Spontaneous Peritoneal Hemorrhage and Anemia: A Rare Case Report of Immune Thrombocytopenic Purpura
Diana M Almeida, Duarte Silva, Marta Henriques, Ricardo C Costa, Joana Azevedo

TL;DR
A 14-year-old girl with immune thrombocytopenia experienced rare spontaneous peritoneal bleeding and anemia, successfully treated with IVIG and blood transfusion.
Contribution
This case report highlights a rare complication of ITP—spontaneous peritoneal hemorrhage—and its successful management.
Findings
The patient showed severe thrombocytopenia and normocytic anemia with peritoneal hematic effusion.
Treatment with IVIG and blood transfusion led to a gradual recovery of platelet count and hemoglobin.
Spontaneous resolution of peritoneal hemorrhage occurred without further intervention.
Abstract
Immune thrombocytopenia (ITP) is characterized by isolated thrombocytopenia manifesting with mucocutaneous bleeding symptoms, generally mild to moderate. The presence of severe symptoms or complications is rare but can be life-threatening and should be promptly diagnosed and treated. We present the case of a 14-year-old female presenting with abdominal tenderness and signs of peritoneal irritation and found to exhibit petechial rash in the buccal mucosa, scant petechiae, and superficial ecchymosis in both arms and legs on physical examination. Laboratory evaluation revealed severe thrombocytopenia and normocytic anemia. Abdominal ultrasound showed a significant peritoneal hematic effusion. The diagnosis of ITP with spontaneous peritoneal hemorrhage was made, and she was treated with intravenous immunoglobulin (IVIG) and antibiotic therapy, as well as one packed red blood cell…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
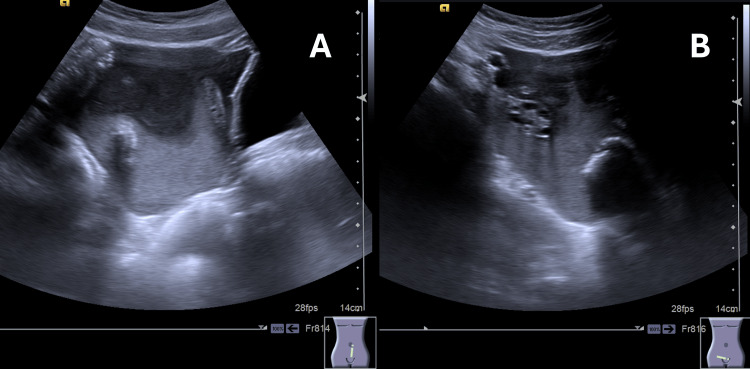 Figure 1
Figure 1| Laboratory test | Patient’s results | Reference range | Interpretation |
| Hematology | |||
| WBC count | 7.5x109/L | 4.5-13.0x109/L | N |
| Neutrophile | 4.3x109/L | 1.8-8.0x109/L | N |
| Lymphocyte | 2.5x109/L | 1.5-5.2x109/L | N |
| Monocyte | 0.4x109/L | 0.1-1.0x109/L | N |
| Eosinophil | 0.06x109/L | 0.02-0.65x109/L | N |
| Basophil | 0.1x109/L | 0.0-0.2x109/L | N |
| Erythrocytes | 2.8x1012/L | 4.1-5.1 x1012/L | L |
| Hemoglobin | 8.7 g/dL | 12.0-16.0g/dL | L |
| Hematocrit | 25.1% | 36-46% | L |
| MCV | 91 fL | 78-102 fL | N |
| MCH | 31.2 pg | 25-35 pg | N |
| MCHC | 34.7 g/dL | 31-37 g/dL | N |
| RDW | 13.4 | 11.5-15.0 | N |
| Platelets | 4x109/L | 160-400x109/L | L |
| Reticulocyte count | 92x109/L | 30-105x109/L | N |
| Blood chemistry | |||
| BUN | 10.5 mg/dL | 7-20 mg/dL | N |
| Creatinine | 0.58 mg/dL | 0.57-0.80 mg/dL | N |
| AST | 38 U/L | <31 U/L | H |
| ALT | 39 U/L | <34 U/L | H |
| CRP | 0.05 mg/dL | <0.50 mg/dL | N |
| Coagulation | |||
| Prothrombin time | 14.5 s | 10.0-14.1 s | H |
| aPTT | 32.0 s | 24.6-38.4 s | N |
| Fibrinogen | 194 mg/dL | 168-529 mg/dL | N |
| Coombs test | Negative | ||
| ADAMTS13 activity | 66% | 40-130% | N |
| Serology | |||
| Cytomegalovirus | IgG: negative; IgM: negative | No infection | |
| EBV | IgG: positive; IgM: positive | Recent infection | |
| Hepatitis B virus; hepatitis C virus | HBsAg: negative; anti-HBs: negative; anti-HBc: antibody to hepatitis B core antigen; anti-HCV: negative | No infection | |
| Human immunodeficiency virus | Anti-HIV 1 and 2: negative | No infection | |
| Laboratory test | Reference range | Days after start of therapy | |||||||
| 1 | 2 | 3 | 12 | 19 | 26 | 12 months | |||
| WBC count | 4.5-13.0x109/L | 7.3 | 7.4 | 6.3 | 5.8 | 6.5 | 12.7 | 5.9 | |
| Neutrophile | 1.8-8.0x109/L | 4.8 | 5.3 | 2.6 | 2.3 | 3.8 | 8.8 | 3.6 | |
| Lymphocyte | 1.5-5.2x109/L | 2.0 | 1.7 | 3.0 | 2.7 | 1.8 | 2.9 | 1.9 | |
| Monocyte | 0.1-1.0x109/L | 0.5 | 0.3 | 0.5 | 0.5 | 0.5 | 1.0 | 0.3 | |
| Eosinophil | 0.02-0.65x109/L | 0.01 | 0.06 | 0.04 | 0.11 | 0.26 | 0.02 | 0.12 | |
| Basophil | 0.0-0.2x109/L | 0.05 | 0.09 | 0.14 | 0.14 | 0.13 | 0.05 | 0.06 | |
| Erythrocytes | 4.1-5.1 x1012/L | 2.27 | 2.78 | 3.39 | 4.43 | 4.11 | 4.44 | 4.14 | |
| Hemoglobin | 12.0-16.0 g/dL | 7.1 | 8.7 | 10.6 | 13.7 | 12.7 | 13.9 | 12.6 | |
| Hematocrit | 36-46 % | 20.4 | 25.2 | 31.4 | 39.8 | 36.6 | 38.5 | 37.4 | |
| MCV | 78-102 fL | 90 | 90.6 | 92.6 | 89.8 | 89.1 | 86.7 | 90.3 | |
| MCH | 25-35 pg | 31.3 | 31.3 | 31.3 | 30.9 | 30.9 | 31.3 | 30.4 | |
| MCHC | 31-37 g/dL | 34.8 | 34.5 | 33.8 | 34.4 | 34.7 | 36.1 | 33.7 | |
| RDW | 11.5-15.0 | 13.3 | 13.5 | 14.6 | 12.4 | 12.1 | 12.1 | 12.1 | |
| Platelets | 160-400 x109/L | 43 | 109 | 163 | 154 | 27 | 184 | 309 | |
| Observation | Red blood cell transfusion | Prednisolone course started | |||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPlatelet Disorders and Treatments · Blood groups and transfusion · Autoimmune Bullous Skin Diseases
Introduction
Immune thrombocytopenia (ITP) is the most common acquired bleeding disorder in childhood (estimated annual incidence of one to 6.4 cases per 100000 children), characterized by isolated thrombocytopenia [1-3]. The typical presentation is the sudden appearance of mild to moderate mucocutaneous bleeding, with no other accompanying symptoms, in an otherwise healthy child or adolescent [1,2,4]. The prognosis is usually very good, with rates of 80% to 90% of complete remission in the first six months after disease onset, irrespective of the treatment [2,3,5,6]. Severe bleeding, such as mucosal bleeding or internal hemorrhage (e.g., severe gastrointestinal or genitourinary bleeding requiring immediate attention and intervention), and other potentially life-threatening conditions (e.g., intracranial hemorrhage) are rare. Nevertheless, they are major causes of mortality and should be promptly diagnosed and treated [1,3-5]. In this case report, we present the case of a 14-year-old ITP patient with a spontaneous peritoneal hemorrhage and anemia.
This article was previously presented as a Poster at the 2º Congreso Ibérico de Hematología y Oncología Pediátricas on May 25-27, 2023.
Case presentation
A 14-year-old female was brought to the emergency department with a 24-hour history of constant and dull abdominal pain in the hypogastric area, with a gradual onset and progression, with no migration, little improvement with paracetamol, and night awakening because of the pain. She had no fever or other gastrointestinal or genitourinary symptoms and denied previous trauma.
She had been diagnosed with acute tonsillitis three weeks earlier (treated with Amoxicillin and nonsteroidal anti-inflammatory drugs), but was otherwise healthy, with no chronic medications. Her menstrual cycle was regular at 28 to 30 days, and her last menstrual period had been four weeks before.
She was hemodynamically stable, with blood pressure of 98/57 mmHg, heart rate of 91 bpm, no fever, good general appearance, and no evidence of neurological impairment. No active bleeding was seen or reported (including no menstrual losses), but the physical examination was relevant for the presence of petechial rash in the buccal mucosa, scarce petechia, and superficial ecchymosis in both arms and legs, which had not been recognized as relevant by the girl and family, as well as abdominal tenderness with signs of peritoneal irritation. No palpable hepatosplenomegaly or lymphadenopathies were described.
Laboratory evaluation (Table 1) revealed severe thrombocytopenia (4x10^9^/L) and normocytic anemia (hemoglobin: 8.7 g/dL, mean corpuscular volume (MCV): 91 fL) with normal reticulocyte count and normal white blood cell count (7.5x10^9^/L). Blood smear showed no evidence of erythrocyte fragmentation or immature cells. General chemistry and coagulation evaluation were unremarkable, the Coombs test was negative, and ADMTS13 activity was 66%. Epstein-Barr virus (EBV) serology was suggestive of recent infection. The pregnancy test was negative. Abdominal ultrasound, presented in Figure 1A, 1B, revealed significant free hematic peritoneal effusion, with no other remarkable findings. The source of the bleeding was not identified.
Abdominal ultrasound revealing significant free hematic peritoneal effusion
She was given 0.8 g/kg/day of intravenous immunoglobulin (IVIG) and 1 mg/kg of methylprednisolone for two days, as well as antibiotic therapy to prevent peritonitis, and hormonal therapy to prevent severe menorrhagia. As seen in Table 2, platelets rose to 43x10^9^/L 24 hours after the beginning of IVIG infusion, but hemoglobin lowered to 7.1 g/dL, requiring packed red blood cell transfusion. Control ultrasonography documented a significant decrease of the peritoneal effusion by D4, with complete resolution in subsequent evaluations. A gradual rise in platelet count and hemoglobin normalization was observed, achieving hemoglobin of 13 g/dL and 154x10^9^/L platelets with no further therapy by D12. The girl was discharged, maintaining regular clinical and laboratory surveillance. In the third week, she was given an oral prednisolone course (initial dose of 1 mg/kg/day) after her platelet count dropped to 27x10^9^/L, with a very good response (platelet count of 184x10^9^/L one week after), allowing its uneventful weaning off and discontinuation. After 12 months, she remains asymptomatic, with no medication, and platelet count stable above 200x10^9^/L. Further investigation, including antinuclear antibodies, anti-dsDNA antibodies, extractable nuclear antigen antibodies, immunoglobulins, direct Coombs test, Helicobacter pylori test, and screening of Von Willebrand disease, was negative.
Discussion
ITP is characterized by the production of autoantibodies directed against platelet membrane antigens and their subsequent destruction [1,2,4,6]. It is more common in preschool age and in boys, but there is also a smaller peak in adolescence, characterized by a female predominance and higher prevalence of chronicity [1,3,6-8]. In approximately 60% of cases, there is a history of preceding viral illness, usually within the past month, EBV being one of the most commonly identified viruses, like in our case [1,6,7]. Vaccination against measles, mumps, and rubella is also associated with an increased risk, occurring in approximately 2.6 cases per 100,000 doses [1,6].
The symptoms are typically mild, and the child/adolescent is usually hemodynamically stable, with good appearance and no systemic signs and symptoms [1,6]. Other causes of thrombocytopenia should be considered if systemic symptoms are present, if there is a prior personal or family history of bleeding or if enlargement of lymph nodes, liver, or spleen is found [1]. Patients can also be asymptomatic, and the incidence of the disease is most likely underestimated [1].
The more common bleeding symptoms are cutaneous (“dry purpura”), like petechiae, purpura, or bruising, followed by mucosal (“wet purpura”) and, less frequently, menstrual, gastrointestinal, and urinary bleeding. Severe signs and symptoms are rare, developing in approximately 3% of children with ITP, and are related, among others, to the presence of severe thrombocytopenia (platelet count of <10x10^9^/L) [1,2,6,8].
To our knowledge, there are only a few reported cases of intra-abdominal bleeding in ITP, and these are usually related to ruptured cysts/follicles [2-4,8,9]. In this case, the source of bleeding was never identified, and she was on week four of her menstrual cycle, but the diagnosis of ruptured follicle/cyst cannot be excluded.
Thrombocytopenia (platelet count: <100x10^9^/L) is often the only abnormality detected, except in cases where significant bleeding leads to anemia. Any other laboratory findings should prompt the consideration of alternative causes [1,4,6,7,9]. In our case, the presence of anemia and abdominal pain prompted an imaging investigation, which led to the diagnosis of hematoperitoneum. In our case, anemia probably had an acute onset, in response to severe and recent peritoneal hemorrhage as the anemia was normocytic, and not microcytic with low iron stores as one would expect if the blood loss was chronic or longstanding. The normal findings obtained from additional investigations performed, coupled with the excellent response to therapy, strongly support this hypothesis over other potential diagnoses.
Supportive measures for ITP are aimed at avoiding bleeding events and rely on restriction from activities with a higher risk of bleeding/traumatic injury, avoidance of antiplatelet and anticoagulant medications (including ibuprofen, unless it is truly necessary), and control of bleeding manifestations, like menorrhagia and epistaxis [5,7]. ITP is generally a self-limiting benign disorder and patients with mild or no bleeding symptoms do not generally require admission to the hospital and can be managed in an ambulatory setting with only these measures and follow-up within 24 to 72 hours [2,5,6,10]. In cases of life-threatening bleeding, it is recommended to initiate immediate combination therapy consisting of platelet transfusion, intravenous corticosteroid, and IVIG. In severe but non-life-threatening hemorrhage, such as in our case, platelet transfusions are generally not necessary, and treatment with isolated corticosteroids or IVIG may be adequate [4,5]. Although IVIG is associated with more costs and side effects compared with corticosteroids alone, the need for a rapid increase in platelet count, given the intraabdominal bleeding, led to the use of IVIG in our case [3,5,6]. Because the platelet count dropped to less than 30x10^9^/L at two to three weeks (consistent with the known half-life of IVIG), we opted to start her on prednisolone as the initial presentation was severe bleeding and we were not able to identify the intraabdominal bleeding source. Due to the good and sustained response, prednisolone was successfully weaned off in eight weeks. She maintained a normal platelet count ever since. Surgical management of the bleeding is rarely needed, like in this case [3,9,11].
The prognosis of ITP is excellent, especially in children, with most patients recovering within three to six months from the time of presentation, regardless of instituted treatment [1,6,7,9]. In this case, the girl remained asymptomatic, with no medication after the short course of prednisolone.
Conclusions
ITP is a relatively common childhood disease characterized by isolated thrombocytopenia. It typically presents with sudden mild to moderate mucocutaneous bleeding, and the prognosis is generally good with high rates of complete remission. However, severe complications, although rare, can occur and should be promptly diagnosed and treated to prevent mortality. In this case report, we present the case of a 14-year-old ITP patient with spontaneous severe peritoneal hemorrhage that required prompt diagnosis and treatment, highlighting the importance of recognizing and managing such a rare presentation in ITP.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Immune thrombocytopenia (ITP) in children: clinical features and diagnosis Up To Date 2 2024 Bussel JB 2022 https://www.uptodate.com/contents/immune-thrombocytopenia-itp-in-children-clinical-features-and-diagnosis
- 2An extremely uncommon complication of ITP: spontaneous rupture of an ovarian follicle cyst and massive intra-abdominal bleeding J Pediatr Hematol Oncol Yilmaz S Demircioğlu F Türker M Oren H Cakmakçi H Irken G 7557562820061711496410.1097/01.mph.0000243653.41185.3f · doi ↗ · pubmed ↗
- 3Intra-abdominal bleeding in a 14-year-old girl with acute immune thrombocytopenic purpura Pediatr Hematol Oncol Mäkipernaa A Nyman R 485488121995851963410.3109/08880019509009479 · doi ↗ · pubmed ↗
- 4Massive spontaneous intraperitoneal hemorrhage in a young female with chronic immune thrombocytopenic purpura masquerading as ruptured ovarian cyst: successful nonsurgical management of this rare catastrophic event Pediatr Emerg Care Singh N Tripathi R Mala YM Tyagi S Jain N 2842853120152583103210.1097/PEC.0000000000000402 · doi ↗ · pubmed ↗
- 5Immune thrombocytopenia (ITP) in children: initial management Up To Date 2 2024 Bussel JB 2022 https://www.uptodate.com/contents/immune-thrombocytopenia-itp-in-children-initial-management
- 6Management of immune thrombocytopenic purpura in children Rev Clin Exp Hematol Gadner H 201221520011170381510.1046/j.1468-0734.2001.00040.x · doi ↗ · pubmed ↗
- 7Immune thrombocytopenia (ITP) in children: management of chronic disease Up To Date 2 2024 Bussel JB 2023 https://www.uptodate.com/contents/immune-thrombocytopenia-itp-in-children-management-of-chronic-disease
- 8Peritoneal hemorrhage due to a ruptured ovarian cyst in ITPJ Pediatr Hematol Oncol Kaplan J Bannon CC Hulse M Freiberg A 1171202920071727900910.1097/MPH.0b 013e 3180314206 · doi ↗ · pubmed ↗