ORTHOPEDIC INJURIES IN MEN’S PROFESSIONAL SOCCER DURING THE CORONAVIRUS DISEASE PANDEMIC
Gustavo Gonçalves Arliani, Eli Henrique Rodrigues da Silva, Hussein Fares, Paulo Henrique Schmidt Lara, Jorge Roberto Pagura, Moisés Cohen

TL;DR
This study examines soccer injuries during the pandemic in Brazil's Paulista Football Championship, finding no significant change compared to pre-pandemic times.
Contribution
The study provides insights into injury patterns during pandemic conditions in professional soccer.
Findings
Muscle injuries were most common, primarily affecting lower limbs.
Most injuries occurred between 31-45 minutes of play and were moderate in severity.
No significant difference in injury rates was found between pre- and post-pandemic periods.
Abstract
To assess the incidence and characteristics of injuries that occurred in the 2020 season of the Paulista Football Championship during the novel coronavirus disease pandemic. We conducted a prospective study using an electronic questionnaire developed by the Medical Committee of the Paulista Football Federation. Results were sent to the team doctors of series A1 and A2 after each round of the Paulista Football Championship. Series A1 and A2 presented 12.17 and 15.6 injuries, respectively, per 1000 gaming hours. The strikers were the most affected, with muscle injuries being the most frequent and the lower limbs being the most affected. Most injuries occurred within 31-45 minutes of playing; only 4.5% of injuries required surgery. There was no statistical difference in the comparison between pre- and post-pandemic conditions. In relation to the variables studied, the most injuries…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
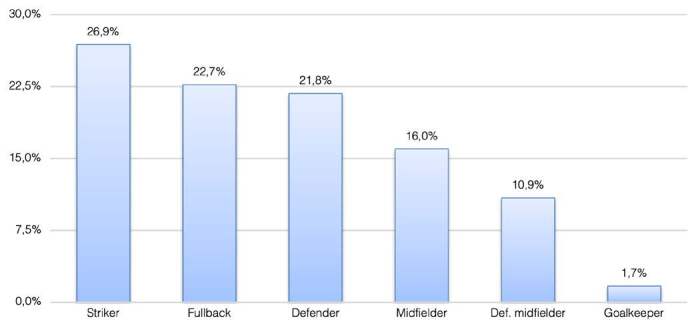 Figure 1
Figure 1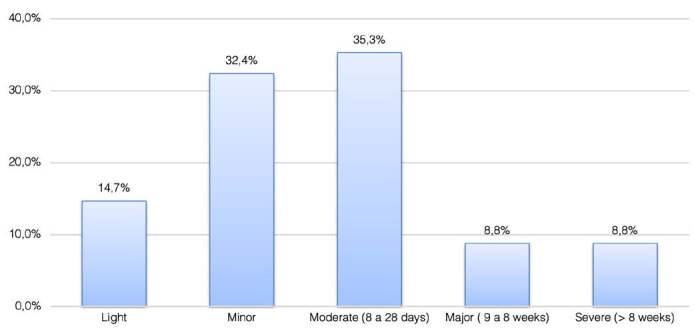 Figure 2
Figure 2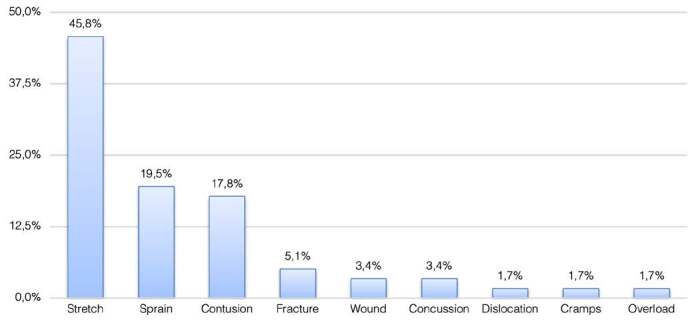 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSports injuries and prevention · Cardiovascular Effects of Exercise · Injury Epidemiology and Prevention
INTRODUCTION
Football is complex and involves considerable risk of injury with associated material, economic, and sports-related impact. In one month, placing a professional footballer on reserve due to injury translates to an average loss of € 500,000 and compromises the success of the team during football matches. 1 Therefore, because of physical and emotional stress, professional football is considered a sport with a high risk for injury. 2 Epidemiological studies revealed an incidence rate of 16-28 and 2-11 injuries during matches and practices, respectively, for every 1,000 hours of exposure at the professional level. 3 According to an epidemiological study on men’s professional football, the average injury rate is approximately 6-8 injuries per 1000 hours of exposure. 2
The majority of football injuries affect the lower limbs; more specifically, the ankles, knees, and thighs. 4 Susceptibility to specific types of injuries varies depending on the athlete’s position in the field. Significant differences found in the incidence rates possibly occur due to changes in game style and intensity. Moreover, the overall mood of the match also plays an important role in the specificities of each injury. 5 A study on elite athletes suggested that the different roles in each position require specific technical, physiological, and tactical demands from the players. For instance, central defense players are more likely to jump for the ball than external defenders, whereas external midfielders generally cover greater distances than those by central midfielders when running. 6
Injuries largely influence the final team results in both national and European tournaments. Such findings have revealed the importance of preventing injuries to increase the chances of awards and success. 7 Implementing prevention strategies for a given population requires obtaining and understanding evidence of a specific pattern. As such, several epidemiological investigations have been conducted worldwide. These patterns have been found to be common practices in main leagues, world tournaments, 2 ^,^ 8 and world cups. 9 ^,^ 10 Although football is the most popular sport in Brazil, there are only a few epidemiological studies and datas pertaining to the regional and national leagues. The purpose of this investigation was to compare the incidence and specificities of injuries to establish preventive measures and policies.
At the beginning of March 2020, the World Health Organization announced the coronavirus disease (COVID-19), an infection caused by the SARS-CoV-2 virus. Subsequently, it was declared a pandemic. As a result, most players had to train from home while following the routines provided by the teams’ strength and conditioning staff. 11 Despite these efforts, many players have shown signs of detraining, 12 thereby resulting in an increased risk of injury upon their return to playing. 13 The objectives of this study were to assess the incidence and characteristics of injuries that occurred in the 2020 season of the Paulista Football Championship before and after the pandemic.
METHODOLOGY
This study was approved by the Ethics Committee of the (number 1.660.701). This was a prospective study conducted via an electronic form developed by the Medical Committee of the São Paulo Football Federation (Federação Paulista de Futebol). Results were sent to the team physicians of series A1 and A2 after each round of the 2020 São Paulo State Football Championship.
The above-mentioned form was developed to analyze the incidence of injuries and their characteristics. The form comprised 15 questions on the specificities of the match, athlete, and injury (Appendix 1). The definition used to determine a football injury was the statement set out by Fuller et al. 14 for the 2005 FIFA consensus, and was as follows: “Any physical complaint sustained by a player that results from a football match or football training, irrespective of the need for medical attention or time loss from football activities”. A form was filled out by the athlete after returning from the field and used to analyze the outcome of each reported injury. There were eight questions structured in the form of complementary tests, exams, and final diagnoses (Appendix 2). The Football Federation was asked to record the events to obtain the time of each match; classifications are as follows: morning (matches beginning before 12 p.m.), afternoon (matches before 6 p.m.), and night (matches after 6 p.m.). The first 10 and 12 matches in the A1 and A2 series were played prior to the COVID-19 lockdown, respectively. Moreover, the remaining six and nine matches in the A1 and A2 series, respectively, were played after the break.
The incidence of injuries was calculated to assess the risk, expressed as the number of injuries per 1000 hours of exposure (14, 15). The following formula was used to calculate the exposure: Exposure = number of matches x number of players starting the match (22) × duration of the match in minutes (90) / 60. The following formula was used to calculate incidence at matches: Incidence = number of injuries at matches x 1000 hours/time of Exposure
Statistical analysis
Parametric statistics were used for data that were both quantitative and uninterrupted. The two-portion test was used to characterize the relative frequency distribution of the qualitative variables. Differences were considered statistically significant at p < 0.05. SPSS V17 software was used to perform the analyses.
RESULTS
Mapping of the injuries
The average age of the injured players was 26.6 years, whereas the average time loss caused by injuries was 20.6 days. Most matches occurred at night (47%). Furthermore, 9.5% were held in the morning and 43.6% in the afternoon. A total of 118 injuries were described during all 256 matches, with an average of 0.46 injuries per match. In terms of the playing position, 26.9% of the injuries were sustained by forwards, 22.7% by external defenders, 21.8% by central defenders, 16% by external midfielders, 10.9% by central midfielders, and 1.7% by goalkeepers ( Figure 1 ).
Figure 1.Position distribution
Most injuries occurred during the first half of the match, and within 31-45 minutes (23.5%), followed by 61-75 minutes (21%), 16-30 minutes, and 76-90 minutes (16%). Most injuries were deemed moderate based on the severity scale, with time loss ranging from 8 to 28 days (35.3%). The results are shown in Figure 2 .
In terms of site of injury, the most common injuries were on the following sites: thigh (42.9%), ankle (13.4%), knee (12,6%), and head (11,8%). Injuries occurred most often on the right side (49.6%); the side did not apply in 12.6% of the cases. The most common injury type was muscle strain (45.8%), followed by sprains (19.5%), and contusions (17.8%) ( Figure 3 ). With respect to the final diagnosis, the most frequent injuries were as follows: hamstring strain (22.4%), adductor muscle strain (10.4%), lateral ankle sprain (10.4%), quadriceps muscle strain (9%), and foot contusion (6%). There were 12.17 injuries per 1000 hours of matches in the A1 Series, and 15.6 injuries per 1000 hours of matches in the A2 Series. When summed, 13.96 injuries occurred in 1000 hours of matches in both series.
Figure 2.Severity distribution
Figure 3.Type of injury distribution
Treatment of the injuries
When requested, the most common complementary tests and exams were magnetic resonance imaging (MRI) (42.6%) and ultrasonography (22.1%), followed by radiography (13.2%) and computed tomography (CT) (4.4%). No tests were necessary for 13.2% of the injuries. Surgery was required in 4.5% of all recorded injuries. Most injuries were deemed moderate according to the severity scale, with a time loss ranging from 8 to 28 days (35.3%). ( Figure 3 )
Before and during the pandemic
The main results are presented in Table 1. There were no statistical differences between the two periods for the variables studied.
Table 1.General results before and after pandemyBeforeDuringTotalP-valueN%N%N%InjuriesWith injury9426,3%2521,7%11925,2%0,324Without injury26373,7%9078,3%35374,8%Tipe injuryStretch4346,2%1144,0%5445,8%0,556Sprain1920,4%416,0%2319,5%Contusion1415,1%728,0%2117,8%Fracture44,3%28,0%65,1%Dislocation11,1%14,0%21,7%Wound44,3%00,0%43,4%Concussion44,3%00,0%43,4%Cramps22,2%00,0%21,7%Overload22,2%00,0%21,7%Injury moment0-15min1313,8%28,0%1512,6%0,12316-30min1010,6%936,0%1916,0%31-45min2425,5%416,0%2823,5%46-60min1010,6%28,0%1210,1%61-75min2122,3%416,0%2521,0%76-90min1516,0%416,0%1916,0%Stoppage time 2 t11,1%00,0%10,8%
DISCUSSION
In this study, the incidence and characteristics of the injuries were similar to the data in the literature. 3 ^,^ 15 ^,^ 16 ^-^ 19 Muscle strains, sprains, and contusions were the most prevalent types of injuries, as was the case in several other investigations in the literature. 2 ^,^ 20 ^-^ 22 Only 4.5% of the injuries required surgery; most diagnoses required non-surgical treatment. In addition, fractures and severe ligament injuries were conservatively managed.
Similar to other studies developed by our group, MRIs were the most commonly requested exams. 21 ^-^ 23 As most cases were muscular injuries, MRI was deemed the most useful. Most injuries occurred within the first 31-45 minutes of the first half of the matches. 21 ^-^ 23 In other studies, the incidence was higher during the last 30 minutes of the match. 16 ^,^ 23 ^,^ 24 However, in some of these studies, the tournament was organized as a single-elimination system, which may have subsequently enhanced the motivation of the athletes.
Recent studies have shown the impact of the lockdown on the physical qualities of athletes. Rampini et al. 25 showed that home-based training during lockdown was effective in improving aerobic fitness, although it did not allow players to maintain their usual strength levels. Grazioli et al. 26 showed that 63 days of quarantine impaired several physical performance capabilities as compared with during regular off-season. Special attention should be given to body composition-, speed-, and power-related capabilities after long-term detraining. Moreno-Perez et al. 11 showed that during isolation at home, eccentric hamstring strength decreased; this magnitude of muscle weakness might indicate a higher risk of injury according to a previous study. 27 Despite showing increased risk for injuries, we found no statistical difference between the incidence and type of injuries and the moment at which these injuries occurred.
Regarding the incidence of injuries, the percentage of injuries before and after the lockdown was at 26.3% and 21.7%, respectively. In both periods, muscle strain was the most common injury, accounting for almost half of the cases; this condition showed that the lockdown did not alter the characteristics of the injuries. Moreover, differences in the occurrence of the injuries were observed. Before the lockdown, injuries were most common between 31-45 min of the match. After the return from the lockdown, they were most common at 16-30 min. This condition might be attributable to a decrease in muscle strength, thereby increasing the risk of injury and decreasing player endurance.
The greatest limitation of this study was the reliability of the information provided by the clubs’ medical personnel, as well as the lack of official records on injuries sustained during the matches. Moreover, it was not possible to accurately measure each athlete’s exposure.
CONCLUSION
Most injuries occurred in the lower limbs; muscle strains were the most common type of injury, followed by sprains and contusions. MRIs were the most commonly requested test; most injuries were classified as moderate. Approximately 4.5% of injuries evolved to require surgery. The results were similar before and after the lockdown due to the COVID-19 pandemic.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ekstrand J. Keeping your top players on the pitch: the key to football medicine at a professional level Br J Sports Med 2013477234
- 2Ekstrand J. Hägglund M. Waldén M. Injury incidence and injury patterns in professional football: the UEFA injury study Br J Sports Med 201145755381955322510.1136/bjsm.2009.060582 · doi ↗ · pubmed ↗
- 3Bjørneboe J. Bahr R. Andersen T. E. Gradual increase in the risk of match injury in Norwegian male professional football: A 6-year prospective study Scand J Med Sci Sports 201424189962258298110.1111/j.1600-0838.2012.01476.x · doi ↗ · pubmed ↗
- 4Ekstrand J. Hägglund M. Waldén M. Epidemiology of muscle injuries in professional football (soccer)Am J Sports Med 20113961226322133535310.1177/0363546510395879 · doi ↗ · pubmed ↗
- 5Waldén M. Hägglund M. Orchard J. Kristenson K. Ekstrand J. Regional differences in injury incidence in European professional football Scand J Med Sci Sports 201323424302209241610.1111/j.1600-0838.2011.01409.x · doi ↗ · pubmed ↗
- 6Di Salvo V. Baron R. Tschan H. Montero F. J. C. Bachl N. Pigozzi F. Performance characteristics according to playing position in elite soccer Int J Sports Med 20072822271702462610.1055/s-2006-924294 · doi ↗ · pubmed ↗
- 7Hägglund M. Waldén M. Magnusson H. Kristenson K. Bengtsson H. Ekstrand J. Injuries affect team performance negatively in professional football: an 11-year follow-up of the UEFA Champions League injury study Br J Sports Med 20134780782364583210.1136/bjsports-2013-092215 · doi ↗ · pubmed ↗
- 8K.Aus Der Fünten Faude O. Lensch J. Meyer T. Injury characteristics in the German professional male soccer leagues after a shortened winter break J Athl Train 2014496786932536513210.4085/1062-6050-49.3.51PMC 4264651 · doi ↗ · pubmed ↗