Herpes Simplex Esophageal Ulcer in an Immunocompetent Adult With Hematemesis
Yusuke Nomoto, Makoto Furihata, Taro Osada

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
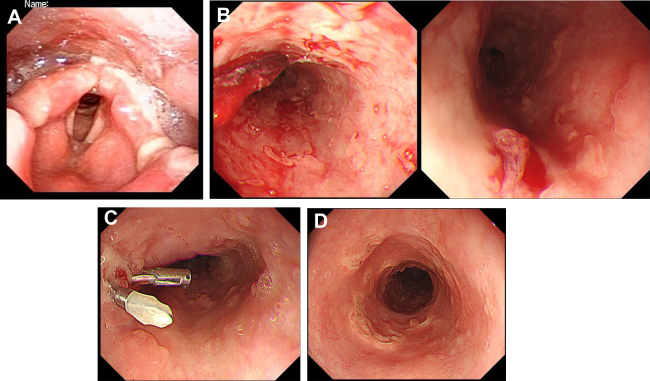 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Parvovirus B19 Infection Studies · Polyomavirus and related diseases
A 61-year-old man with pharyngitis and stomatitis for 2 months was admitted due to difficulty in swallowing solids. Laryngoscopy demonstrated multiple laryngopharyngeal ulcers with exudative laryngopharyngitis (Figure A). He had elevated IgM antibody for herpes simplex virus (HSV). Acyclovir (750 mg daily) was orally administered soon after admission. After 2 days, he had hematemesis and tarry stool. Hemoglobin level decreased to 4.9 g/dL with hemorrhagic shock and required blood transfusion. Urgent upper gastrointestinal endoscopy showed multiple erosions and ulcers with spurting bleeding in the upper esophagus (Figure B). Multiple skipping erosions and round-shaped ulcers were spread 10 cm-wide. Temporal hematemesis is achieved by endoscopic clips to a visible vessel (Figure C). Punched-out ulcers remained but bleeding arrest was reconfirmed by follow-up endoscopy 3 days later. Sixty days post-discharge, endoscopy showed multiple scaring replaced the lesions (Figure D). His symptoms disappeared completely over time, with no recurrence so far. Our report gives a clinical description of exceedingly rare HSV esophageal ulcers accompanying hematemesis in an immunocompetent individual. Though the patient took warfarin and aspirin for old myocardial and middle cerebral infarction, he was not deemed immunocompromised. We propose esophagitis due to HSV should be considered a causative factor for hematemesis even in an immunocompetent host.