Stent Placement Using a Combination of Decompression Tube and Colonoscopy for Malignant Ileocolonic Obstruction
Mie Tanabe, Naoki Ishii, Daisuke Inagaki

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1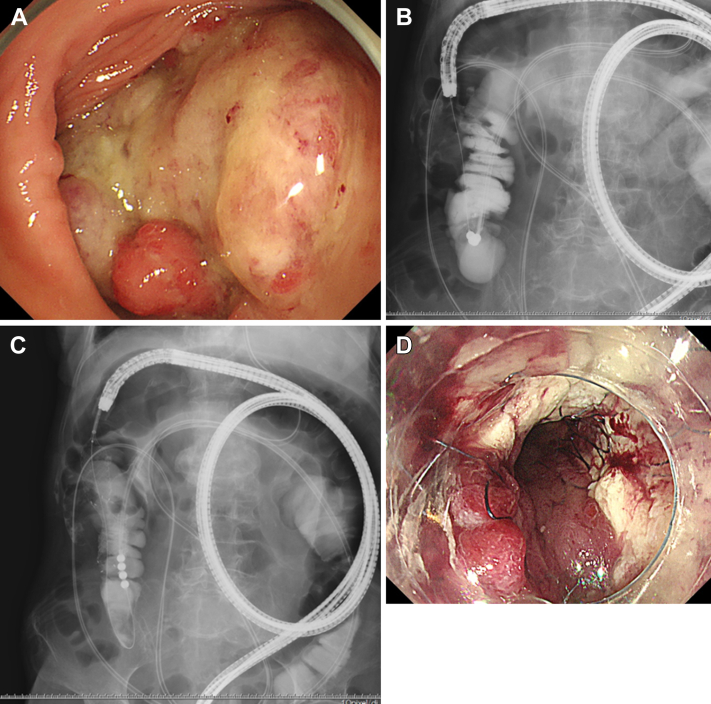 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Surgical Treatments · Diverticular Disease and Complications · Intestinal Malrotation and Obstruction Disorders
The placement of self-expandable metallic stents (SEMSs) from colon to terminal ileum for malignant ileocolonic obstruction (MIO) is technically challenging, often necessitating surgery. However, it is recommended for patients with severe comorbidities, who cannot tolerate general anesthesia and surgery. We performed the first case of SEMS placement for MIO using the combination of a decompression tube and colonoscopy.
A 101-year-old female underwent computed tomography for the assessment of abdominal pain and vomiting. MIO was suspected (Figure A1). A decompression tube was first inserted. A colonoscopy without bowel purge demonstrated a protruding-type colonic cancer occupying the ascending colon (Figure A). Due to advanced age and comorbidities, SEMS placement was planned to alleviate the symptoms. Due to ileocolonic anatomy and difficulties in identifying the opening mouth for colonoscopic guidewire insertion, the guidewire was, instead, passed into the ascending colon through a decompression tube, grasped by colonoscopy forceps and brought out from the working channel of the colonoscope (Figure B). The SEMS was deployed using the guidewire from the ascending colon into the terminal ileum (Figure C and D). The decompression tube was pulled away. After the -procedure, the patient had no episodes of abdominal pain or vomiting and was able to eat after stenting.