Somatic Mutation Profile as a Predictor of Treatment Response and Survival in Unresectable Pancreatic Ductal Adenocarcinoma Treated with FOLFIRINOX and Gemcitabine Nab-Paclitaxel
Rodrigo Paredes de la Fuente, Santiago Sucre, Cristina Ponce, Ahmed Anwer Ali Rattani, Mary Linton B. Peters

TL;DR
This study shows that genetic mutations in pancreatic cancer can predict how well patients respond to chemotherapy and how long they survive.
Contribution
The study identifies specific genetic pathways linked to better treatment outcomes and survival in pancreatic cancer patients.
Findings
NOTCH and KIT pathway mutations are associated with longer survival in patients receiving FOLFIRINOX or gemcitabine nab-paclitaxel.
PI3K and KIT pathway mutations correlate with improved progression-free survival in the gemcitabine nab-paclitaxel subgroup.
Combinatorial pathway analysis suggests synergistic effects on survival outcomes.
Abstract
This study explored how genetic changes influence treatment effectiveness and survival in patients with advanced pancreatic cancer. By examining tumors from 142 patients, researchers identified specific genetic mutations that can predict how well a patient responds to chemotherapy. Findings showed that mutations in certain genetic pathways are associated with longer survival and better treatment outcomes. This research highlights the importance of tailoring cancer treatment based on individual genetic profiles, potentially leading to more personalized and effective therapies for pancreatic cancer patients. (1) Background: Pancreatic ductal adenocarcinoma (PDAC) has low survival rates despite treatment advancements. Aim: This study aims to show how molecular profiling could possibly guide personalized treatment strategies, which may help improve survival outcomes in patients with PDAC.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
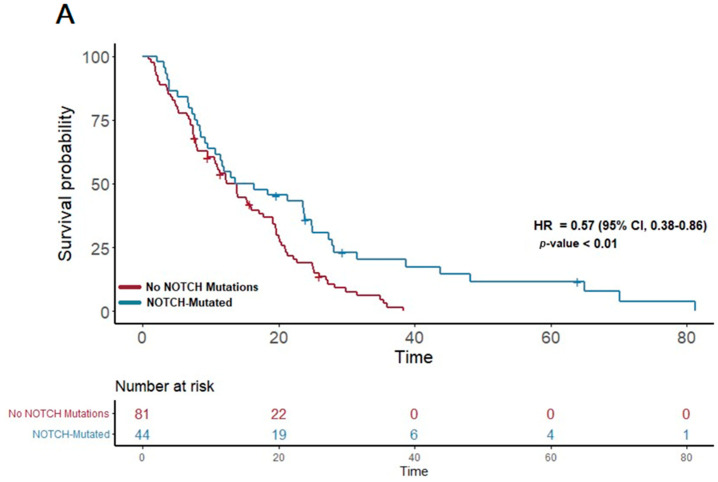 Figure 1
Figure 1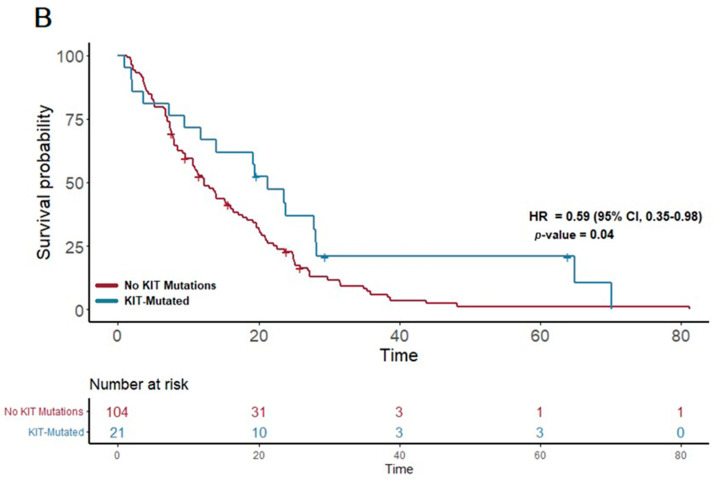 Figure 2
Figure 2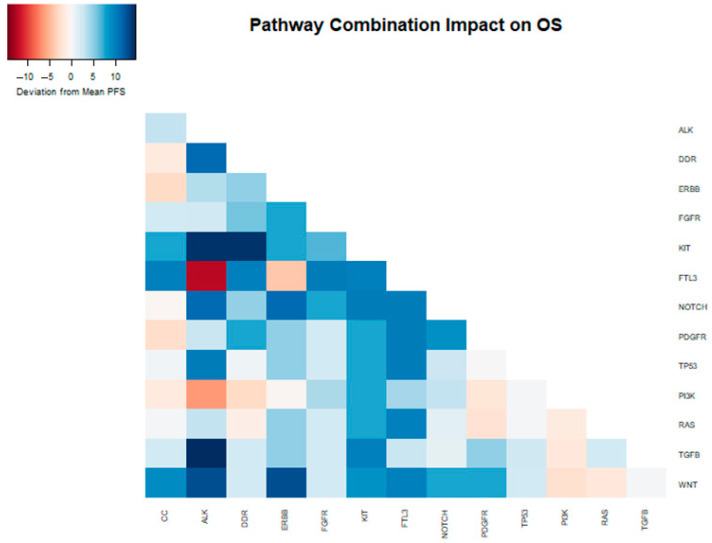 Figure 3
Figure 3 Figure 4
Figure 4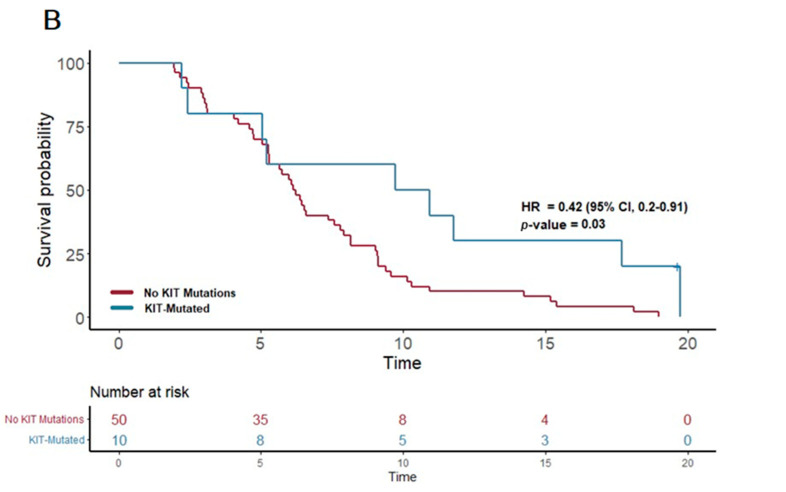 Figure 5
Figure 5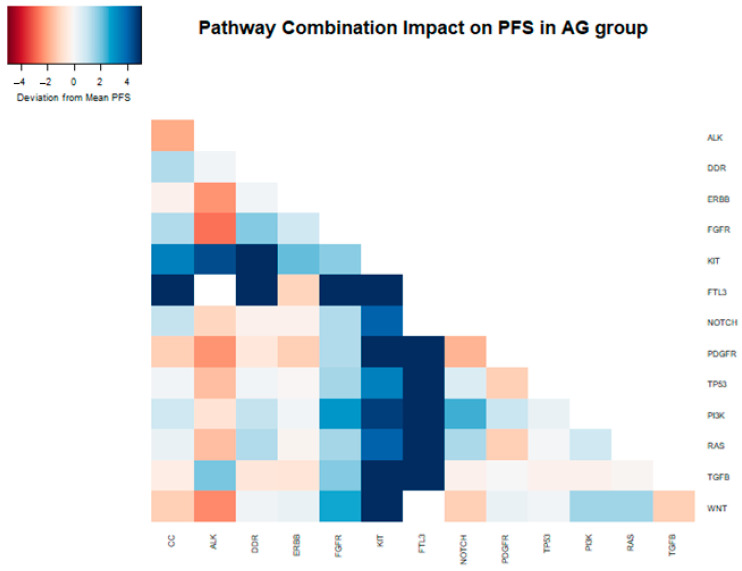 Figure 6
Figure 6- —National Cancer Institute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Cancer Genomics and Diagnostics · Renal cell carcinoma treatment
1. Introduction
Pancreatic cancer presents a significant challenge as it is the third-leading cause of cancer-related deaths [1], with a rising incidence that is expected to make it the second-leading cause by 2030 [2]. Despite advancements in therapy, the 5-year survival rate remains low at 11.5% [3]. While surgical resection offers a curative option, it is feasible for only a small percentage of patients because this cancer often presents at an advanced stage, limiting the potential for curative interventions. [4,5]. Despite extensive study, immune–oncology agents have had little benefit in pancreatic ductal adenocarcinoma (PDAC), and targeted treatment based on molecular pathological tumor characteristics has yet to be as broadly beneficial as they have been in other tumor types [6]. Aggressive cytotoxic chemotherapy remains the primary treatment option for unresectable pancreatic tumors, despite its relatively low response rate [7]. Treatment regimens for PDAC vary based on the patient’s performance status [8]. FOLFIRINOX, which includes infusional 5-fluorouracil, leucovorin, irinotecan, and oxaliplatin, is preferred for patients with good performance status (ECOG 0-1) due to its superior efficacy compared to gemcitabine alone. For patients with a slightly lower performance status (ECOG 1-2), the combination of gemcitabine plus nab-paclitaxel is another frontline option.
PDAC exhibits significant molecular heterogeneity, with an average of from 60 to 70 genetic changes observed [9]. Efforts have been made to categorize pancreatic cancer based on molecular activity and phenotypical aspects. However, due to the complexity of the disease, a consensus has not been reached [10,11,12,13,14]. Nonetheless, profiling studies have identified potentially actionable molecular alterations in up to 25% of pancreatic cancers [15]. The advent of next-generation sequencing (NGS) has revolutionized genomic profiling and made it widely accessible, and it plays a crucial role in pancreatic cancer research and clinical decision-making [16,17,18]. Leveraging NGS technology can lead to a more comprehensive understanding of the molecular landscape of pancreatic cancer, paving the way for improved treatments and future advancements in the field [11].
In this study, we retrospectively examined the molecular profiles of unresectable PDAC patients, aiming to elucidate the relationship between specific genetic alterations, natural history of disease, and treatment responses. Our focus was on understanding how the presence of mutations in key oncogenic pathways might influence the overall survival and efficacy of first-line chemotherapy regimens, such as FOLFIRINOX and gemcitabine nab-paclitaxel. By integrating molecular data with clinical outcomes, this study seeks to contribute to the burgeoning field of precision oncology, offering insights into personalized treatment strategies that could potentially improve survival and quality of life for patients with this formidable disease.
2. Materials and Methods
This study is a retrospective chart review designed to investigate the role of molecular profiling in predicting treatment response and survival in patients with unresectable pancreatic ductal adenocarcinoma.
Study Population: The study population consisted of patients diagnosed with PDAC who presented to the medical oncology clinic of a single center (Beth Israel Deaconess Medical Center, Boston MA) between the years 2013 and 2022. Only those patients with next-generation tumor sequencing who underwent cytotoxic chemotherapy were selected for inclusion. The sample size was calculated to ensure a power of 0.80 and a significance level of 0.05. Patients who were included followed these characteristics: diagnosed with unresectable PDAC (Stage III or IV) [19], underwent NGS for molecular profiling, and received first-line systemic cytotoxic chemotherapy (FOLFIRINOX or gemcitabine nab-paclitaxel). Of those, we obtained a sample of 142 patients.
Data Collection: A targeted chart review was performed which captured demographic information, age at diagnosis, performance status at diagnosis, tumor histology, and first-line chemotherapy regimen. Although we captured all first-line chemotherapy regimens, most patients received standard-of-care treatment with either FOLFIRINOX [20,21] or gemcitabine nab-paclitaxel [20,22]. Disease progression was assessed using the Response Evaluation Criteria in Solid Tumors (RECIST) criteria, as determined by provider documentation [23].
Molecular Profiling: The genetic profile of each tumor sample was obtained through next-generation tumor sequencing using the Foundation Medicine CDX Report [24]. This analysis includes 324 genes that are potentially cancer-related, of which 225 were altered in at least one sample within our selected patient population. These genes were grouped into 14 different pathways (Appendix A) based on their biological function using the Reactome Pathway database [25]; some genes may be members of multiple pathways. Each patient sample was classified by the altered genes present, and then by the pathways represented by those mutations. We recorded whether mutations were present in these pathways as a binary yes-or-no variable. Any insertion, deletion, substitution, duplication, rearrangement, truncation, or amplification was considered a mutated state [26]. All data were collected and managed using REDCap electronic data capture hosted at Beth Israel Deaconess Medical Center [27,28]. This study was approved by the BIDMC IRB and determined to be exempt from informed consent requirements.
Statistical Analysis: We conducted two distinct survival analyses based on the presence or absence of specific mutated pathways: overall survival and progression-free survival. We performed a sub-group analysis of the patients who received FOLFIRINOX or gemcitabine nab-paclitaxel as a first-line therapy. We used Kaplan–Meier curves and log-rank tests to compare survival between groups with and without each specific mutated pathway. We also performed a Cox Proportional Hazards Regression analysis to adjust for potential confounding variables. The threshold for statistical significance was set at p < 0.05. All analyses were performed using R Statistical Software (v4.2.2; R Core Team 2021) via the survival package [29,30].
3. Results
3.1. Characteristics of the Patient Population
This study included 142 patients with a median age of 66 years who were balanced in gender (49% male, 51% female). Most patients were diagnosed at advanced stages (37% Stage III, 63% Stage IV). The majority underwent standard first-line chemotherapy, with equal distribution between FOLFIRINOX (44%) and gemcitabine nab-paclitaxel (44%) (Table 1).
3.2. Characteristics of the Pathology Samples
The majority of samples were tissue samples obtained from the primary tumor (68, 48%) or a metastatic site (68, 48%), while a small number were from peripheral blood (6, 4%). Tumor mutation burden (TMB) status was known for 110 patients, with a median value of 2.5 (IQR 1.3–3.8), and 4 patients classified as TMB-High. MSI status was known for 140 patients, with 1 classified as MSI-H.
The comprehensive genomic analysis of the 142 PDAC patient samples revealed a significant degree of mutational burden, with an average of 7.83 mutations per sample, ranging from 1 to 35 mutations. Predominantly, mutations were observed in the MAPK-RAS pathway in 94% of patients (n = 134) and the TP53 pathway in 87% (n = 123). Other frequently altered pathways included the Cell Cycle (CC) pathway in 76% of patients (n = 108), DNA Damage Repair (DDR) in 49% (n = 70), TGF-beta pathway in 46% (n = 65), PI3K pathway in 37% (n = 52), and NOTCH pathway in 36% (n = 51). Less commonly altered pathways comprised FGFR (23%, n = 32), WNT (20%, n = 29), PDGFR (18%, n = 25), KIT (16%, n = 23), ERBB2 (14%, n = 20), ALK (13%, n = 19), and FTL3 (6%, n = 9). These findings highlight the extensive molecular diversity present in PDAC and underscore the potential for targeted therapeutic strategies based on individual mutational profiles.
3.3. Overall Survival Analysis
In our study cohort, the median overall survival (OS) was found to be 13.6 months. A detailed analysis of the genetic profiles revealed significant survival advantages in specific mutational pathways. Notably, patients exhibiting mutations in the NOTCH pathway (n = 51) demonstrated a median OS of 15 months, markedly longer than the 12.3 months observed in those without NOTCH mutations (p = 0.007; HR 0.57; 95% CI 0.38–0.86) (Figure 1A). This suggests a potential protective effect of NOTCH pathway alterations on survival.
Furthermore, a similar trend was observed in the KIT pathway mutations. Among the 23 patients with KIT pathway mutations, the median OS was significantly extended to 21.3 months, compared to 12.12 months in patients without these mutations (p = 0.04; HR 0.59; 95% CI 0.35–0.98) (Figure 1B). This finding suggests a notable survival benefit associated with KIT pathway alterations.
In contrast, other individual pathways did not show a statistically significant association with OS in our cohort. However, an interesting non-significant trend towards improved OS was noted in patients with mutations in the ALK pathway, where the median OS was 16.7 months compared to the overall cohort median of 13.6 months (p = 0.06, HR = 0.57, 95% CI 0.32–1.03). This observation warrants further investigation to elucidate the potential role of ALK pathway mutations in PDAC survival.
We further tested all two-way combinations of mutations among the 14 pathways. In the two-way combination analysis (Table 2 and Figure 2), mutations in the ALK, KIT, ERBB2, and PDGFR pathways could be synergistic with NOTCH, showing increases in overall survival (median OS of 25, 24, 25, and 23 months vs. 15 months for NOTCH overall). Combinatoric analysis with the KIT pathway revealed a potentially negative effect of combination with the DDR pathway (median OS of 11 months vs. 21 months for KIT overall). Although the ALK pathway overall did not show a statistically significant increase in OS, in combination with TGFB (median OS 28 months) and TP53 (median OS 24 months) it did achieve significance in the combination analysis.
3.4. Progression-Free Survival Analysis
In our study, we examined the progression-free survival (PFS) among the 142 patients with PDAC, specifically analyzing differences in PFS based on first-line chemotherapy regimens and genetic mutations. The median PFS for patients treated with FOLFIRINOX (n = 62) was 9.1 months, while those receiving gemcitabine nab-paclitaxel (n = 62) had a median PFS of 6.3 months.
For the FOLFIRINOX cohort, the analysis did not reveal any significant correlation between the presence of specific mutational pathways and improvements in PFS. Even with the exploration of potential two-way interactions between different pathways, no statistically significant results emerged that suggested a benefit in PFS from combined mutations in the FOLFIRINOX-treated group.
In contrast, the patients treated with gemcitabine nab-paclitaxel exhibited notable associations between certain genetic alterations and PFS. Notably, the presence of a PI3K pathway mutation (found in 25 patients) was associated with a significantly extended PFS of 6.6 months, compared to 5.7 months in patients without such mutations (p = 0.03; HR = 0.54, 95% CI 0.31–0.93). Furthermore, mutations in the KIT pathway (observed in 10 patients) correlated with an even more substantial increase in PFS, reaching 10.3 months versus 6.2 months in non-mutated cases (p = 0.03; HR 0.42, 95% CI 0.2–0.91). Additionally, mutations in the FTL3 pathway (n = 4) were linked to the longest median PFS of 13.3 months, a significant improvement compared to 6.2 months in those without FTL3 mutations (p = 0.02; HR 0.21, 95% CI 0.05–0.89).
These results highlight the potential of certain genetic mutations, particularly within the PI3K, KIT, and FTL3 pathways, to predict longer progression-free survival in PDAC patients receiving gemcitabine nab-paclitaxel as their first-line treatment. (Figure 3) This insight underscores the value of molecular profiling in guiding therapy choices and tailoring treatment strategies to individual patient profiles.
In a two-way combination analysis, these three pathways (PI3K, KIT, and FTL3) could be synergistic for response to gemcitabine nab-paclitaxel, with a longer PFS in combination (PI3K + KIT 10.9 months, PI3K + FTL3 13.1 months, KIT + FTL3 19.7 months). In addition, DDR pathway mutations in combination with KIT or FTL3 (but not PI3K) appeared to provide additional PFS benefits (DDR + KIT 14.7 months, DDR + FTL3 19.7 months) (Table 3 and Figure 4).
4. Discussion
Our study aimed to comprehensively investigate the molecular profiles and clinical characteristics of patients with PDAC. We placed particular emphasis on identifying potential predictive biomarkers and evaluating their significance in treatment selection and outcomes. This analysis consisted of 142 PDAC patients, with a relatively equal gender distribution and a median age of 66 years. In line with current treatment guidelines, the most frequently administered first-line chemotherapy regimens in our cohort were gemcitabine nab-paclitaxel and FOLFIRINOX [20]. Within our study, a small subset of patients exhibited TMB-H or MSI-H characteristics, a known characteristic that contributes to the limited efficacy of immunotherapy in pancreatic cancer [31,32,33,34].
In the current study, tumors with NOTCH-mutated pathways exhibited a longer OS compared to tumors without mutations in the NOTCH pathway. The role of NOTCH signaling in pancreatic cancer is complex and context-dependent. It appears to have both oncogenic and tumor-suppressive functions, with different NOTCH receptors playing distinct roles [35,36,37]. Individual NOTCH receptors can exhibit opposing activities and lead to diverse cellular responses [38]. Furthermore, NOTCH signaling is intricately intertwined with other signaling pathways and mechanisms, further complicating our understanding of its involvement in oncogenic processes [39,40]. The NOTCH signaling pathway has emerged as a crucial regulator in triggering epithelial-to-mesenchymal transition (EMT) [41], a transformative process that intensifies tumor aggressiveness by enhancing cellular motility and metastatic potential [42]. In addition, the NOTCH pathway has been linked to chemotherapy resistance in tumors [43,44], and therapeutic interventions targeting the NOTCH signaling pathway have shown potential for reversing chemoresistance [45]. We did not see a PFS difference between groups in our study. Interestingly, in our cohort, this improvement in OS with NOTCH-mutated pathways persisted even when combined with other mutated pathways such as TP53, which are typically associated with poor prognosis [46,47].
The consistent superior performance of NOTCH-mutated pathways raises intriguing questions. Some studies have proposed that highly mutated NOTCH samples exhibit significantly enhanced immunogenicity and immune response [48]. Additionally, other studies have suggested that the specific genes mutated within the NOTCH pathway may also play a role in determining prognosis [49]. The therapeutic targeting of the NOTCH pathway has been investigated in various trials using medications that globally inhibit the pathway [50,51]. However, other studies [52,53] suggest that the therapeutic targeting of the NOTCH pathway may be more complex than initially believed. The prognostic and predictive implications of NOTCH pathway mutations, as well as the potential targeting of this pathway for therapeutic benefit, will be a topic of substantial interest.
In our cohort, we identified a more favorable OS and PFS in samples exhibiting mutations within the KIT pathway. Furthermore, our findings indicate a synergistic effect as the combined presence of NOTCH and KIT mutations was associated with significantly prolonged OS compared to the analysis of these mutations individually. While the existing knowledge on pancreatic cancer is limited, certain studies have suggested that KIT may serve as a valuable prognostic marker for favorable outcomes in specific solid tumors [54]. However, the majority of available evidence suggests KIT as a marker for poorer prognosis [55,56]. Conversely, ALK has been proposed as a potential biomarker for favorable prognosis in lung cancer [57]. Although our results align with this finding, the understanding of ALK’s role in pancreatic cancer prognosis remains constrained due to limited data. Lastly, we observed that PI3K mutations were associated with improved PFS compared to samples lacking such mutations. Despite disappointing evidence regarding its therapeutic targeting [58], PI3K has been shown to interact with other pathways and influence survival outcomes [59].
Finally, this analysis highlights the potential role of chemotherapy selection, specifically noting that gemcitabine nab-paclitaxel may exhibit better performance in the presence of certain mutation pathways. Platinum-based therapy has been recognized for its effectiveness in tumors with homologous combination defects [60]. However, there is limited clinical data available for gemcitabine or taxanes in this context [61]. To predict in vivo tumor response to treatment, several studies have utilized PDX and organoid models [62], where the mutational profile serves as a readily available tool. This hypothesis-generating information suggests that mutational profile analysis should be considered for inclusion in future clinical trials.
This study has several limitations that should be taken into account when interpreting the findings. Firstly, the retrospective study design introduces inherent limitations. Data collected retrospectively from chart reviews may be influenced by biases and limitations in data availability, quality, and completeness. Secondly, this study’s single-center nature restricts the generalizability of the results. Moreover, this study’s sample size is relatively small, and the presence of missing data for OS or PFS analysis, as well as the subdivision of patients by treatment, further reduced the sample size. This limited sample size may affect the statistical power and precision of the findings. Finally, it is important to acknowledge that the genetic analysis was based on pathways that grouped several genetic mutations, thus limiting the scope of the analysis. This approach may have overlooked important genetic alterations that could specifically impact treatment response and survival. A more comprehensive and broader genetic profiling approach may provide additional insights into the study’s subject matter.
5. Conclusions
These findings contribute to our understanding of the clinical characteristics and treatment patterns of pancreatic cancer patients and highlight the potential for personalized treatment approaches based on molecular profiling. The integration of molecular profiling, such as next-generation sequencing, holds great promise for identifying actionable targets and guiding personalized therapeutic approaches in PDAC. However, further studies are needed to validate these findings and determine their clinical implications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel R.L. Giaquinto A.N. Jemal A. Cancer statistics, 2024 CA Cancer J. Clin.2024741249 Erratum in CA Cancer J. Clin. 2024, 74, 20310.3322/caac.2183038230766 · doi ↗ · pubmed ↗
- 2Rahib L. Smith B.D. Aizenberg R. Rosenzweig A.B. Fleshman J.M. Matrisian L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States Cancer Res.2014742913292110.1158/0008-5472.CAN-14-015524840647 · doi ↗ · pubmed ↗
- 3Cronin K.A. Scott S. Firth A.U. Sung H. Henley S.J. Sherman R.L. Siegel R.L. Anderson R.N. Kohler B.A. Benard V.B. Annual report to the nation on the status of cancer, part 1: National cancer statistics Cancer 20221284251428410.1002/cncr.3447936301149 PMC 10092838 · doi ↗ · pubmed ↗
- 4Maloney S. Itchins M. Arena J. Sahni S. Howell V.M. Hayes S.A. Gill A.J. Clarke S.J. Samra J. Mittal A. Optimal Upfront Treatment in Surgically Resectable Pancreatic Cancer Candidates: A High-Volume Center Retrospective Analysis J. Clin. Med.202110270010.3390/jcm 1012270034207372 PMC 8235361 · doi ↗ · pubmed ↗
- 5Chhoda A. Vodusek Z. Wattamwar K. Mukherjee E. Gunderson C. Grimshaw A. Sharma A. Ahuja N. Kastrinos F. Farrell J.J. Late-stage pancreatic cancer detected during high-risk individual surveillance: A systematic review and meta-analysis Gastroenterology 202216278679810.1053/j.gastro.2021.11.02134813861 · doi ↗ · pubmed ↗
- 6Sarantis P. Koustas E. Papadimitropoulou A. Papavassiliou A.G. Karamouzis M.V. Pancreatic ductal adenocarcinoma: Treatment hurdles, tumor microenvironment and immunotherapy World J. Gastrointest. Oncol.20201217318110.4251/wjgo.v 12.i 2.17332104548 PMC 7031151 · doi ↗ · pubmed ↗
- 7Principe D.R. Underwood P.W. Korc M. Trevino J.G. Munshi H.G. Rana A. The Current Treatment Paradigm for Pancreatic Ductal Adenocarcinoma and Barriers to Therapeutic Efficacy Front. Oncol.20211168837710.3389/fonc.2021.68837734336673 PMC 8319847 · doi ↗ · pubmed ↗
- 8De Dosso S. Siebenhüner A.R. Winder T. Meisel A. Fritsch R. Astaras C. Szturz P. Borner M. Treatment landscape of metastatic pancreatic cancer Cancer Treat. Rev.20219610218010.1016/j.ctrv.2021.10218033812339 · doi ↗ · pubmed ↗