Valve-in-valve transcatheter aortic valve implantation (TAVI): a new valuable approach to bioprosthetic infective endocarditis?
Joelle Kefer, David Vancraeynest, Véronique Roelants, Leila Belkhir

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
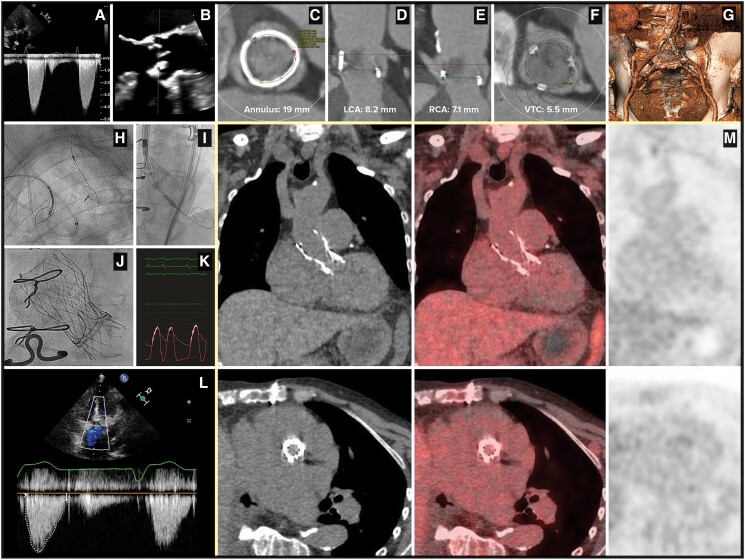 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSocial and Educational Sciences
A 77-year-old female patient was admitted for heart failure and severe aortic Magna Ease 21 mm bioprosthetic valve dysfunction (Figure 1A, Supplementary material online, Movie Image S1). Echocardiography revealed a vegetation on the right cusp of the bioprosthesis (Figure 1B, Supplementary material online, Movie Images S2 and S3), and blood cultures were positive for a Streptococcus sanguinis. Despite antibiotics (ceftriaxone followed by penicillin), stroke due to septic embolization occurred 3 days after the initial presentation.
The recommended treatment^1^ would have been surgical intervention, for a complete debridement of the infected material. Because of a prohibitive risk for surgery, the heart team considered a transcatheter aortic valve implantation (TAVI), which has not been empirically considered in this context until now, mainly due to the procedural risk and to the expected probability of infectious relapse during follow-up.
According to the pre-procedural computed tomography (CT) findings (Figure 1C–G), an Evolut-R 23 mm was successfully implanted (Figure 1H–J, and Supplementary material online, Movie Image S4). Thanks to the supra-annular design of the Evolut platform, the peak residual gradient was only 4 mmHg, with no leak (Figure 1K, Supplementary material online, Movie Image S5).
The periprocedural period was uneventful, antibiotics were stopped at Day 3, and patient was discharged at Day 8 under apixaban, with a good clinical outcome after 3 months, a well-functioning valve (peak gradient of 17 mmHg, trivial leak, no vegetation, no abscess—Figure 1L). There was no reinfection, as suggested by the low level of C-reactive protein (0.8 mg/dL—normal ranges: 0.6–1.3) and the absence of abnormal uptake during 18F-FDG PET-CT (Figure 1M).
To date, only six male patients underwent TAVI for active aortic valve infective endocarditis.^2^ To our knowledge, this is the first report of TAVI performed in a frail woman to treat a bioprosthetic infective endocarditis, with a PET-CT follow-up illustrating the absence of infectious relapse. Since surgical aortic valve replacement is not offered to a substantial number of patients with prohibitive surgical risk, TAVI would become a valuable approach to correct the residual valvular dysfunction despite antibiotics. The heart teams could include this strategy in the decisional tree of bioprosthetic infective endocarditis, integrating it in the lifetime management^3^ of each patient.
Supplementary Material
ytae384_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Delgado V , Ajmone Marsan N, de Waha S, Bonaros N, Brida M, Burri H, et al 2023 ESC guidelines for the management of endocarditis. Eur Heart J 2023;44:3948–4042.37622656 10.1093/eurheartj/ehad 193 · doi ↗ · pubmed ↗
- 2Brankovic M , Hashemi A, Ansari J, Sharma A. Transcatheter aortic valve replacement for aortic valve infective endocarditis: a systematic review and call for action. Cardiol Ther 2023;12:297–306.37079182 10.1007/s 40119-023-00314-9PMC 10209359 · doi ↗ · pubmed ↗
- 3Russo G , Tang G, Sangiorgi G, Pedicino D, Enriquez-Sarano M, Maisano F, et al Lifetime management of aortic stenosis: transcatheter versus surgical treatment for young and low-risk patients. Circ Cardiovasc Interv 2022;15:915–927.36378737 10.1161/CIRCINTERVENTIONS.122.012388 · doi ↗ · pubmed ↗