Huge, invasive, and destructive Abiotrophia defectiva endocarditis of the aortic valve and the aortic wall: a case report of an emergency but successful Ross–Konno operation in a child
Vera Cetera, Massimiliano Cantinotti, Elisa Barberi, Vitali Pak

TL;DR
A rare case of severe heart infection caused by Abiotrophia defectiva in a child was successfully treated with emergency surgery despite high risks.
Contribution
This paper presents a rare pediatric case of A. defectiva endocarditis requiring emergency Ross–Konno surgery and highlights the need for surgical intervention in such cases.
Findings
Abiotrophia defectiva infective endocarditis in children is rare and often leads to severe complications.
Conservative antibiotic treatment is usually insufficient, requiring urgent surgical intervention.
Only 16 pediatric cases of A. defectiva endocarditis have been reported since 1995.
Abstract
Abiotrophia defectiva forms Gram-positive cocci, is part of normal oropharyngeal and gastrointestinal flora, and is rarely involved in endocarditis in children population. Its special nutritional requirements and subacute clinical course may delay diagnosis and proper treatment, leading to life-threatening consequences. We report a rare case of huge and destructive A. defectiva infective endocarditis (IE) of the aortic valve and the aortic wall in a 3-year-old child, in follow-up after surgical valvuloplasty for congenital aortic stenosis. The child presented at our department with signs of left side hemiplegia. Transthoracic echocardiography showed severe aortic regurgitation due to large vegetation extending to the aortic wall up to the aortic arch. Blood cultures resulted positive for A. defectiva. He was initially treated conservatively with antibiotic therapy. Ten days after…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
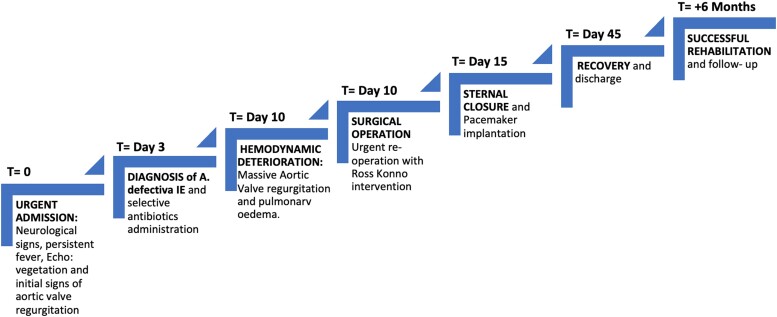 Figure 1
Figure 1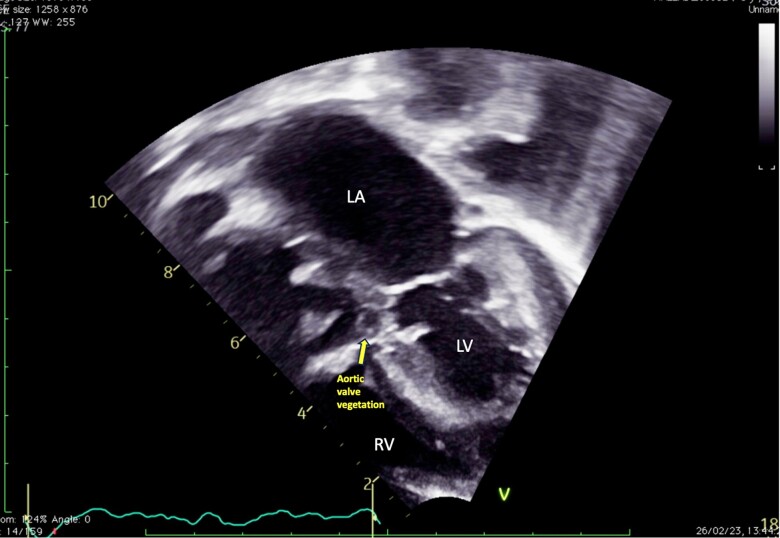 Figure 1
Figure 1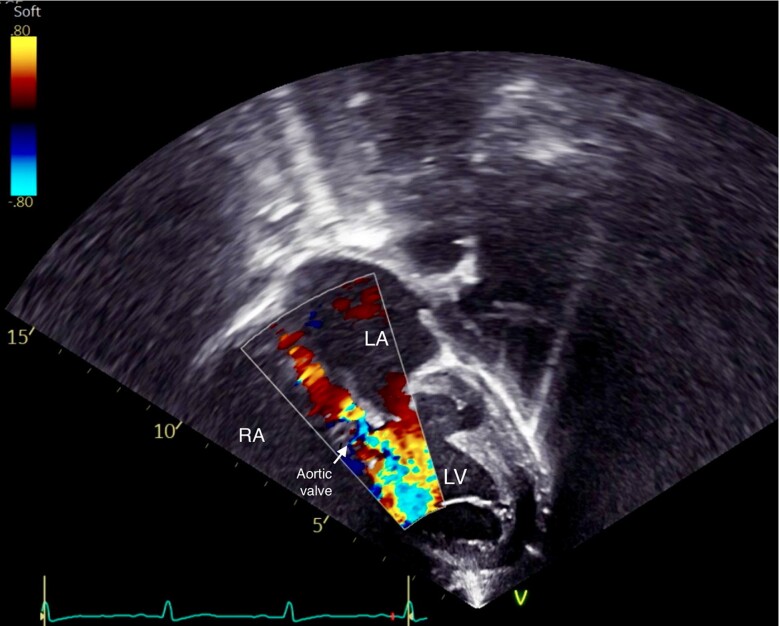 Figure 2
Figure 2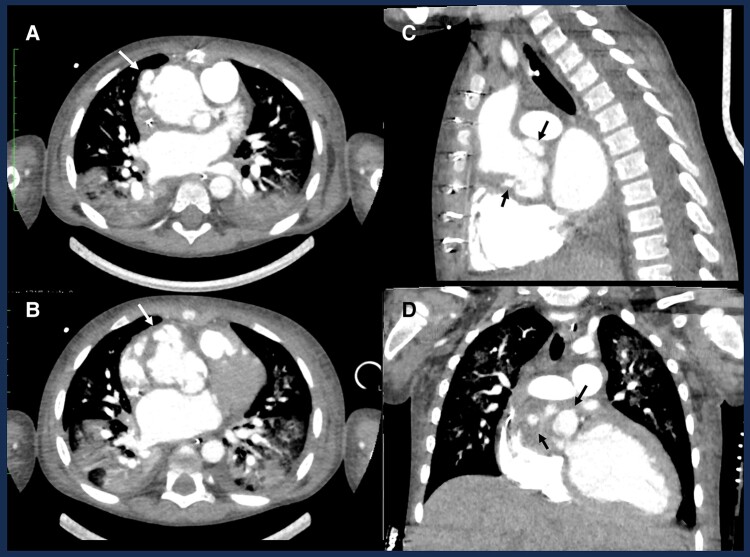 Figure 3
Figure 3| Study | Age | Sex | CHD | Predisposing factor | Embolization | Vegetation | Antibiotics | Surgery |
|---|---|---|---|---|---|---|---|---|
| Song | 15 | M | 0 | 0 | Cerebral/splenic | MV | AMP + CRO + GEN | No |
| Song | 6 | M | VSD | 0 | Septic pneumonia | TV | AMP + CRO + GEN | Yes |
| Song | 3.5 | F | PA | 0 | Septic pneumonia | PV | CTX + CRO | No |
| Song | 6 | F | VSD | 0 | Septic pneumonia | TV | CRO + GEN | Yes |
| Chang | 12 | F | 0 | Dental procedure | Thigh | MV | VAN + GEN → AMP + GEN → CTX + RIF | No |
| Raf | 5 | M | 0 | Dental procedure | Foot | MV + AV | VAN + GEN | Yes |
| Takayama | 17 | M | 0 | Dental procedure | Septic pneumonia | TV | PEN + GEN | Yes |
| Bhat | 11 | M | 0 | n.d. | Cerebral/splenic | MV | AMP/VAN + GEN | Yes |
| Bhat | 14 | F | 0 | Dental procedure | 0 | MV | AMP + GEN | Yes |
| Torres | 9 | M | VSD | Pharyngitis | 0 | RV + TV | AMP + GEN | No |
| Bonura | 9 | F | DX, VSD, AR, LV pseudoaneurysm | Face and oral trauma | Cerebral | Only LV pseudoaneurysm | CRO + GEN | Yes |
| Du | 8 | F | 0 | Suppurative tonsillitis | Cerebral | MV + left atrium | VAN + MRP | n.d. |
| Dong | 10 | F | VSD | Pharyngitis | 0 | RV + TV | VAN + MRP | Yes |
| Hayashi | 9 | M | VSD + BAV | Dental procedure | n.d. | n.d. | PEN | No |
| Krajcar | 5.5 | F | PDA | n.d. | 0 | 0 | CRO → cefpodoxime | Yes |
| Our case | 3 | M | AS s/p valvuloplasty | n.d. | Cerebral | AV + aortic root + ascending aorta | VAN + GEN + CRO | Yes |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Cardiac Valve Diseases and Treatments · Infectious Aortic and Vascular Conditions
Introduction
Abiotrophia defectiva is part of the normal flora of the gastrointestinal tract and is rarely involved in infective endocarditis (IE). Due to its atypical clinical presentation and the need for specialized culture media, diagnosis and treatment of IE by this pathogen may be delayed.^1,2^ Compared with other streptococci, IE by A. defectiva is known to be more aggressive and predisposed to valve destruction, heart failure, systemic embolization, and death.^2,3^ The majority of patients affected by A. defectiva IE require surgical intervention despite treatment with sensitive antibiotics.^2,4^ Our study reports one case of A. defectiva IE in a 3-year-old child with a history of aortic valve repair, who had severe neurological complications and successfully underwent Ross–Konno operation.
Summary figure
**
Case report
A 3-year-old male child, in follow-up for congenital aortic stenosis after neonatal surgical valvuloplasty, presented at our department with signs of left side hemiplegia. The parents reported only an isolated episode of toothache a few days prior to the onset of symptoms, which did not require any dental procedure. Upon admission, the child was irritable, his body temperature was 35.6°C, pulse rate of 130 b.p.m., blood pressure of 108/50 mmHg, and oxygen saturation of 98%. Electrocardiography showed moderate sinus tachycardia, normal PR interval and Qtc, left ventricular hypertrophy, and mild intraventricular delay. The transthoracic echocardiography (TTE) revealed moderate aortic regurgitation due to large vegetation on the aortic valve, extending to the aortic root and ascending aorta (see Figure 1). The ascending aorta was dilated (diameter: 39 × 38 mm) with multiple pseudoaneurysms on the right anterolateral wall (the largest: 12 × 9 mm of diameter). The size and systolic function of both ventricles were normal. Due to suspicion of cerebral embolization, computed tomography (CT) scan was urgently requested, which revealed a subtotal occlusion of the right median cerebral artery. Laboratory findings showed normal white blood cell count with high levels of C-reactive protein (10 mg/dL). Two separate sets of blood cultures, taken on admission, showed colonies of Gram-positive cocci growing on a blood agar plate. On the third day after admission, A. defectiva was identified by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry and the triple antibiotic treatment (vancomycin 100 mg/kg/day + ceftriaxone 80 mg/kg/day + gentamicin 35 mg/day) was started. Although his initial clinical stability led us to a conservative approach, 10 days after the admission, the child manifested a sudden deterioration of clinical conditions and developed signs of heart and lung failure, requiring urgent oral intubation. Transthoracic echocardiography demonstrated massive aortic regurgitation (Figure 2) and moderate tricuspid valve regurgitation (TVR) with signs of pulmonary hypertension and pulmonary oedema. Computed tomography chest scan was urgently performed, confirming the TTE findings (Figure 3). The heart team thereafter evaluated the critical conditions, young age, and surgical history of the patient and decided to proceed with an emergency Ross–Konno operation. Intraoperative findings confirmed the presence of active endocarditis, probably originating from the aortic annulus and then infiltrating the aortic root and the ascending aorta. Aortic wall appeared to be affected by several pseudoaneurysms bordered solely by adventitial tissue. The pulmonary valve and pulmonary truncus, on the other side, seemed to be free from vegetations or abscess. Several samples of tissue, collected and sent for microbiological analysis, resulted positive for A. defectiva. We harvested the pulmonary autograft and sutured it in aortic position and replaced the pulmonary trunk using Contegra® 20 mm conduit. Following the aortic clamp removal, temporary epicardial pacing leads were placed on the epicardium and immediately initiated for complete atrioventricular (AV) block. After a slow weaning and haemofiltration, we were able to close the sternum and move the patient to the post-operative care unit. Overnight, due to progressive signs of right ventricular failure, we reopened the sternum. On the fifth post-operative day, clinical improvements and haemodynamic stability allowed for successful sternal closure. At the same time, considering the persisting complete AV block, we decided to implant a permanent pacemaker. The following post-operative course was uncomplicated. The patient was extubated 2 days after the sternal closure. During his stay, he received 2 weeks of triple antibiotic therapy, then downgraded to vancomycin and ceftriaxone, to complete 5 weeks of intravenous treatment. He showed considerable neuro-motor improvements and was discharged home on 45th post-operative day, with one more month of oral antibiotic therapy (cefixime 100 mg/day). We performed several TTE during his stay, always confirming the good surgical results on the neo-aortic valve and good ventricular function. Residual moderate to severe TVR was also revealed, with no clinical consequences. This pathological finding is the result of TV annulus dilatation and consequent lack of coaptation. At the latest TTE assessment, 6 months after surgery, TVR remained stable, with an estimated systolic pulmonary pressure of 35 mmHg. The child was totally asymptomatic, on medical therapy (diuretic, beta-blocker, and aldosterone antagonist).
Transthoracic echocardiography performed at admission. Five-chamber view showing aortic valve vegetation.
Transthoracic echocardiography images showing massive aortic valve regurgitation on five-chamber views with colour Doppler.
Chest computed tomography scan showing several pseudoaneurysm and abscess (arrows) regarding the aortic root and ascending aorta on axial (A and B), sagittal (C), and coronal (D) views.
Discussion
Abiotrophia defectiva forms Gram-positive cocci, part of normal oropharyngeal flora, that is rarely involved in endocarditis, osteomyelitis, meningitis, brain abscess, and septic arthritis.^1^ According to the literature, Abiotrophia spp. are responsible for 4–6% of all cases of streptococcal endocarditis.^2,3^ To the best of our knowledge, 16 cases of A. defectiva IE have been reported in children population since 1995, including our case (Table 1).^4,5–10^ Among these 16 cases, 9 patients (56%) had a history of congenital heart disease (CHD). The patient we reported underwent surgery during the first year of life due to congenital aortic valve stenosis. This may suggest that children with CHD or previous cardiac surgery are more susceptible to contracting A. defectiva IE. Notably, in >60% of cases of A. defectiva IE, children had dental procedure or oral cavity infection (pharyngitis or suppurative tonsillitis) at the time of diagnosis. In our case, even though the primitive infectious source was not clearly identified, the toothache and the onset of the symptoms, within the following few days, remain extremely suspicious. Strong binding affinity for extracellular matrix proteins and high virulence can explain why A. defectiva causes severe complications, such as valve damage or emboli.^11^ Children seem to have a higher rate of complications (69% had embolic events) than adults, where the rate of systemic embolism is 11.8% and mycotic aneurysm is 8.8%.^2^ Our patient unfortunately presented both cerebral embolization and massive valve regurgitation. Considering this important rate of complications, prompt diagnosis and administration of appropriate antibiotics are crucial. Nowadays, the most common antibiotic strategy consists of β-lactam or vancomycin plus gentamicin.^2,12^ However, a recent study demonstrated that A. defectiva spp. 95–100% are responsive to third-generation cephalosporins.^13^ At admission, we started a broad-spectrum antibiotic therapy and then adjusted to vancomycin + ceftriaxone + gentamicin. Despite the specific antibiotic treatment, surgery was required in 10 out of the 16 cases reported in the literature. Recurrent embolic events, persistent large vegetation, or severe valvular dysfunction are the principal indications for surgery.^12^ In our experience, the decision to proceed with the surgery was particularly challenging, because of the complexity of the procedure (Ross–Konno operation) and the critical conditions of the child (haemodynamic instability, pulmonary oedema, and recent cerebral embolization). Nevertheless, a radical surgical intervention with delayed sternal closure, in addition to prolonged antibiotic therapy, revealed to be the correct strategy in such a difficult scenario.
Conclusion
Although A. defectiva remains a rare pathogen involved in IE, in the paediatric population, it causes a higher rate of complications. Prompt diagnosis and appropriate antibiotic administration are necessary to avoid life-threatening consequences. However, a conservative strategy is not always resolutive. Based on our experience and considering the good results reported in the literature, we suggest that surgery should not be delayed if one or more indications are present, even in highly risky conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bouvet A . Human endocarditis due to nutritionally variant streptococci: Streptococcus adjacens and Streptococcus defectivus. Eur Heart J 1995;16:24–27.10.1093/eurheartj/16.suppl_b.247671920 · doi ↗ · pubmed ↗
- 2Tellez A , Ambrosioni J, Llopis J, Pericàs JM, Falces C, Almela M, et al Epidemiology, clinical features, and outcome of infective endocarditis due to Abiotrophia species and Granulicatella species: report of 76 cases, 2000–2015. Clin Infect Dis 2018;66:104–111.29020360 10.1093/cid/cix 752 · doi ↗ · pubmed ↗
- 3Birlutiu V , Birlutiu RM. Endocarditis due to Abiotrophia defectiva, a biofilm-related infection associated with the presence of fixed braces: a case report. Medicine (Baltimore)2017;96:e 8756.29145328 10.1097/MD.0000000000008756 PMC 5704873 · doi ↗ · pubmed ↗
- 4Song SH , Ahn B, Choi EH, Lee SP, Cho EY, Bae EJ, et al Abiotrophia defectiva as a cause of infective endocarditis with embolic complications in children. Infection 2020;48:783–790.32474827 10.1007/s 15010-020-01454-z · doi ↗ · pubmed ↗
- 5Bonura ED , Sutherell JS, King W. Abiotrophia defectiva endocarditis with septic emboli and an enlarging subaortic pseudoaneurysm: a novel application for ferumoxytol cardiac magnetic resonance. Circ Cardiovasc Imaging 2022;15:e 014192.35862017 10.1161/CIRCIMAGING.122.014192 · doi ↗ · pubmed ↗
- 6Du Y , Zhang Z, Chen C, Xia H, Zhang H, Guo Z, et al Case report: report of infective endocarditis caused by Abiotrophia defectiva and literature review. Front Pediatr 2022;10:894049.35874573 10.3389/fped.2022.894049 PMC 9299070 · doi ↗ · pubmed ↗
- 7Dong W , Wu S, Zhou J. A rare association of invasive infective endocarditis due to Abiotrophia defectiva with ventricular septal defect and recurrent Henoch-Schonlein purpura in a child. J Cardiothorac Surg 2022;17:320.36528593 10.1186/s 13019-022-02092-2PMC 9758810 · doi ↗ · pubmed ↗
- 8Torres-Burgos I , Mendez-Castro L, Alkon J. A common defect with a not so common complication: Abiotrophia defectiva endocarditis in a child with unrepaired ventricular septal defect. CASE (Phila)2022;6:454–457.36589346 10.1016/j.case.2022.08.005PMC 9794499 · doi ↗ · pubmed ↗