Disseminated Infection with Aspergillus fumigatus in a Scarlet Macaw Parrot (Ara macao)—A Case Report
Oana Irina Tanase, Geta Pavel, Ozana Maria Hritcu, Mihaela Anca Dascalu, Bianca Elena Bratuleanu, Cristina Mihaela Rimbu, Florentina Daraban Bocaneti

TL;DR
A scarlet macaw parrot died from a widespread fungal infection caused by Aspergillus fumigatus, diagnosed through postmortem examination and molecular testing.
Contribution
This is the first reported case of disseminated Aspergillus fumigatus infection in a scarlet macaw parrot.
Findings
Postmortem examination revealed granulomas and caseous plaques in multiple organs, including lungs, air sacs, and liver.
Fungal hyphae were confirmed via histopathology, culture, and molecular identification as Aspergillus fumigatus.
The case highlights the diagnostic challenges of aspergillosis in psittacine birds due to non-specific clinical signs.
Abstract
Aspergillosis is an important fungal disease occurring in avian fauna, especially in birds kept in captivity. In Psittaciformes, severe disease occurs in the lungs and air sacs, with the development of white-to-yellow caseous nodules and plaques in the organs, in addition to greenish-grey fungal growth in the air sacs. Herein, we report the presence of disseminated infection with Aspergillus fumigatus in a 3-year-old male scarlet macaw parrot (Ara macao) that was presented to the Exotic Animal Clinic at the Faculty of Veterinary Medicine, Iași University of Life Sciences (Iași, Romania) for its postmortem examination. The confirmation of the fungal infection was achieved using histopathological, microbiological, and molecular methods. Since birds suffering from Aspergillus spp. do not always show respiratory issues, or their clinical signs are non-specific, this may create diagnostic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1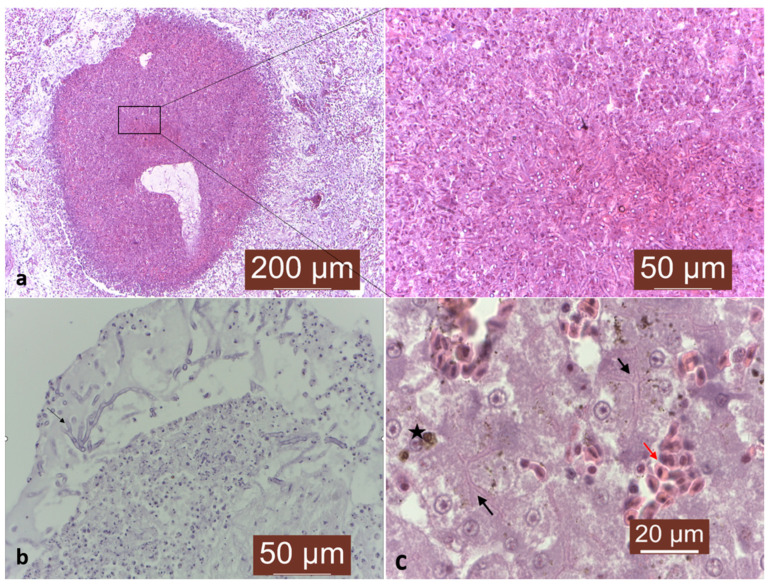 Figure 2
Figure 2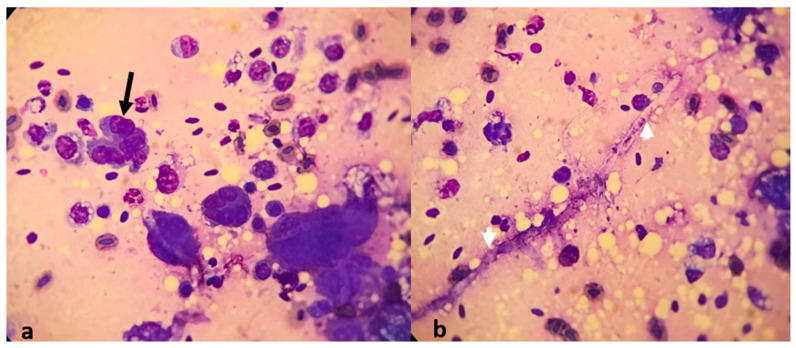 Figure 3
Figure 3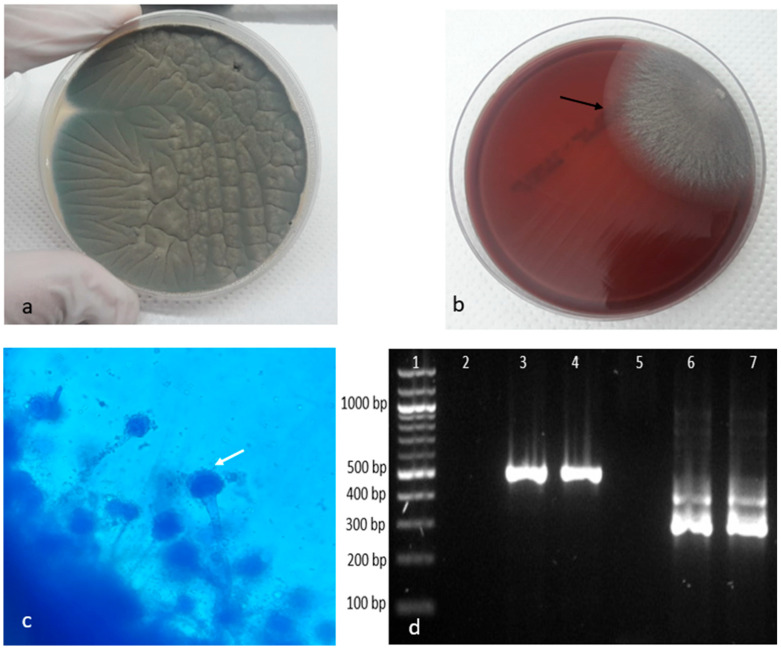 Figure 4
Figure 4- —Iasi University of Life Sciences Ion Ionescu de la Brad
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInsect and Pesticide Research · Bird parasitology and diseases · Vector-borne infectious diseases
1. Introduction
Aspergillosis is an important fungal disease in avian fauna. Out of the approximately 340 accepted Aspergillus species (Aspergillus spp.), only a small number are implicated in the development of avian aspergillosis [1]. According to recent studies, Aspergillus fumigatus is by far the most prevalent species, representing up to 95% of all occurrences in both wild and domestic avian species [1,2]. Birds kept in captivity are more susceptible to acquiring an infection with Aspergillus spp. due to several factors related to environmental conditions (increased concentration of fungal spores precipitated by humid, warm, dirty, poorly ventilated air) or to host immunity (concurrent infections, virulence of the isolate, therapies, stress) [3,4]. The anatomy and physiology of the avian respiratory system is substantially distinct from that of the bronchoalveolar lungs of mammals. Given the small size (2–3 µm), inhaled Aspergillus fumigatus conidia is able to overcome the first physical barriers and profoundly penetrate into the respiratory system and subsequently, into the air sacs, which are particularly predisposed to contamination, since they are subjected to an airflow that facilitates particle deposition. In addition, avian species have few resident macrophages to eliminate corpora aliena and have an epithelial surface nearly lacking in a mucociliary transport mechanism [5]. When the immune response is less effective, the fungus can spread from the respiratory system via the circulatory system or by simple extension from the air sac wall to contiguous organs or cavities. Moreover, hematogenous transmission is achieved by hyphal penetration of the lung blood vessels and by means of macrophages transporting viable spores. Under appropriate aerobic conditions, fungal asexual reproduction within the air sacs is a common result, associated with plaques becoming velvety and changing color, depending on the Aspergillus spp. involved [6]. Microscopically, lesions are characterized by granulomatous inflammation associated with the fungal hyphae.
Acute infection, usually seen in young poultry, is defined by high morbidity and mortality, by respiratory signs, or by systemic disease in the visceral organs and the brain, while chronic respiratory infection is mostly seen in adult or captive birds, such raptors or parrots [7]. Furthermore, aspergillosis has been confirmed in various species of captive parrots, such in African grey parrots (Psittacus erithacus), blue-fronted Amazon parrots (Amazona aestiva), or Eclectus parrots (Eclectus roratus) [8,9,10]. In Psittaciformes, severe disease occurs with infection of the lower respiratory system (lungs and air sacs), resulting in the development of white-to-yellow caseous nodules and plaques in the organs, in addition to greenish-grey fungal growth in the air sacs [11]. Herein, we report the presence of disseminated infection with Aspergillus fumigatus in a scarlet macaw confirmed by histopathological, microbiological, and molecular methods.
2. Materials and Methods
2.1. Case Description
A 3-year-old male scarlet macaw (Ara macao) was presented to the Exotic Animal Clinic at the Faculty of Veterinary Medicine, Iași University of Life Sciences (Iași, Romania) in June 2021 for its postmortem examination. According to the owner, the parrot had been raised only in captivity and after 5 days of inappetence, lethargy, and mild respiratory clinical signs, the parrot suddenly died. No antemortem assays had been performed. A post-mortem examination was performed, and various-sized granules were noted in the internal organs. For the histopathological evaluation, tissue samples were collected from the lungs and liver, fixed in 10% buffered formalin, embedded in paraffin, sectioned at 5 μm, and stained with Masson’s trichrome stain. Moreover, in order to visualize the suspected fungal hyphae, the sectioned samples were stained using periodic acid Schiff (PAS) staining. In parallel, for cytological examination, fresh smears from the lungs were prepared and routinely stained using the May–Grünwald–Giemsa method.
2.2. Isolation and Identification of Aspergillus spp.
Samples from the lungs and liver were cultured onto Sabouraud dextrose agar (Oxoid, Basingstoke, UK) and onto Mueller–Hinton agar with 5% sheep blood (Oxoid) and aerobically incubated at 37 °C for 7 days. Aspergillus fumigatus is a thermophilic species that can develop at temperatures of up to 55 °C, but can also survive up to 70 °C [12].
The suspected Aspergillus fumigatus isolate was obtained, and its macroscopic and microscopic morphologies, such as hyphae, conidial heads, and arrangements, were identified by lactophenol cotton blue staining, as previously described by Thom and Raper (1945) [13].
The conventional polymerase chain reaction (PCR) technique was performed on lungs and liver for the identification of Aspergillus fumigatus, following a protocol published by Sugita et al. (2004) [14]. Briefly, the DNA was extracted using the PureLink™ Genomic DNA Mini Kit, following the manufacture’s instruction. The genus specific amplification was performed using the PCR Master Mix Platinum II Hot-Start Green (Invitrogen, Vilnius, Lithuania), 5 µL of extracted DNA, and 20 µM of primers ASAP1 (5′-CAGCGAGTACATCACCTTGG-3′) and ASAP2 (5′-CCATTGTTGAAAGTTTTAACTGATT-3′). The cycling conditions consisted of: an initial denaturation step at 94 °C for 4 min, 30 cycles of denaturation at 94 °C for 1 min, annealing at 55 °C for 2 min, and extension at 72 °C for 90 s, followed by a final extension step at 72 °C for 10 min. By nested PCR, for the specific amplification of the A. fumigatus ITS1 region, the primers ASPU (5′-GCCCGCCGTTTCGAC-3′) and AFI3 (5′-CCGTTGTTGAAAGTTTTAACTGATTAC-3′) were used, with a 1 µL PCR product used as a template. The cycling conditions consisted of: an initial denaturation step at 94 °C for 4 min, 25 cycles of denaturation at 94 °C for 1 min, annealing at 60 °C for 15 s, and extension at 72 °C for 15 s, followed by a final extension step at 72 °C for 10 min. The amplification products were visualized using 2% agarose gel electrophoresis.
3. Results
During the post mortem examination, extreme emaciation, with loss of body weight, was revealed. Various-sized granulomas and caseous plaques were observed in the lungs, air sacs, kidneys, spleen, intestinal serosa, and liver (Figure 1a,b).
The histopathological evaluation of the collected samples revealed areas of necrosis in the pulmonary parenchyma, characterized by infiltration of numerous multinucleated giant cells, epithelioid-like cells, fibrin heterophilic deposits, and hemosiderin granules. The necrotic areas were delimited from the surrounding tissue, while the bronchi spaces were blocked by inflammatory infiltrate (Figure 2a). Additionally, using PAS staining, numerous fungal hyphae with a characteristic architecture consisting of 45° dichotomous branches were observed within the necrotic and inflammatory areas of the affected lung parenchyma (Figure 2b).
In liver tissue, a diffuse inflammation, characterized by a mild congestion with a significant hepatocyte necrosis, hemosiderin granules phagocytosis, and numerous fungal hyphae, were noted (Figure 2c).
Furthermore, the cytological examination of the lung smears revealed the presence of inflammatory cells consisting of numerous neutrophiles, macrophages, and lymphocytes. Moreover, atypical cells showing multinucleated giant cells (Figure 3a) with intensely vacuolated cytoplasm and undifferentiated walls, along with few fungal hyphae, have been identified (Figure 3b).
Following the cultivation on Sabouraud dextrose agar and Mueller–Hinton agar with 5% sheep blood media, the fungal presence in the lung and liver samples was confirmed, while according to the mycological descriptions, the causative Aspergillus spp. was identified as Aspergillus fumigatus on the basis of the following: (1) cultural characteristics—the presence of dense smoky colonies, gray-green in color with a slight creamy-white reverse (Figure 4a), and (2) microscopical morphology (revealed by lactophenol cotton blue staining)—septate hyphae and columnar conidia with a diameter from 2.5 to 3 µm, basipetally constructed in chains from a single palisade-like layer of phialides that were produced directly on broadly clavate vesicles in the absence of metulae (Figure 4c). These results were confirmed by PCR and nested PCR assays, in which an amplified product of 521 bp, corresponding to genus Aspergillus, and a product of 310 bp, corresponding to the Aspergillus fumigatus ITS1 region, respectively, were amplified in both the lung and liver samples and visualized by electrophoresis (Figure 4d).
4. Discussion
Avian aspergillosis is described as a disease of captivity, with Aspergillus fumigatus and Aspergillus flavus mainly implicated as etiological agents, while their transmission occurs mostly via the respiratory route [10]. In our case, the infiltrate and the chronic lung parenchyma inflammation led to a progressive impaired air circulation, which eventually proved fatal. Aspergillus spp. is able to induce both granulomatous and diffuse lesions, consisting of some characteristic changes. Moreover, there is a high probability of finding both lesion types in the same affected organ, which may indicate that the dissemination route is not exclusively respiratory. In our case, the fresh examination of the lung granulomas using May–Grünwald–Giemsa staining demonstrated the characteristic branching structures of the Aspergillus spp. hyphae. Furthermore, the main lesions were identified in the lungs, where areas of necrosis, characterized by infiltration of numerous multinucleated giant cells, epithelioid-like cells, fibrin heterophilic deposits, and hemosiderin granules were noted, which may suggest that the path of conidia infection was via the respiratory route, which is stated to be the main avian infection route [3]. Beside lung infection, other organs are also reported to be affected by Aspergillus spp. In this regard, Aspergillus spp. was isolated from rib osteomyelitis in farmed ostriches, from sternum osteomyelitis in chickens, from ribs bone marrow in the African grey parrot, from kidneys in a swift parrot, from ocular lesions in domestic turkeys and Rufous owls, or from gizzard and liver lesions in the Java Finch [15,16,17]. Interestingly, in Psittaciformes, liver damage has not been associated with Aspergillus spp. infection. Accordingly, in an African grey parrot (Psittacus erithacus) infected with Aspergillus fumigatus, significant damage was found in the lungs, while no lesions were reported in the liver [4]. Moreover, a similar pattern was reported in a captive Eclestus parrot (Eclestus roratus) infected with Aspergillus flavus [10]. In our case, Aspergillus spp. hyphae were noted in the liver, which were accompanied by a diffuse inflammation, characterized by a mild congestion, with a significant hepatocyte necrosis and phagocytosis of the hemosiderin granules. To the authors’ best knowledge, this is the first time that Aspergillus fumigatus has been associated with liver inflammation, suggesting a disseminated infection. The liver involvement demonstrated in this case may be explained by the small size of the conidia, enabling them to reach the lungs and its air sacs, and frequently, the caudal–thoracic and abdominal air sacs as well. When the immune system is not able to eliminate conidia, or when their accumulation is high, the infection progresses, with subsequent dissemination to the surrounding tissues, such those of the lungs, bronchi, liver, spleen, or intestinal serosa [3,4].
The identification of the Aspergillus spp. is of great importance in the confirmation of the avian aspergillosis diagnostic, since confusion may occur due to the lack of differences between the lesions induced by various species of Aspergillus such as Aspergillus fumigatus, Aspergillus flavus, Aspergillus niger, Aspergillus nidulans, or Aspergillus restrictus [10,17].
According to some authors, the simultaneous isolation of Aspergillus spp. with the demonstration of specific lesions plays a key role in the confirmation of the diagnostic [10,18,19]. As stated by Ref. [7], “due to the ubiquity of Aspergillus conidia, isolation of the fungi without the presence of lesions is not of diagnostic”. In this case, the microscopical findings were further confirmed by the successful isolation of Aspergillus fumigatus on Sabouraud dextrose agar and Mueller–Hinton agar media and by its microscopical mycological morphology revealed by lactophenol cotton blue staining. Furthermore, the aforementioned diagnostic methods were completed by PCR using genus-specific and species-specific primers. According to Ref. [20], this approach, based on PCR detection for Aspergillus spp., is highly recommended for a definitive diagnosis, since this technique allows for the active demonstration of sensitivity and specificity (PCR 25%, culture 19.5%, microscopy 10%).
The histopathological findings for the macroscopical lesions, along with the fungal isolation and molecular confirmation of Aspergillus fumigatus by nested PCR, allowed for the diagnostic of disseminated aspergillosis.
It is important to note that the treatment of avian aspergillosis, when possible, is not always successful, for various reasons, including the following: (1) the diagnosis is confirmed in the late stages of the disease; (2) a narrow spectrum of antifungal drugs are available for avian species; (3) the available drugs may fail to penetrate the target tissues; (4) concurrent diseases and/or immunosuppression may be present [1]. Since aspergillosis occurrence in captive birds is known to depend on several factors, such as improper environmental conditions or host immunity, preventative measures play a crucial role. In this context, controlling the level of exposure and minimizing stressors are necessary. Moreover, a regular cleaning and disinfection of the nest areas, opening the canopy to increase the amount of sunlight reaching the floor of the aviaries, and ensuring proper ventilation, together with improved animal husbandry practices, can minimize stress in the environment, which in turn decreases the risk of aspergillosis [1].
5. Conclusions
Since birds suffering from Aspergillus spp. do not always show respiratory issues and considering that the clinical signs are non-specific, together, these challenges may create diagnostic difficulty for clinicians unfamiliar with the parrots’ pathology. Therefore, for a definitive diagnosis, demonstration of fungal presence by cytology or histopathology, and its identification using culturing and molecular techniques, is required.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1ArnéP. Risco-Castillo V. Jouvion G. Barzic C.L. Guillot J. Aspergillosis in wild birds J. Fungi 2021724110.3390/jof 703024133807065 PMC 8004873 · doi ↗ · pubmed ↗
- 2Tell L.A. Aspergillosis in mammals and birds: Impact on veterinary medicine Med. Mycol.200543(Suppl. S 1)S 71S 7310.1080/1369378040002008916110795 · doi ↗ · pubmed ↗
- 3Oglesbee B.L. Mycotic diseases Avian Medicine and Surgery 1st ed. Altman R.B. Chubb S.L. Dorrestein G.M. Quesenberry K. Publisher Saunders Company Philadelphia, PA, USA 1997323361
- 4De Oca V.M. Martínez S.E.V. Salinas E.M. Roberto E.O. Sánchez-Godoy F. Pathological and mycological characterization of pulmonary Aspergillus fumigatus infection producing gliotoxin in a captive African grey parrot (Psittacus erithacus)Braz. J. Vet. Pathol.202215939810.24070/bjvp.1983-0246.v 15i 2p 93-98 · doi ↗
- 5Maina J.N. The Lung-Air Sac System of Birds: Development, Structure, and Function 1st ed.Springer Berlin/Heidelberg, Germany New York, NY, USA 200515917410.1007/3-540-29727-8 · doi ↗
- 6Hauck R. Cray C. França M. Spotlight on avian pathology: Aspergillosis Avian Pathol.20204911511810.1080/03079457.2019.169694631766868 · doi ↗ · pubmed ↗
- 7Kaplan W. Arnstein P. Ajello L. Chandler F. Watts J. Hicklin M. Fatal aspergillosis in imported parrots Mycopathologia 197556252910.1007/BF 004935791097931 · doi ↗ · pubmed ↗
- 8Burr E.W. Enzootic aspergillosis in wild red vented cockatoos in the Philippines Mycopathologia 198173212810.1007/BF 004430087012630 · doi ↗ · pubmed ↗