A Cautionary Tale—Aortic Compression by Transesophageal Echocardiography Probe
Sarah Khan, Oliver Aregullin

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
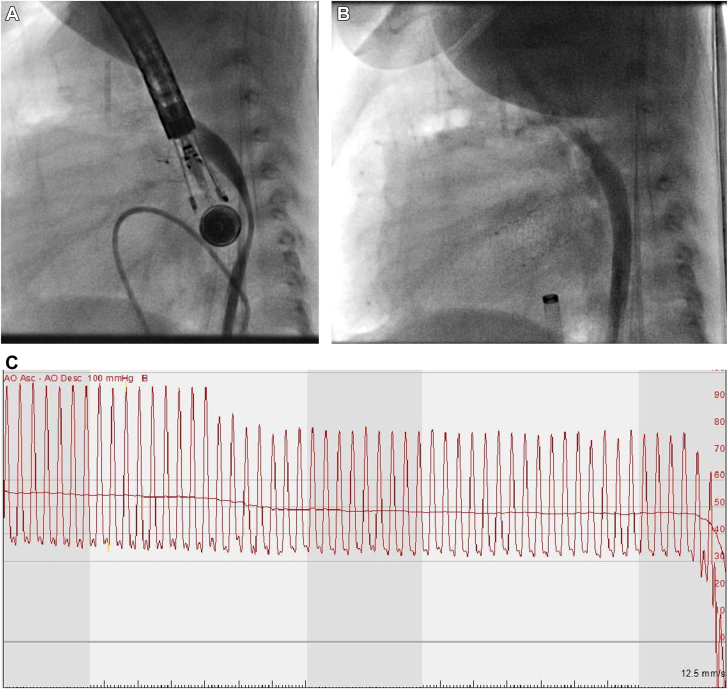 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Ultrasound in Clinical Applications · Cardiovascular and Diving-Related Complications
The use of transesophageal echocardiography (TEE) has become widespread in pediatric cardiac surgical operating rooms and cardiac catheterization labs. To limit fluoroscopy, TEE is frequently utilized for atrial septostomy and stent placement.1 Complications including esophageal injury, dental injury, and arrhythmia due to vasogenic response are well established in literature.2 A publication by Stevenson et al3 detailed a vascular compression incidence of 0.6% in pediatric patients, most commonly occurring intraoperatively in infants with congenital heart disease. Our report presents angiographic evidence of direct aortic compression by an appropriately sized TEE probe with resultant hemodynamic compromise.
Our patient was a 3-month-old, 4.2 kg, male baby with a postnatal diagnosis of critical aortic stenosis and severe mitral regurgitation, who initially underwent aortic valve balloon valvuloplasty followed by Damus-Kaye Stansel anastomosis, mitral valve repair, and Sano shunt placement as a neonate. This procedure is indicated in patients with single ventricle anatomy in which an anastomosis between the pulmonary artery and aorta provides relief of systemic outflow obstruction. The patient returned to the catheterization lab for atrial stent placement to decompress the hypertensive left atrium as well as repeat aortic balloon valvuloplasty and aortic arch angioplasty. Right heart catheterization was done through femoral venous access whereas left heart catheterization was accomplished through femoral arterial access in the usual fashion. Blood pressure was monitored through femoral arterial access. As appropriate for weight, a Philips S7-3t Pediatric TEE probe (Philips) was advanced to the mid-esophagus level. Immediately thereafter, femoral arterial tracing was lost, with ensuing profound hypotension 28/13 mm Hg. Immediate contrast injection in the descending aorta demonstrated near-complete compression of the aorta by the rotated TEE with near obliteration of the aortic lumen. With the removal of the TEE probe, repeat contrast injection demonstrated widely patent descending aorta and immediate normalization of blood pressure (Figure 1).Figure 1(A) Compression of the thoracic descending aorta by the TEE probe in anterior-posterior direction with near obliteration of aortic lumen. Probe dimensions: tip: 1.5 × 3.5 cm (0.6 × 1.4 in) W × L, shaft: 1.0 cm (0.4 in) diameter, 1 m (39.4 in). (B) Resolution of compression with removal of the TEE probe; contrast injection filling the widely patent thoracic descending aorta. (C) Femoral arterial waveform at the time of advancement of the TEE probe to mid-esophageal level with ensuing profound hypotension. TEE, transesophageal echocardiography.
It is important to consider vascular compression by TEE probes as a contributing factor for decreased central perfusion and hemodynamic instability in pediatric cardiac operating rooms and catheterization labs. A case series by Lunn et al4 proposed anteflexion and leftward rotation of the TEE probe as the culprit. The anatomical arrangement may explain this; the esophagus lies anterior and to the left of the aorta. It then passes further to the left as it passes through the esophageal hiatus to join the stomach. In small-sized patients, patients with dilated thoracic aorta, or dilated esophagus due to gastrointestinal reflux, this close interaction can be a factor in the protrusion of the TEE probe into the aortic lumen, especially with anteflexion and rotation to the left. Intraprocedurally, it is important to monitor the probe position and ensure a neutral position when not in active use. Upper extremity arterial catheter may miss vascular compression causing downstream vascular compression. We recommend monitoring lower extremity perfusion with a pulse oximeter, blood pressure cuff, or arterial catheter.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ayres N.A.Miller-Hance W.Fyfe D.A.Indications and guidelines for performance of transesophageal echocardiography in the patient with pediatric acquired or congenital heart disease: report from the task force of the Pediatric Council of the American Society of Echocardiography J Am Soc Echocardiogr 1812005919810.1016/j.echo.2004.11.00415637497 · doi ↗ · pubmed ↗
- 2Patel K.M.Desai R.G.Trivedi K.Neuburger P.J.Krishnan S.Potestio C.P.Complications of transesophageal echocardiography: a review of injuries, risk factors, and management J Cardiothorac Vasc Anesth 36820223292330210.1053/j.jvca.2022.02.015B 35317955 · doi ↗ · pubmed ↗
- 3Stevenson J.G.Incidence of complications in pediatric transesophageal echocardiography: experience in 1650 cases J Am Soc Echocardiogr 126199952753210.1016/s 0894-7317(99)70090-810359925 · doi ↗ · pubmed ↗
- 4Lunn R.J.Oliver W.C.Jr.Hagler D.J.Danielson G.K.Aortic compression by transesophageal echocardiographic probe in infants and children undergoing cardiac surgery Anesthesiology 773199258759010.1097/00000542-199209000-000271519796 · doi ↗ · pubmed ↗