Quality of Life in Palliative Care: A Systematic Meta-Review of Reviews and Meta-Analyses
Mauro Demuro, Elisa Bratzu, Stefano Lorrai, Antonio Preti

TL;DR
This study reviews existing research to evaluate how quality of life is measured and improved in palliative care, finding that it is often understudied and inconsistently measured.
Contribution
The paper provides a comprehensive meta-review of recent systematic reviews and meta-analyses on quality of life in palliative care.
Findings
Quality of life is often a secondary outcome in palliative care studies.
Lower quality studies are more likely to report efficacy of palliative care in improving quality of life.
There is a lack of standardized tools for measuring quality of life in palliative care.
Abstract
The area of palliative care is a setting in which the evaluation of the quality of life (QoL) is fundamental. However, the topic has been covered from many different points of view, and there is a lack of comprehensive synthesis of the evidence drawn from the available literature. We carried out a meta-review of all available systematic reviews and meta-analyses that have dedicated part or most of the investigation to the assessment of QoL in palliative care to provide the most updated and comprehensive depiction of all available information about measurement and intervention aimed at improving QoL in palliative care. A meta-review of all recent (5 years) available systematic reviews and meta-analyses on “palliative care” and “quality of life” was carried out. The quality of the extracted studies was assessed with the AMSTAR scale. The search extracted 24 systematic reviews, 14…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
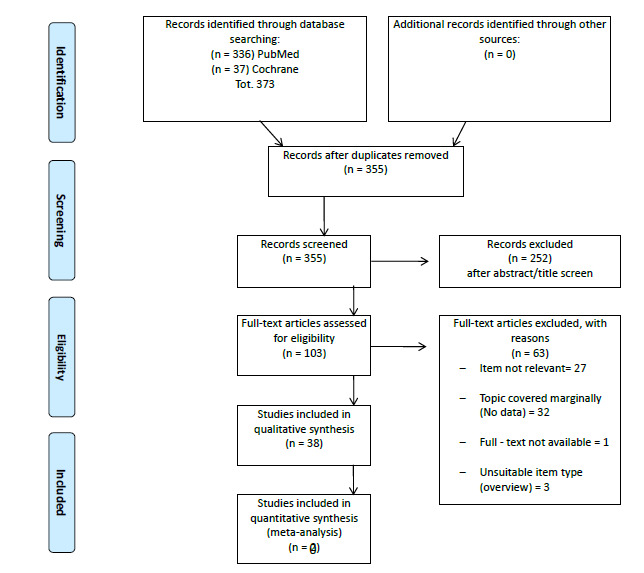 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCultural Identity and Representation · Folklore, Mythology, and Literature Studies · Gender and Women's Rights
INTRODUCTION
1
The World Health Organization Quality of Life (WHOQOL) group in 1995 defined quality of life (QoL) as “the perception that individuals have of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns”. Six fundamental domains or key aspects of QoL were proposed: physical well-being, psychological well-being, level of independence, social relationships, environment, personal beliefs, and/or spirituality. However, so far, the scientific community still struggles to find a concordant definition, as the concept of QoL is wide and subjective. Some believe in a limited set of concepts: QoL is a subjective construct, or it must be evaluated by the subject. It is multidimensional and dynamic; thus, it may change based on time and circumstances, and finally, it is related to the culture of the subject. Despite some inconsistencies, the construct of QoL is important for clinical purposes. The QoL assessment allows us to quantify the impact of the patients’ clinical condition and their possible treatment on the most varied aspects of their life.
Nevertheless, the evaluation of QoL is a complex subject, which includes a great heterogeneity of tools with considerable methodological and statistical difficulties. General purposes tools and specific measures were developed to tailor QoL in selected samples of patients, such as those with cancer or chronic diseases. A detailed description of the tools used in the studies that were reviewed in the present meta-review is reported further in the given Table.
The area of palliative care is a setting in which the evaluation of the QoL is fundamental. The WHO defines palliative care as an approach capable of improving “the quality of life of patients and their families, who are faced with the problems associated with incurable diseases, through prevention and relief of suffering through early identification and optimal treatment of pain and other problems of a physical, psychosocial, and spiritual nature” (World Health Organization, National Cancer Control Programs. Policies And Managerial Guidelines, 2002, p. 84) [1]. The term “palliative” indicates that the intervention does not act on the cause of the disease (etiological therapy) but acts to relieve refractory symptoms, therefore the suffering and the problems related to the pathology. There is a wide and varied dissemination of studies about QoL in palliative care. However, the topic has been covered from many different points of view, and there is a lack of comprehensive synthesis of the evidence drawn from the available literature. Moreover, a still-controversial topic concerns the role of Health-Related QoL (HRQoL) in terminal or permanently disabling diseases, which are among the major causes of discomfort and poor QoL and are often treated in palliative care when the etiologic cure is no more effective.
We carried out a meta-review of all available systematic reviews and meta-analyses that have dedicated part or most of the investigation to the assessment of HRQoL in palliative care with special reference to the most widespread terminal or permanently disabling diseases. The main goal of this meta-review is to provide the most updated and comprehensive depiction of all available information about measurement and intervention aimed at improving the HRQoL in palliative care.
METHODS
2
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [2]. Available literature was explored with a search in PubMed/Medline (https://pubmed.ncbi.nlm.nih.gov/) and the Cochrane Library (https://www.cochranelibrary.com/). The most recent articles were searched, with an interval from 1^st^ January, 2015 to 31^st^ December, 2020. The simplest combination of keywords was used to increase the comprehensiveness of the search: “palliative care” and “quality of life”. Articles were included when they were written in English, were published in peer-review journals, and detailed the results of a systematic review or a meta-analysis. No limitation on age, sex, religion, or geographic origin was applied to the search. Three independent researchers (MD, EB, and SL) cross-checked the reports found in the search results, checking for the title, abstract, and text to confirm their eligibility. Each step of inclusion/exclusion was supervised by a fourth experienced researcher (AP).
The search retrieved 373 articles; 18 articles were excluded as duplicates. From the remaining 355 articles, 252 articles were eliminated based on their title/abstract since they were not a systematic review or a meta-analysis or were not congruent with the topic of the search. The remaining eligible 103 were inspected in full text; a total of 63 were excluded because they were not relevant to the research, the topic was mentioned only marginally, the full text was not available, or they were not articles. Overall, 40 articles were found to be suitable for qualitative assessment and data extraction (Fig. 1).
The extracted articles were inspected for references of each review suitable for inclusion, and the procedure was repeated for each new potential review. No suitable additional reference was found.
From each article, data of interest were extracted by three investigators under the supervision of an independent fourth investigator. The extracted data were organized in a table in chronological order by setting every single article from the oldest to the most recent and grouping the information into the following fields:
1: Type of study (systematic review or meta-analysis),
2: Geographic location of the studies included in the systematic review or meta-analysis,
3: Characteristics of the included samples,
4: Medical condition under investigation,
5: Diagnosis,
6: Evaluation tools for the assessment of QoL and
7: Main findings.
Table 1 lists the details concerning the main charac-teristics and findings of the included systematic reviews and meta-analyses.
The potential risk of bias was assessed with the AMSTAR scale [3, 4]. For this study, the articles were evaluated according to the following rule: any “yes” was scored 1; instances of “no” or “cannot say” were scored 0. The articles that received a global score of 1 to 6, 7 to 9 and 10 to 11 were evaluated, respectively, as “Unaccep-table,” “Acceptable,” and “High Quality” articles. Articles that received a score of 0 were rated as “Rejected” and consequently excluded from the search, just like articles that scored 1 to 6 (Unacceptable) (Table 2).
RESULTS
3
The included 40 articles were: 23 systematic reviews [5-27], 15 systematic reviews completed with a meta-analysis [28-41], and 2 meta-analyses [42, 43].
Sample Size and Characteristics of the Included Studies
3.1
The results obtained relating to QoL were often extrapolated from the selected articles since not all research had QoL as the main topic. For this reason, we carefully analyzed each search to minimize the possibility of entering incorrect data in the results. The largest sample size was found in a study by Diop et al. [32], with 24,403 participants, while the smaller one was found in a study by Abdel-Rahman et al. [21]. It should be noted that a few articles reported no sample size information or data (Table 1).
Regarding geolocation, the articles included results from different countries; most studies were conducted in North America, Europe, and China and less frequently in Central and South America, Australia, South Africa, Israel, Japan, and the former Soviet Union.
Evaluation Tools for the Assessment of the QoL
3.2
Most articles reported the evaluation tools that were used to assess QoL (Table 3).
The most frequently assessed dimensions were the mental, physical, and functional health status, while the measurement tools only aimed at the assessment of the physical health status were rarely used, and many studies did not report QoL results about this dimension. Several tools were also found for measuring QoL in patients with specific pathologies, tools for measuring QoL in pediatric patients, and tools for measuring QoL of families or staff caring for the patient in palliative care or in the hospital.
The most commonly administered questionnaires were the EORTC-QLQ (various versions), SF-36, MQOL, and EUROQOL EQ-5D. Several studies did not directly report the measurement tools used but only the data.
Quality of the Assessment Tools and Risk of Bias
3.3
It was found that there were problems in the reliability of the results due to the high mortality of patients, often due to pathology or other complications, and therefore, in many studies, there was a lack of follow-up. This problem, leading to the loss of critical information, was found in most articles dealing with terminal illnesses, and many of these studies reported the data as “statistically significant but not clinically relevant” due to the risk of bias.
Disorders and Pathologies
3.4
In the included articles, we found various pathologies and carefully selected those that exclusively concerned the possibility of receiving treatments that include palliative care. Of these, we distinguished 2 categories, terminal pathologies and permanently disabling pathologies (both respect the standards of the study of QoL in palliative care). The first group included tumors, cardiac arrest, HIV / AIDS, and a combination of them (multiple tumors, cardiac arrest associated with tumors, etc.). The chronic diseases included multiple sclerosis, chronic obstructive pulmonary disease, Parkinson's disease, chronic pruritus, hemodialysis, dyspnea, and chronic kidney disease.
Treatments
3.5
Many treatments have been proposed in the studies, all related to palliative care.
Of these, 5 used a placebo in the control group [9, 10, 12, 14, 33], 4 had a control group without palliative care [6, 8, 17, 32], and the remaining ones had specific therapies versus the lack of them in the control.
Among the prescribed therapies, there were:
Protocols Based on the Administration of Drugs or Integrators
3.5.1
-
Administration of vitamins,
-
Administration of minerals,
-
Administration of proteins,
-
Administration of morphine or other opioids,
-
Checkpoint inhibitor therapy.
Protocols Based on Psychosocial Interventions
3.5.2
-
Psychotherapy,
-
Music therapy,
-
Acupuncture,
-
Mindfulness,
-
Exercise.
Protocols Focused on the Oncological Treatment of the Patient
3.5.3
-
Radiofrequency ablation (RFA/Rhizotomy),
-
Delayed chemotherapy,
-
Surgery combined with chemo and radiotherapy.
Special Treatment Protocols
3.5.4
-
Parenteral nutrition,
-
Paracentesis.
More Advanced Protocols of Care
3.5.5
-
Advanced care plans (multiple or combined palliative care protocols),
-
Hospitalization or home hospitalization,
-
Multidisciplinary palliative care.
Only a minority of these protocols were tested for effectiveness, either via comparisons between patients with and without palliative care or measuring differences between treatments administered independently or with the support of medical staff. Indeed, only 5 out of 40 articles reported no information on the control group [7, 30, 13, 38, 40], and only the last two studies reported numerical data concerning QoL.
These treatments produced improvements that vary between zero, minimal and discrete in several sub-categories that were cited in the results of the articles reviewed. Only 27 of the 40 articles reported numerical data regarding the results of the studies that were carried out; the remaining 13 studies reported a description of the results but no numerical data, and of these, only 4 reported the impossibility of arriving at a valid result due to “high attrition rate in the measurement of quality of life due to patient death” [22], “lack of focus and content analysis” [18], or because “the heterogeneity of QoL assessments makes direct comparisons difficult” [16].
When some improvement was reported, it concerned various dimensions of HR-QoL, in particular, physical, emotional, cognitive, mental, spiritual, social, vitality, general health, self-efficacy and optimism, personal autonomy, concerns about the quality of life, purpose in life, health care, and pain reduction (Table 1).
DISCUSSION
4
The investigation of QoL is essential to understand the aspects (physical, mental, or functional) that are most affected in patients accessing palliative care and to better understand how to deal with them. This area of investigation is understudied despite being a relevant topic in evaluating the usefulness of palliative care in terminal patients. In many studies, the investigation of QoL represents a secondary or even marginal outcome. In most studies, the most relevant improvements concern the mental or functional aspects and, to a lesser extent, the physical ones.
The most noticeable improvements in HRQoL were especially in the studies comparing palliative care versus control groups without palliative care, with common medical treatments or without any treatment, supporting the theory on the efficacy of palliative care in relation to the conditions of terminal patients or patients with permanent disability [5, 6, 8, 11, 32, 33, 14, 34, 17, 42].
Some specific treatment was found to improve QoL in special groups of patients. For example, Rosian et al. reported in their study a noticeable improvement in bone pain in patients with metastatic cancer undergoing rhizotomy. An improvement in general QoL was reported by Burlacu et al. [44] in dying patients experiencing some sort of religious beliefs. They found fewer symptoms of depression and a lower risk of suicide in relation to a positive correlation with hope and spirituality, thus linking religiosity with a possible association with better mental health [44]. According to this study, there could be a strong correlation between religiosity and QoL improvement. Overall, improvement in QoL was more likely for medical or psychosocial protocols applied to patients with cancer, while other terminal conditions accessing palliative care were less likely to benefit from the administered protocols of care. This is an area in need of better trials, especially trials that test the proposed treatment against adequate control groups. There is a shortage of RCTs as far as QoL in palliative care is concerned.
It should be noted that the quality of the studies had a strong influence on the chance that some improvement in QoL was found in relation to palliative care. Based on the quality assessment and the results reported by the studies that received an excellent rating (25 studies with ++ scoring), there was a significant improvement in 20% of the reviewed studies, a non-significant improvement in 60%, and no improvement in 20%. Of the studies that received a positive but not excellent evaluation (25 studies), 40% of the studies reported a significant improvement, 33.3% reported a non-significant improvement, and 33.3% stated no improvement.
CONCLUSION
Overall, the investigation of QoL in palliative care remains understudied. In many studies, QoL is a secondary outcome, and there is some tendency to use a disparate range of tools to measure it, whose reliability and validity should still be established in some groups of patients. There is some evidence that patients undergoing palliative care may benefit from it as far as QoL is concerned, especially in mental and functional areas.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National cancer control programmes : Policies and managerial guidelines,2nd ed. World Health Organization Genève 2002 Available from: https://apps.who.int/iris/handle/10665/42494
- 2Page M.J. Mc Kenzie J.E. Bossuyt P.M. Boutron I. Hoffmann T.C. Mulrow C.D. Shamseer L. Tetzlaff J.M. Akl E.A. Brennan S.E. Chou R. Glanville J. Grimshaw J.M. Hróbjartsson A. Lalu M.M. Li T. Loder E.W. Mayo-Wilson E. Mc Donald S. Mc Guinness L.A. Stewart L.A. Thomas J. Tricco A.C. Welch V.A. Whiting P. Moher D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews.BMJ 202137271 n 7110.1136/bmj.n 7133782057 PMC 8005924 · doi ↗ · pubmed ↗
- 3Shea B.J. Grimshaw J.M. Wells G.A. Boers M. Andersson N. Hamel C. Porter A.C. Tugwell P. Moher D. Bouter L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews.BMC Med. Res. Methodol.2007711010.1186/1471-2288-7-1017302989 PMC 1810543 · doi ↗ · pubmed ↗
- 4Shea B.J. Hamel C. Wells G.A. Bouter L.M. Kristjansson E. Grimshaw J. Henry D.A. Boers M. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews.J. Clin. Epidemiol.200962101013102010.1016/j.jclinepi.2008.10.00919230606 · doi ↗ · pubmed ↗
- 5Salakari M.R.J. Surakka T. Nurminen R. Pylkkänen L. Effects of rehabilitation among patients with advances cancer: A systematic review.Acta Oncol.201554561862810.3109/0284186 X.2014.99666125752965 · doi ↗ · pubmed ↗
- 6Mc Caffrey N. Bradley S. Ratcliffe J. Currow D.C. What aspects of quality of life are important from palliative care patients’ perspectives? A systematic review of qualitative research.J. Pain Symptom Manage.2016522318328.e 510.1016/j.jpainsymman.2016.02.01227216362 · doi ↗ · pubmed ↗
- 7Maharaj S. Harding R. The needs, models of care, interventions and outcomes of palliative care in the Caribbean: A systematic review of the evidence.BMC Palliat. Care 2016151910.1186/s 12904-016-0079-626801078 PMC 4722788 · doi ↗ · pubmed ↗
- 8Health Quality Ontario Vertebral augmentation involving vertebroplasty or kyphoplasty for cancer-related vertebral compression fractures: A systematic review.Ont. Health Technol. Assess. Ser.20161611120227298655 PMC 4902848 · pubmed ↗