAComplete response72 mo657 FTrunk, upper and lower extremitiesYes, classic patch MF appeared 3 y after diagnosis with pathology confirming diagnosis. Not present concurrently.PUVAComplete response120 moUddin et al 2007731 FTrunk, upper extremitiesNoUVBResponded to therapy, degree of improvement not reported10 moLiu et al 2010827 MChest, axillae, and left popliteal fossaNoTopical high-potency corticosteroids daily with retinoids nightly, NB-UVBPartial responseNot reportedMartorell-Calatayud et al 2010950 FLateral trunkNoClobetasol dipropionate 0.1% ointment twice dailyComplete response15 mo1055 FTrunk, buttocks, feetNoPUVAComplete response20 moNeri et al 20111147 FLower extremitiesNoPUVA, spontaneous responseComplete response60 moNoe et al 20131283 FAbdomen, trunk, proximal extremitiesNoTopical corticosteroid, topical mechlorethamine, NB-UVB, resolution with ECPPartial response48 mo1365 FChest, mid-lower back, abdomenNoTopical mechlorethamine, PUVA, and then methotrexatePartial response36 moBrajon et al 20131463 MTrunkNoTopical high-potency corticosteroid (clobetasol cream 0.05%), narrow-band ultraviolet BComplete responseNot reportedSantamarina-Albertos et al 20141555 MLower extremitiesNoTopical high-potency corticosteroid (clobetasol cream 0.05%), PUVAComplete response18 moBalta et al 20151633 MTrunk, extremitiesNoPUVAComplete response10 moKimet al 20161766 MTrunk, extremitiesNoNarrow-band ultraviolet B, topical high-potency corticosteroidStable disease36 moGoto et al 20211861 MTrunkNoNarrow-band ultraviolet BComplete response36 moDyshidrotic MFDiehl et al 2011173 FSoles, ankles, and heelsNoNB-UVB, clobetasol 0.05% ointment twice dailyPartial response15 moJuan-Carpena et al 2021258 FPalms and solesNoOral PUVA, topical 5% imiquimod, topical mechlorethamine, 16% MAL-PDTComplete response12 mo
Additionally, there have been no previously reported cases of either papular or dyshidrotic MF in a Black individual. CTCL is an important diagnosis for healthcare providers to consider in Black patients, especially since the typical morphology of MF may be more challenging to identify in darker skin tones, resulting in misdiagnosis for more common inflammatory diagnoses such as atopic dermatitis, psoriasis, or pityriasis alba.6 Currently, Black patients are underrepresented in MF case reports and randomized controlled trials despite CTCL disproportionately affecting Black patients with a higher incidence rate, earlier age of disease onset, and more aggressive malignancy at time of diagnosis compared to White patients.7, 8, 9 Large cancer database analyses have suggested that overall survival and disease-free survival in Black patients with MF are significantly poorer than those of White patients despite controlling for relevant disease, socioeconomic, and treatment factors.10 Therefore, further research is required to determine whether more uncommon and challenging to detect MF variants like papular and dyshidrotic MF may be associated with worse outcomes in Black patients.
In conclusion, we present a rare case of combination papular and dyshidrotic mycosis fungoides in a Black patient. CTCL is an important diagnosis for healthcare providers to consider in patients with skin of color, and dermatologists must be aware of the multiplicity of ways that MF and its clinical variants may present.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kaufman A.E.Patel K.Goyal K.Mycosis fungoides: developments in incidence, treatment and survival J Eur Acad Dermatol Venereol 34102020228822943214111510.1111/jdv.16325 PMC 7733543 · doi ↗ · pubmed ↗
- 2Ahn C.S.AL Sayyah A.Sangüeza O.P.Mycosis fungoides: an updated review of clinicopathologic variants Am J Dermatopathol 362014933948 quiz 949-512541513810.1097/DAD.0000000000000207 · doi ↗ · pubmed ↗
- 3Geller S.Lebowitz E.Pulitzer M.P.Outcomes and prognostic factors in African American and black patients with mycosis fungoides/Sézary syndrome: retrospective analysis of 157 patients from a referral cancer center J Am Acad Dermatol 83220204304393149915710.1016/j.jaad.2019.08.073PMC 7058509 · doi ↗ · pubmed ↗
- 4Miyashiro D.Sanches J.A.Mycosis fungoides and Sézary syndrome: clinical presentation, diagnosis, staging, and therapeutic management Front Oncol 132023114110810.3389/fonc.2023.1141108 PMC 1014075437124514 · doi ↗ · pubmed ↗
- 5Kodama K.Fink-Puches R.Massone C.Kerl H.Cerroni L.Papular mycosis fungoides: a new clinical variant of early mycosis fungoides J Am Acad Dermatol 5220056946981579352610.1016/j.jaad.2004.12.018 · doi ↗ · pubmed ↗
- 6Flaum-Dunoyer P.Noor S.J.Myskowski P.L.Cutaneous lymphomas in African American/Black patients: pitfalls and presentations Int J Dermatol 62320233573683601795710.1111/ijd.16374 · doi ↗ · pubmed ↗
- 7Wilson L.D.Hinds G.A.Yu J.B.Age, race, sex, stage, and incidence of cutaneous lymphoma Clin Lymphoma Myeloma Leuk 12520122912962304043410.1016/j.clml.2012.06.010PMC 3475508 · doi ↗ · pubmed ↗
- 8Johnson W.T.Kartan S.Sokol K.Nikbakht N.Porcu P.Clinical characteristics and outcomes of black patients with mycosis fungoides and Sézary syndrome: a subgroup analysis of the phase III MAVORIC trial Leuk Lymphoma 6282021187718833361859210.1080/10428194.2021.1888376 PMC 9931803 · doi ↗ · pubmed ↗