Ileal Lipohyperplasia Masquerading as Stricturing Crohn’s Disease
Muhammad B. Hammami, Nathalie H. Urrunaga

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
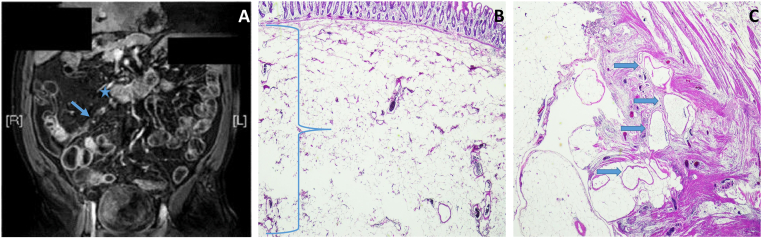 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Intraperitoneal and Appendiceal Malignancies · Pancreatitis Pathology and Treatment
A 47-year-old male with stricturing Crohn’s disease (CD) presented with intermittent right-lower-quadrant abdominal pain (RLQAP), nausea/vomiting, and constipation.
His history revealed small bowel resections (age 20/32 years) followed by 9 years of symptomatic remission with sulfasalazine, which was discontinued 7 years ago (medical insurance lapse). For 6 years, he had mild, intermittent, self-resolving RLQAP with nausea/vomiting that became more frequent two months ago, necessitating two hospitalizations (unremarkable esophagogastroduodenoscopy, colonoscopy, barium enema).
On presentation, he had mild RLQAP and tenderness without rebound/distention. Magnetic resonance enterography showed a 4-cm-dilated distal ileum (Figure A, asterisk), with 3 × 0.6-cm stricture proximal to the ileocecal valve (Figure A, arrow). Ileocecectomy revealed prominent adipose tissue in the submucosa between the mucosa and muscularis propria (Figure B, right brace) and dilated lymphatic vessels in the terminal ileum (Figure C, arrows) without evidence of CD.
This is the first case of lipohyperplasia causing small bowel stricture/obstruction in CD. Although management is still resection, lipohyperplasia should be considered in the differential diagnosis of small bowel stricture even in patients with known stricturing CD.