The Supreme Biodegradable Polymer DES in Acute and Chronic Coronary Syndromes: A PIONEER III Substudy
Yasin Hussain, Shigeru Saito, Michael Curtis, Dean J. Kereiakes, Andreas Baumbach, James P. Zidar, Brent McLaurin, Nabil Dib, Pieter C. Smits, Victor Alfonso Jiménez Díaz, Ángel Cequier, Sjoerd H. Hofma, Cody Pietras, Ovidiu Dressler, M. Ozgu Issever, Stephan Windecker

TL;DR
This study found that a new biodegradable stent (Supreme DES) is as safe and effective as a traditional stent for treating both acute and chronic coronary artery disease.
Contribution
The study provides evidence that the Supreme DES is noninferior to durable polymer stents in both acute and chronic coronary syndromes.
Findings
Supreme DES showed similar 12-month target lesion failure rates compared to durable polymer stents in patients with acute coronary syndromes.
There was no significant difference in safety outcomes like stent thrombosis between Supreme DES and durable polymer stents in either patient group.
Supreme DES achieved similar clinical outcomes in both acute and chronic coronary syndrome patients.
Abstract
The PIONEER III trial demonstrated noninferiority of 12-month target lesion failure (TLF) with the Supreme DES (Sinomed), a thin-strut cobalt-chromium, biodegradable polymer, sirolimus-eluting stent, compared with a durable polymer, everolimus-eluting (XIENCE/PROMUS) stent (DP-EES). The relative safety and effectiveness of the Supreme DES in patients with acute coronary syndromes (ACS) and those with chronic coronary syndromes (CCS) is not known. PIONEER III was a prospective, multicenter, international, 2:1 randomized trial stratified by clinical presentation. The primary end point was TLF at 12 months (a composite of cardiac death, target vessel myocardial infarction, or ischemia-driven target lesion revascularization). A total of 1628 patients were enrolled, including 41% of patients with ACS (unstable angina and non–ST-elevation myocardial infarction) randomized to Supreme DES (n…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
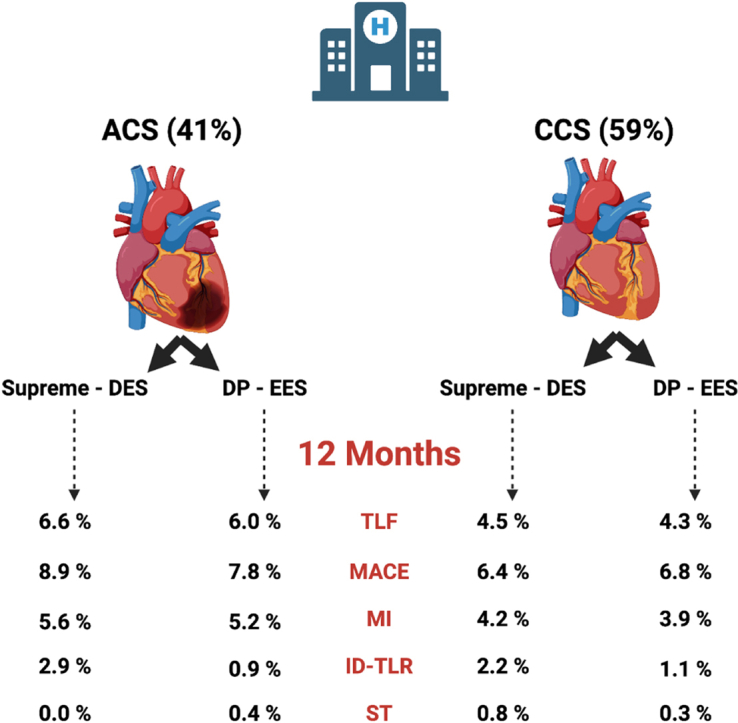 Figure 1
Figure 1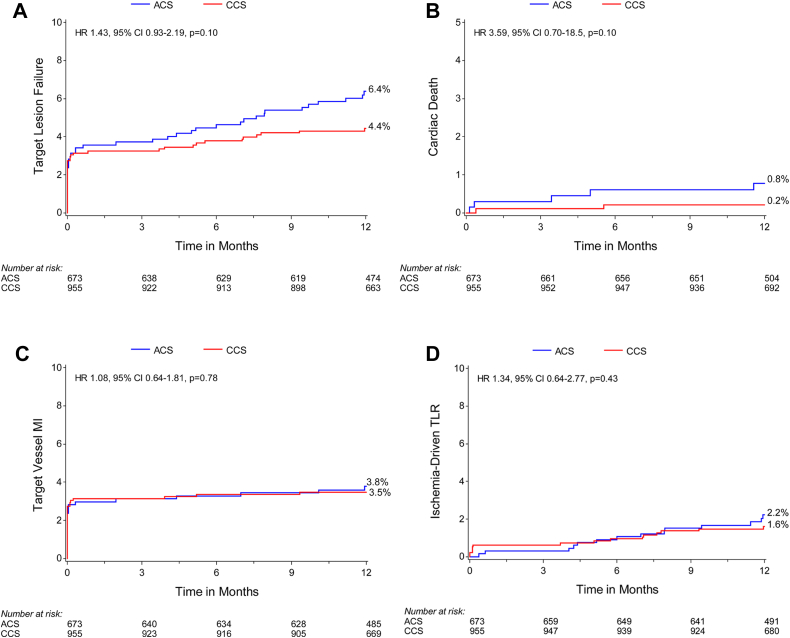 Figure 2
Figure 2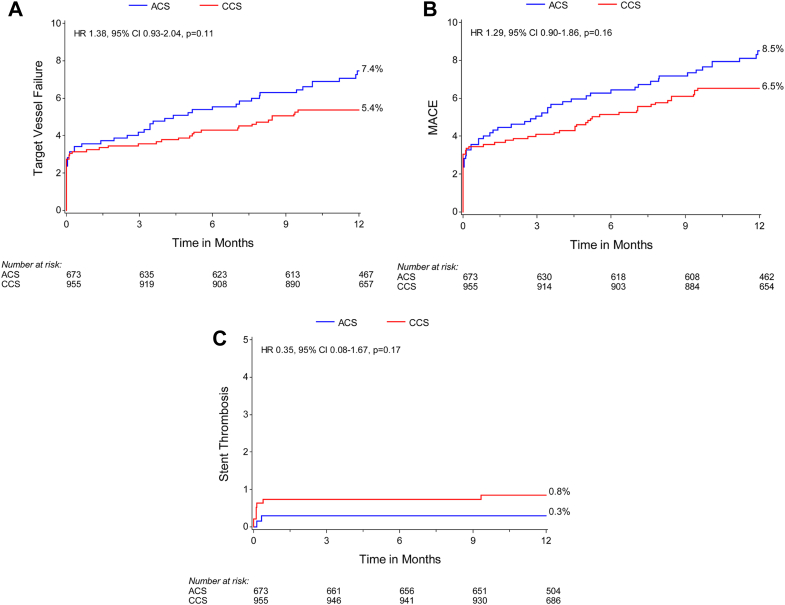 Figure 3
Figure 3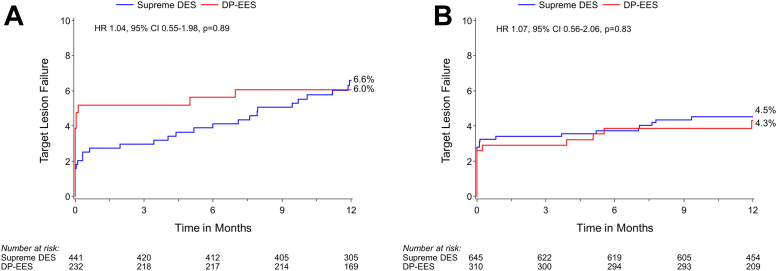 Figure 4
Figure 4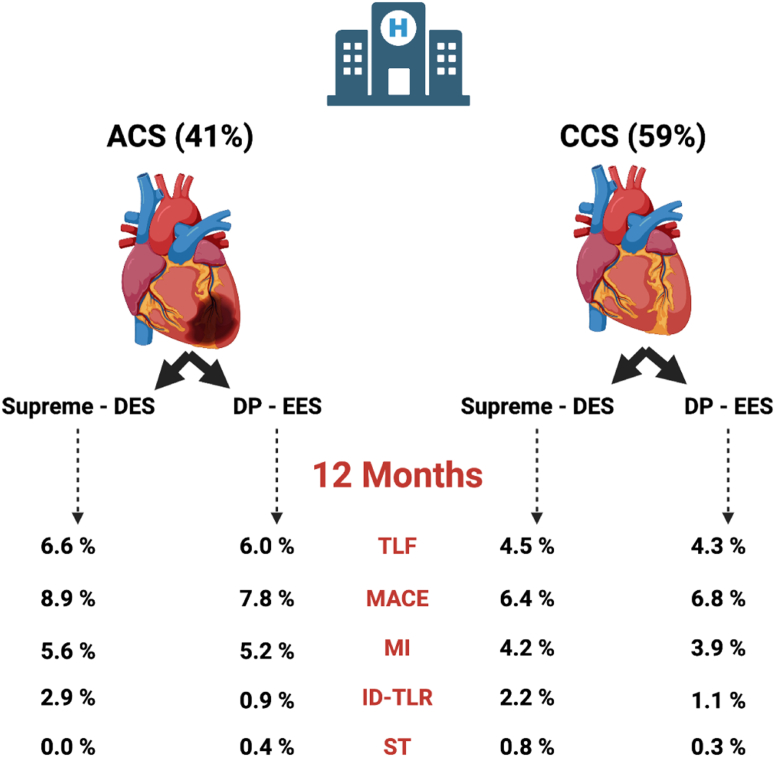 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Antiplatelet Therapy and Cardiovascular Diseases · Cardiac Imaging and Diagnostics
Introduction
Second-generation drug-eluting stents (DES) are the current standard of care for patients undergoing percutaneous coronary intervention (PCI).1, 2, 3 Patients presenting with acute coronary syndromes (ACS) tend to have worse outcomes than patients with chronic coronary syndromes (CCS).4 Evidence from autopsy series of patients treated with DES have demonstrated delayed culprit vessel healing in patients with ACS compared with that in patients with CCS, with less neointimal thickness, greater fibrin deposition, more inflammation, and greater areas of uncovered struts in patients with ACS.5 Furthermore, optical coherence tomography (OCT) studies have shown higher rates of incomplete stent apposition and uncovered stent struts in patients with ACS than those in patients with CCS in the short-term and longer term,6^,^7 and delayed vascular healing has been shown to be an important determinant of stent thrombosis and restenosis.8^,^9
The Supreme DES (Sinomed) is designed to accelerate early re-endothelialization and vascular healing by delivering the antiproliferative drug sirolimus with simultaneous polymer degradation within an early 4-week to 6-week therapeutic window, leaving behind a stent surface with a biostable ultrathin coating.10 Preclinical studies suggest that the Supreme DES achieves early endothelial restoration with improved vascular function and regulation of vascular smooth muscle cell proliferation, which may be of a particular benefit in patients with ACS.11, 12, 13 The PIONEER III trial demonstrated that the Supreme DES was noninferior to durable polymer everolimus-eluting stents (DP-EES) at 12 months.14 Whether the safety and effectiveness of the Supreme DES is consistent in patients with ACS compared with those in patients with CCS is not known.
Methods
Study design and population
PIONEER III (NCT03168776) is a prospective, 2:1 randomized, single-blind, multicenter trial conducted at 74 investigational sites in North America, Europe, and Japan. Randomization was stratified by ACS presentation. Patients were enrolled from October 2017 to August 2019. We report a prespecified analysis of PIONEER III based on ACS or CCS presentation at the baseline. The rationale, design, inclusion and exclusion criteria, methods, and data management have been reported previously.14 In summary, the study included adults with symptomatic CCS with an evidence of ischemia or ACS (unstable angina or non–ST-elevation myocardial infarction [MI]) requiring urgent or elective PCI. The trial was conducted in accordance with the tenets of the Declaration of Helsinki, and all patients provided signed informed consent.
Study procedures
The Supreme DES is a balloon-expandable, biodegradable polymer (BP), sirolimus-eluting coronary stent system. The stent platform is a laser cut L605 cobalt-chromium alloy tube that is electropolished to a strut thickness of 80.0 μm. Stent struts are covered by a nanometric (∼200.0 nm), nonerodible brush of poly(n-butyl methacrylate) that is covalently bonded to the metal surface through a proprietary electrografting (eG coating) process.15 The topcoat (3.0-μm to 10.0-μm thick) consists of a poly(lactic-co-glycolic acid) BP with sirolimus embedded at a drug density of 1.2 μg/mm^2^; both drug and topcoat are completely resorbed within 4-6 weeks.16^,^17 The design, safety, and efficacy of the Supreme DES has been extensively characterized.18 The control DP-EES (Xience, Abbott Vascular; Promus, Boston Scientific Corporation) is a laser cut cobalt-chromium stent of 81.0-μm strut thickness coated with a 7.8-μm durable fluoride-hexafluoropropylene polymer. The everolimus drug density is 1.0 μg/mm^2^, released by 120 days. PCI was performed according to local standard practices.
All patients were pretreated with aspirin and a P2Y12 inhibitor (clopidogrel, ticagrelor, or prasugrel); dual antiplatelet therapy was continued for at least 6 months and 12 months for patients with ACS.19^,^20
End points and outcome measures
The primary end point was the device-oriented outcome of TLF, a composite of cardiac death, target vessel MI, or clinically driven target lesion revascularization (TLR) at 12 months. The secondary end points included the components of the primary end point, death, MI (modified Third Universal Definition21), target vessel failure (composite of cardiac death, target vessel MI, or target vessel revascularization), major adverse cardiac events (composite of all-cause death, MI, or target vessel revascularization), bleeding complications defined by the Bleeding Academic Research Consortium,22 and stent thrombosis defined by the Academic Research Consortium.23 All events were adjudicated by an independent clinical event committee (Cardiovascular Research Foundation), and all baseline angiograms were reviewed by an independent angiographic core laboratory (Yale Cardiovascular Research Group).
Statistical analysis
Patient randomization was stratified by site and presentation (ACS vs CCS). The PIONEER III trial was designed to demonstrate the noninferiority of the primary TLF end point at 12 months in the intention-to-treat population. There was no prespecified hypothesis in this substudy. We compared patients and outcomes based on presentation (CCS vs ACS) and treatment allocation (Supreme DES vs DP-EES).
Categorical variables are reported as counts and percentages, and comparisons between treatment groups were performed using the χ^2^ or Fisher exact test. Continuous variables are presented as mean and standard deviation and compared with the 2-sample t test. If the data failed to meet the assumption for normality per the Shapiro-Wilk test, then the comparisons were made using the Wilcoxon rank sum test. Kaplan-Meier methods were used to calculate time-to-event outcomes, and the log-rank test was used for between-group comparisons. A Cox proportional hazards analysis was used to calculate hazard ratios (HR) with 95% CI and P values. Cox proportional hazard assumption was assessed by including a time-dependent covariate (an interaction between the treatment group and logarithm of event time) in the Cox proportional hazard model. A 2-sided P < .05 was considered to indicate a statistical significance. SAS version 9.4 (SAS Institute) was used for all statistical analyses.
Results
The PIONEER III trial enrolled 1628 patients, including 673 (41%) patients with ACS randomized to Supreme DES (n = 441) versus DP-EES (n=232) and 955 (59%) patients with CCS randomized to Supreme DES (n = 645) versus DP-EES (n = 310). Compared with CCS, patients with ACS were younger, fewer presented with less diabetes, hypertension, hyperlipidemia, previous PCI, and previous coronary artery bypass grafting, but more were often previous/current smokers (Table 1). A mean of 1.2 ± 0.5 lesions were treated in both ACS and CCS groups. PCI guidance with a fractional flow reserve (3.6% [30/809] vs 10.6% [123/1136]; P < .0001) and intravascular ultrasound (8.4% [69/809] vs 20.0% [231/1136]; P < .0001) was used less commonly in patients with ACS. In both ACS and CCS groups, treated lesions were mostly complex, with 64.3% (520/809) versus 67.8% (770/1136) meeting American College of Cardiology/American Heart Association B2/C criteria, respectively (P = .12). Patients with ACS presented with fewer lesions with a moderate-to-severe calcification (30.9% [249/807] vs 36.5% [415/1136]; P = .014) than patients with CCS, and use of plaque modification was infrequent (<1%) (Table 2). Within the ACS group, patients randomized to Supreme DES recorded a significantly higher percentage of complex lesions (ACC/AHH lesion class B2/C) (66.9% [356/532] vs 59.2% [164/277]; P = .04) and significantly a smaller final in-segment minimal lesion diameter (2.57 ± 0.40 mm vs 2.64 ± 0.41 mm; P = .03) (Table 2).Table 1. Baseline and procedural characteristicsCharacteristicsAcute coronary syndromesChronic coronary syndromesPaAll, N = 673Supreme DES n = 441DP-EES n = 232PAll, N = 955Supreme DES, n = 645DP-EES, n = 310PAge, y62.6 ± 10.562.9 ± 10.362.0 ± 10.8.3465.6 ± 9.465.7 ± 9.465.4 ± 9.6.83<.0001Female sex24.2% (163)21.3% (94)29.7% (69).1725.4% (243)25.4% (164)25.5% (79).98.57Smoker (current/previous)64.2% (432)62.4% (275)67.7% (157).4158.1% (555)60.5% (390)53.2% (165).03<.0001Diabetes mellitus25.4% (171)25.4% (112)25.4% (59).9933.8% (323)34.0% (219)33.5% (104).90.0003Insulin treatment33.9% (58)35.7% (40)30.5% (18).3733.4% (108/323)32.4% (71/219)35.6% (37/104).29.47Hypertension68.8% (463)71.2% (314)64.2% (149).0675.6% (722)76.3% (492)74.2% (230).48.002Hyperlipidemia71.9% (484)72.1% (318)71.6% (166).8880.2% (766)80.5% (519)79.7% (247).77<.0001Previous MI15.3% (103)16.3% (72)13.4% (31).3119.6% (187)18.1% (117)22.6% (70).11.03Previous PCI22.7% (153)23.8% (105)20.7% (48).3633.2% (317)30.9% (199)38.1% (118).03<.0001Previous CABG2.8% (19)3.4% (15)1.7% (4).216.0% (57)5.9% (38)6.1% (19).88.003Previous stroke2.8% (19)2.5% (11)3.4% (8).484.8% (46)5.4% (35)3.5% (11).20.043Renal insufficiency7.9% (53)7.9% (35)7.8% (18).748.0% (76)7.9% (51)8.1% (25).93.95No. of diseased vessels 168.9% (464)70.1% (309)66.8% (155).3973.2% (699)74.3% (479)71.0% (220).28.06 224.2% (163)21.8% (96)28.9% (67).0418.6% (178)18.1% (117)19.7% (61).57.006 ≥36.9% (46)8.1% (36)4.3% (10).028.2% (78)7.6% (49)9.3% (29).43.29Procedural characteristicsNo. of vessels treated per patient1.14 ± 0.351.14 ± 0.361.13 ± 0.34.911.11 ± 0.311.10 ± 0.291.14 ± 0.35.05.12Multiple vessels treated13.5% (91)13.6% (60)13.4% (31).9411.0% (105)9.6% (62)13.9% (43).05.17No. of target lesions per patient1.2 ± 0.51.2 ± 0.51.2 ± 0.4.431.2 ± 0.51.2 ± 0.41.3 ± 0.5.06.44 179.5% (532/672)80.5% (355)77.5% (179/231).3681.3% (776)82.8% (534)78.1% (242).08.37 218.6% (125/672)17.0% (75)21.6% (50/231).1415.8% (151)15.0% (97)17.4% (54).35.14 31.9% (13/672)2.5% (11)0.9% (2/231).242.9% (28)2.2% (14)4.5% (14).04.21No. of stents per patient1.3 ± 0.61.2 ± 0.61.3 ± 0.6.101.2 ± 0.61.2 ± 0.61.3 ± 0.6.09.82Radial access85.7% (577)86.4% (381)84.5% (196).5076.5% (731)77.4% (499)74.8% (232).39<.0001Brachial access0.3% (2)0.2% (1)0.4% (1)1.00.6% (6)0.6% (4)0.6% (2)1.0.48Femoral access14.0% (94)13.4% (59)15.1% (35).5422.8% (218)22.0% (142)24.5% (76).39<.0001Hemostasis device use76.7% (516)77.8% (343)74.6% (173).3571.3% (681)72.1% (465)69.7% (216).44.016Values are given as mean ± standard deviation or % (n).CCS, chronic coronary syndromes; DES, drug-eluting stent; DP-EES, durable polymer everolimus-eluting stent.aAll patients with acute coronary syndromes (ACS) vs all patients with CCS regardless of stent.Table 2. Angiographic characteristicsAcute coronary syndromesChronic coronary syndromesPaAll, N = 673 (809 lesions)Supreme DES, n = 441 (532 lesions)DP-EES, n = 232 (277 lesions)PAll, N = 955 (1136 lesions)Supreme DES, n = 645 (751 lesions)DP-EES n = 310 (385 lesions)PStent implantation characteristics No. of stents per lesion1.1 ± 0.31.1 ± 0.31.1 ± 0.3.921.1 ± 0.31.1 ± 0.31.0 ± 0.2.12.43 Stented lesion length, mm22.26 ± 9.4322.57 ± 9.6521.66 ± 8.99.1222.14 ± 8.5122.30 ± 8.6721.81 ± 8.19.22.62Maximum stent diameter, mm2.97 ± 0.432.95 ± 0.423.00 ± 0.44.242.91 ± 0.412.91 ± 0.412.91 ± 0.42.61.004Procedural characteristics Fractional flow reserve3.6% (30)3.7% (20)3.5% (10).8810.6% (123)10.2% (78)11.5% (45).49<.0001 Intravascular ultrasound8.4% (69)8.9% (48)7.3% (21).4420.0% (231)19.9% (152)20.2% (79).89<.0001 Predilation76.4% (630)79.6% (429)70.3% (201).0375.9% (887)77.5% (593)72.6% (284).07.80 Postdilation53.6% (440)53.2% (285)54.4% (155).7451.5% (591)51.7% (393/760)51.0% (198/388).83.35Target vessel locationb Left anterior descending43.3% (350)44.5% (237)40.8% (113).1846.0% (522)45.9% (345)46.0% (177).94.24 Left circumflex26.6% (215)27.1% (144)25.6% (71).9624.4% (227)25.3% (190)22.6% (87).38.28 Right coronary30.2% (244)28.4% (151)33.6% (93).1329.6% (236)28.6% (215)31.4% (121).34.77 Left main0.0% (0)0.0% (0)0.0% (0)NA0.1% (1)0.1% (1)0.0% (0)1.0.98ACC/AHA lesion class A9.4% (76)8.6% (46)10.8% (30).337.7% (88)7.1% (53)9.1% (35).23.20 B126.3% (213)24.4% (130)30.0% (83).1124.5% (278)25.8% (194)21.8% (84).14.37 B226.1% (211)27.3% (145)23.8% (66).3028.2% (320)26.2% (197)31.9% (123).05.32 C38.2% (309)39.7% (211)35.4% (98).2839.6% (450)40.9% (307)37.1% (143).24.53 B2/C64.3% (520)66.9% (356)59.2% (164).0467.8% (770)67.1% (504)69.1% (266).50.12Calcification (moderate/severe)30.9% (249/807)31.7% (168/530)29.2% (81).5636.5% (415)37.0% (278)35.6% (137).77.014Any bifurcation21.1% (171)21.4% (114)29.6% (57).7822.3% (253)22.4% (168)22.1% (85).94.55Baseline QCA resultsb Reference diameter, mm2.74 ± 0.452.72 ± 0.442.77 ± 0.47.102.68 ± 0.482.69 ± 0.482.67 ± 0.47.47.01 Minimal lumen diameter, mm0.87 ± 0.380.85 ± 0.370.90 ± 0.40.070.97 ± 0.390.98 ± 0.400.96 ± 0.39.40<.0001 Percent diameter stenosis, %68.02 ± 13.0468.35 ± 12.9767.37 ± 13.16.3163.63 ± 13.1963.49 ± 13.1963.92 ± 13.20.68<.0001 Lesion length, mmc15.22 ± 7.7315.53 ± 8.1614.64 ± 6.83.1615.06 ± 7.1315.11 ± 7.1014.95 ± 7.20.73.63Final QCA resultb In-stent minimal lumen diameter, mmc2.70 ± 0.402.68 ± 0.402.73 ± 0.40.092.65 ± 0.402.65 ± 0.412.65 ± 0.38.96.012 In-stent diameter stenosis, %c7.99 ± 4.728.14 ± 4.977.70 ± 4.22.208.38 ± 4.588.50 ± 4.348.14 ± 5.01.21.07 In-stent acute gain, mmc1.83 ± 0.461.83 ± 0.461.83 ± 0.47.921.68 ± 0.451.67 ± 0.451.69 ± 0.44.56<.0001 Segment minimal lumen diameter, mmd2.59 ± 0.412.57 ± 0.402.64 ± 0.41.032.55 ± 0.432.55 ± 0.432.54 ± 0.42.74.02 Segment diameter stenosis, %d9.65 ± 3.869.70 ± 3.899.55 ± 3.81.6610.06 ± 4.8010.09 ± 4.8610.00 ± 4.68.75.06 Segment acute gain, mmd1.72 ± 0.471.72 ± 0.481.73 ± 0.47.691.57 ± 0.461.57 ± 0.461.58 ± 0.46.82<.0001Values are given as mean ± standard deviation or % (n).ACC, American College of Cardiology; AHA, American Heart Association; QCA, quantitative coronary angiography.aAll patients with acute coronary syndromes (ACS) vs all patients with chronic coronary syndromes (CCS) regardless of stent.bThe results reported based on the angiographic core laboratory analysis.cThe total number of lesions was 802 for ACS and 1120 for CCS.dThe total number of lesions was 804 for ACS and 1127 for CCS.
At 12 months, there was not sufficient evidence to determine a difference in the primary end point of TLF (6.4% [42/673] vs 4.4% [42/955]; HR, 1.43; 95% CI, 0.93-2.19; P = .10) (Supplemental Table S1 and Figure 1A) or the components of the primary outcome including cardiac death, target vessel MI, and clinically driven TLR and target vessel failure, major adverse cardiac events, and definite or probable stent thrombosis were similar between the ACS and CCS groups (Figures 1B-D and 2). The rates of minor and major bleeding (4.2% [28/673] vs 2.1% [20/955]; HR, 2.02; 95% CI, 1.14-3.59; P = .014) and spontaneous MI (3.0% [19/673] vs 1.3% [12/955]; HR, 2.27; 95% CI, 1.10-4.68; P = .02) were higher in patients with ACS than those in patients with CCS (Supplemental Table S1).Figure 1Kaplan-Meier time-to-event curves for target lesion failure and its components in patients with ACS versus CCS. (A) Primary outcome (target lesion failure); (B) cardiac death; (C) target vessel MI; (D) clinically driven target lesion revascularization (TLR). ACS, acute coronary syndromes; CCS, chronic coronary syndromes; HR, hazard ratio; MI, myocardial infarction.Figure 2Kaplan-Meier time-to-event curves for secondary outcomes in patients with ACS versus CCS. (A) Target vessel failure; (B) major adverse cardiac events (MACE); (C) stent thrombosis (definite and probable). ACS, acute coronary syndromes; CCS, chronic coronary syndromes; HR, hazard ratio.
TLF at 12 months was similar for the Supreme DES and DP-EES subgroups among patients with ACS (6.6% [28/441] vs 6.0% [14/232]; P = .89) and those with CCS (4.5% [29/645] vs 4.3% [13/310]; P = .83) (Figure 3 and Central Illustration); the interaction P = .51 for TLF by clinical presentation. Stent thrombosis in patients with ACS occurred in 0.2% (1/441) and 0.4% (1/232) (P = .64) of patients with Supreme DES and DP-EES respectively. In patients with CCS, stent thrombosis occurred in 1.1% (7/645) and 0.3% (1/310) (P = .23) of patients with Supreme DES and DP-EES, respectively. In the ACS group, periprocedural MI was higher in the DP-EES group (1.6% [7/441] vs 4.7% [11/232]; P = .02), but spontaneous MI was higher in the Supreme DES group (4.0% [17/441] vs 1.0% [2/232]; P = .03) (Table 3).Figure 3Kaplan-Meier time-to-event curves for target lesion failure in patients with ACS and CCS based on stent type. (A) Target vessel failure in ACS; (B) target vessel failure in CCS. ACS, acute coronary syndromes; CCS, chronic coronary syndromes; DES, drug-eluting stents; DP-EES, durable polymer everolimus-eluting stents; HR, hazard ratio.Central IllustrationPrimary and secondary endpoints at 12 months in Supreme drug-eluting stent (DES) and durable polymer everolimus-eluting stent (DP-EES) in both acute coronary syndromes (ACS) and chronic coronary syndromes (CCS) presentation. ID-TLR, ischemia-driven target lesion revascularization; MACE, major adverse cardiac events; MI, myocardial infarction; ST, stent thrombosis; TLF, target lesion failure.Table 3. Outcomes at 1 year by presentation and treatmentAcute coronary syndromesChronic coronary syndromesP_interaction_Supreme DES, n = 441DP-EES, n = 232PSupreme DES, n = 645DP-EES, n = 310PPrimary outcome Target lesion failure6.6% (28)6.0% (14).894.5% (29)4.3% (13).83.96Secondary outcomes Major adverse coronary events8.9% (38)7.8% (18).726.4% (41)6.8% (21).81.67 Target vessel failure7.3% (31)7.8% (18).725.5% (35)5.2% (16).86.71 Any death0.7% (3)1.8% (4).210.5% (3)1.3% (4).16.93 Cardiac death0.5% (2)1.4% (3).430.2% (1)0.3% (1).59.86 Any myocardial infarction5.6% (24)5.2% (13).904.2% (27)3.9% (12).82.95 Periprocedural1.6% (7)4.7% (11).023.1% (20)2.9% (9).87.06 Spontaneous4.0% (17)1.0% (2).031.2% (8)1.3% (4).95.11 Any revascularization6.4% (28)3.6% (8).114.2% (27)4.3% (13)1.00.26 Target lesion revascularization2.9% (12)0.9% (2).102.2% (14)1.1% (3).19.72 Clinically driven2.9% (12)0.9% (2).101.9% (12)1.1% (3).30.61 Target vessel revascularization4.5% (19)3.1% (7).403.3% (21)2.9% (9).77.67 Clinically driven4.5% (20)3.1% (7).403.0% (19)2.9% (9).97.55 Nontarget vessel revascularization3.0% (13)1.8% (4).331.6% (10)2.1% (6).66.37 Any bleeding (BARC definition)3.5% (15)5.7% (13).172.5% (16)1.3% (4).23.08 BARC 3 or 53.3% (14)1.3% (3).141.6% (10)0.7% (2).24.97 Definite stent thrombosis0.0%0.4% (1).170.9% (6)0.3% (1).30.99 Early (0-30 d)0.0%0.4% (1).170.8% (5)0.3% (1).41.99 Late (31-365 d)0.0%0.0%—0.2% (1)0.0%.49>.99 Definite/probable stent thrombosis0.2% (1)0.4% (1).641.1% (7)0.3% (1).23.30 Early (0-30 d)0.2% (1)0.4% (1).640.9% (6)0.3% (1).30.34 Late (31-360 d)0.0%0.0%—0.2% (1)0.0%.49>.99Values are given as % (n).BARC, Bleeding Academic Research Consortium; DES, drug-eluting stent; DP-EES, durable polymer everolimus-eluting stent.
Discussion
This substudy of the PIONEER III trial stratified by clinical presentation shows the following important observations: (1) the primary device-specific outcome of TLF and its components were similar in the ACS and CCS groups at 12 months; (2) patients with ACS had more periprocedural bleeding and spontaneous MI; and (3) Supreme DES had similar rates of TLF with DP-EES irrespective of ACS or CCS presentation.
Outcomes based on ACS and CCS presentations
Unlike previous studies, this substudy did not demonstrate significant differences in outcomes between the ACS and CCS groups. Although patients with ACS showed increased platelet activation and delayed vessel healing compared with patients with CCS,5^,^24 the lower risk profile of the ACS cohort likely balances the overall observed outcomes of the ACS and CCS groups. In the PIONEER III trial, patients with ACS showed a significantly lower comorbid disease than those with CCS and were younger, with fewer presenting with diabetes, hypertension, hyperlipidemia, previous revascularization, and less lesions with moderate-to-severe calcification, all of which likely contribute to worse clinical outcomes for patients with CCS.25 Furthermore, although periprocedural MI may be more difficult to detect in ACS than that in CCS, we did observe a higher risk of spontaneous MI among patients with ACS which is in line with other studies.26^,^27 It is important to note that the study excluded patients with ST-elevation myocardial infarction (STEMI), who have been shown to experience a higher mortality within the first year of intervention than patients with other ACS.28
Device-related outcomes based on ACS and CCS presentations
Vascular response to stent implantation in patients with ACS has been shown to be associated with a less neointimal thickness, greater fibrin deposition, more inflammation, and greater areas of uncovered struts in autopsy series,5 and OCT studies have confirmed a greater stent malapposition and more uncovered struts in patients with ACS.7 Furthermore, perfusion imaging studies have shown that patients with ACS show significantly impaired vasodilator response compared with patients with CCS after PCI, and this impairment persists as long as 6 months.29 Immunohistologic studies investigating circulating endothelial cells, which are associated with endothelial injury, show significantly higher circulating endothelial cells counts in ACS than those in CCS.30 Because the endothelium plays a central role in releasing vasoactive substances and is the main modulator of vascular tone,31 these studies suggest that, in ACS, endothelial injury is accentuated, and its function is impaired long after the acute insult.
The Supreme DES design emphasizes early synchronized elution of antiproliferative drug and polymer degradation to promote early endothelial restoration.14 The concept that the Supreme DES achieves early healing and restoration of endothelial function is supported by intracoronary OCT data from a randomized study, showing more complete strut coverage at 1 month than that with DP-DES (83.8 ± 10.4% vs 73.0 ± 17.5%; P = .04).32 Furthermore, in vivo data using Evans Blue staining and P120/VE-cadherin co-staining to assess the integrity of the endothelial barrier showed an improved restoration of endothelial function with Supreme DES compared with that with other second-generation DESs.33 The results from the PIONEER III trial show that device-specific outcomes with Supreme DES, such as TLF and ST, were similar to DP-EES for both ACS and CCS groups at 12 months. Given that the PIONEER III trial was designed to demonstrate the noninferiority of TLF between devices at 1 year and differentiation in outcomes with Supreme would be expected after 1 year, the current results with Supreme DES are reassuring, especially in the ACS cohort. Among patients with ACS, clinically driven TLR was numerically higher and spontaneous MI was significantly higher in the Supreme DES group than those in the DP-EES group at 12 months, which may be due to an imbalance of patients with more complex lesion (American College of Cardiology/American Heart Association class B2/C) and smaller final segment minimal lesion diameter at the end of the procedure in patients with ACS randomized to the Supreme DES group, both factors known to be associated with worse clinical outcomes such as MI and TLR.34^,^35 The higher observed rate of spontaneous MI in the Supreme group was likely related to nontarget lesion plaque rupture rather than stent thrombosis related to the Supreme DES because adjudicated rates of stent thrombosis were exceedingly rare in both groups. In the ACS population, periprocedural MI occurred more frequently in the DP-EES population, with the prognostic importance of periprocedural MI being substantially less than that of spontaneous MI.26
Several studies have evaluated biodegradable polymer drug-eluting stents (BP-DESs) in patients with ACS and yielded mostly modest or no benefit, and outcomes vary based on specific stent designs.36 The only BP-DES that has shown consistent benefit in ACS populations is the ultrathin bioresorbable Orsiro stent. The BIOFLOW V trial included 677 patients with ACS, in whom the Orsiro BP-DES placement resulted in a reduction in TLF at 12 months compared with the Xience DP-EES placement (5.6% vs 11.0%; difference, −5.37%; 95% CI, −10.66% to −0.96%; P = .02).37 In a subgroup analysis of the BIOSCIENCE trial including patients with STEMI, the Orsiro stent reduced TLF at 12 months compared with Xience (3.4% vs 8.8%; rate ratio [RR], 0.38; 95% CI, 0.16-0.91; P = .02),38 although the results were no longer significant at 5 years (16.9% vs 16.0%; RR, 1.04; 95% CI, 0.78-1.41; P = .78).39 In the BIOSTEMI trial of patients with STEMI exclusively, the Orsiro stent resulted in a significant reduction in TLF compared with Xience (4.0% vs 6.0%; RR, 0.59; 95% Bayesian CrI, 0.37-0.94).40 Orsiro is not only the alone DES showing superiority in patients with STEMI but also the alone DES to show an inferior performance in treating complex calcified lesions.41 Studies of other BP-DES in patients with ACS have not demonstrated clinical benefit compared with DP-DES,42^,^43 highlighting that not all BP-DES are created equal, and each DES needs to be evaluated individually because there is no evidence for a class effect of BP-DESs.
Limitations
The PIONEER III trial was designed to demonstrate the noninferiority of the primary composite TLF end point. Although randomization was stratified by ACS presentation, this subgroup analysis was not powered to demonstrate the noninferiority or differences in event rates between ACS and CCS populations or treatment groups. Therefore, the results are purely hypothesis generating. PIONEER III excluded patients with STEMI, and multivessel and multilesion treatment were uncommon, and the results only apply to the population studied.
Conclusions
In the PIONEER III trial, there was no sufficient evidence to suggest a difference in TLF at 12 months between Supreme DES and DP-EES in both ACS and CCS groups. Ongoing follow-up to 5 years will determine whether a clinical benefit exists in the longer term.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Levine G.N.Bates E.R.Blankenship J.C.2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions J Am Coll Cardiol 58232011 e 574e 65110.1016/j.jacc.2011.08.00722070834 · doi ↗ · pubmed ↗
- 2Authors/Task Force members Windecker S.Kolh P.2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI)Eur Heart J 35372014254126192517333910.1093/eurheartj/ehu 278 · doi ↗ · pubmed ↗
- 3Amsterdam E.A.Wenger N.K.Brindis R.G.2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Circulation 130102014 e 344e 4262524958510.1161/CIR.0000000000000134 · doi ↗ · pubmed ↗
- 4Pilgrim T.Vranckx P.Valgimigli M.Risk and timing of recurrent ischemic events among patients with stable ischemic heart disease, non-ST-segment elevation acute coronary syndrome, and ST-segment elevation myocardial infarction Am Heart J 175201656652717972410.1016/j.ahj.2016.01.021 · doi ↗ · pubmed ↗
- 5Nakazawa G.Finn A.V.Joner M.Delayed arterial healing and increased late stent thrombosis at culprit sites after drug-eluting stent placement for acute myocardial infarction patients: an autopsy study Circulation 118112008113811451872548510.1161/CIRCULATIONAHA.107.762047 · doi ↗ · pubmed ↗
- 6Kubo T.Imanishi T.Kitabata H.Comparison of vascular response after sirolimus-eluting stent implantation between patients with unstable and stable angina pectoris: a serial optical coherence tomography study J Am Coll Cardiol Img 14200847548410.1016/j.jcmg.2008.03.01219356470 · doi ↗ · pubmed ↗
- 7Räber L.Zanchin T.Baumgartner S.Differential healing response attributed to culprit lesions of patients with acute coronary syndromes and stable coronary artery after implantation of drug-eluting stents: an optical coherence tomography study Int J Cardiol 173220142592672463111310.1016/j.ijcard.2014.02.036 · doi ↗ · pubmed ↗
- 8Joner M.Finn A.V.Farb A.Pathology of drug-eluting stents in humans: delayed healing and late thrombotic risk J Am Coll Cardiol 48120061932021681466710.1016/j.jacc.2006.03.042 · doi ↗ · pubmed ↗