A Rare Finding of Gastric Metastasis From Tonsillar Squamous Cell Carcinoma
Anish Vinit Patel, Mahmoud A. Ali

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
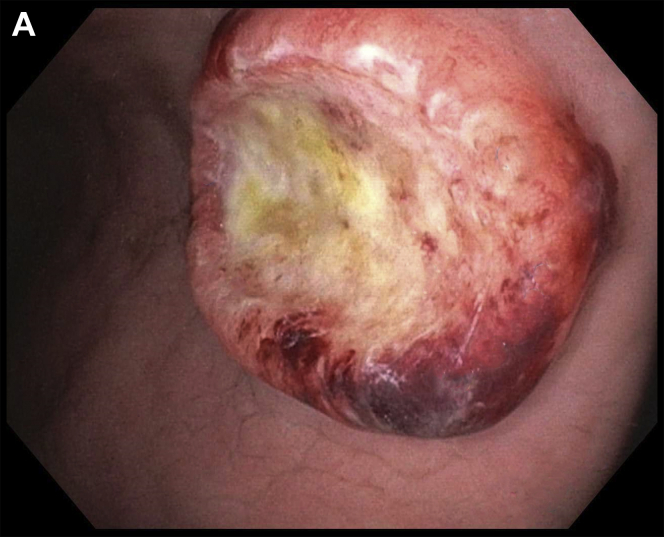 Figure 1
Figure 1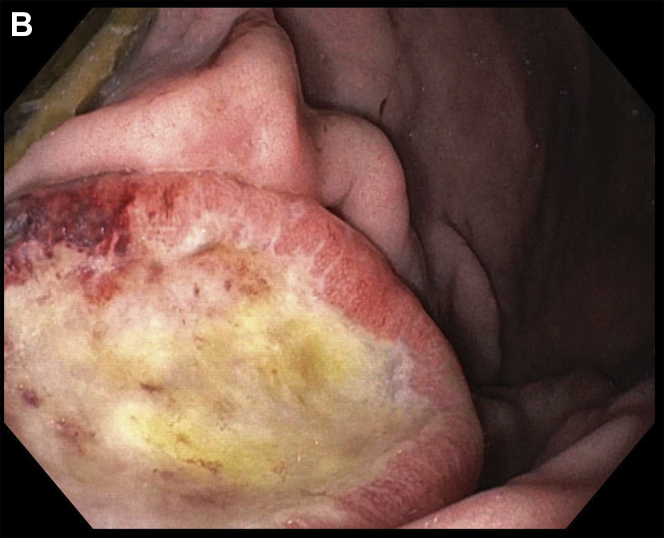 Figure 2
Figure 2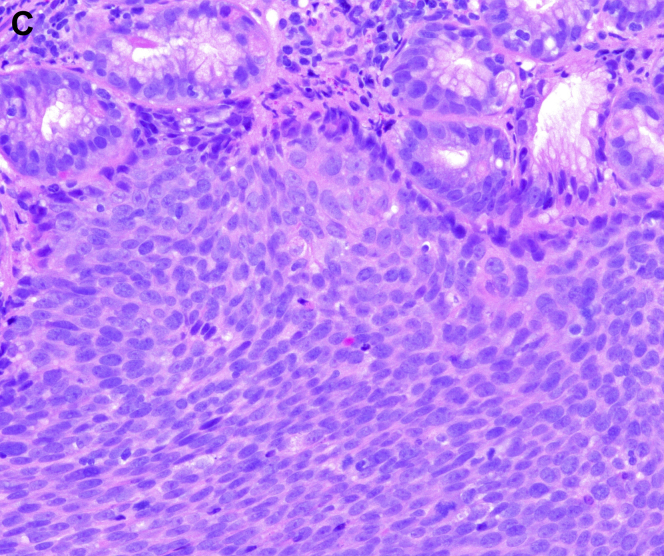 Figure 3
Figure 3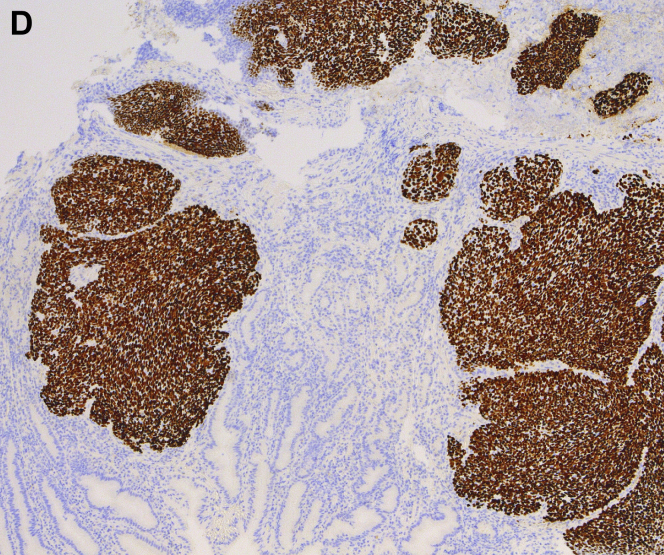 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Diagnosis and Treatment · Metastasis and carcinoma case studies · Tracheal and airway disorders
A 61-year-old Caucasian man with tonsillar squamous cell carcinoma (SCC, stage T2N1, diagnosed 1 year ago) underwent an endoscopic percutaneous gastrostomy tube (PEG) placement for oropharyngeal dysphagia at the time of diagnosis. Given pulmonary metastases, he was begun on immunotherapy. Upper endoscopy was scheduled for PEG tube replacement. He denied abdominal pain, melena, and hematochezia. Hemoglobin was 11.6 g/dL. The upper endoscopy found a 3-cm ulcerated mass along the greater curvature of the gastric body (Figure A and Figure B). This was located 2 cm away from the internal PEG bumper. He underwent an uneventful PEG replacement. Biopsies demonstrated SCC (Figure C), with staining positive for p40 (Figure D). This established the diagnosis of gastric metastasis of tonsillar SCC. He was continued on immunotherapy.
Head and neck SCC metastasize to the lung, bone, and liver. We demonstrate here one of the few reported cases of tonsillar metastases to the stomach, which is one of the least common primary malignancies that result in gastric metastases. Although our patient did not have metastases at the gastric stoma, PEG tubes have been suggested as a risk factor for distal seeding of metastases. Gastroenterologists should consider direct PEG placement instead of pull-through placement in such patients.