Emergent Percutaneous Transluminal Coronary Angioplasty of an Occluded Giant Ectatic Coronary Aneurysm
Jay M. Patel, Carlos Sisniega, Aleesha Shaik, Olcay Aksoy, Daniel Levi, Rushi V. Parikh

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
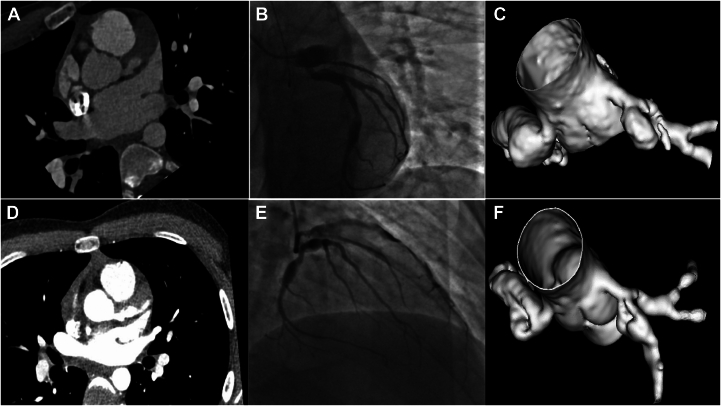 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKawasaki Disease and Coronary Complications · Coronary Artery Anomalies · Coronary Interventions and Diagnostics
The incidence of giant coronary aneurysms (GCAs) and subsequent intracoronary thrombosis is approximately 0.02%, with most occurring due to Kawasaki disease or Takayasu arteritis.1 Currently, there are only a few reported cases of GCA secondary to multisystem inflammatory syndrome in children.2
This case report involves a 14-year-old boy with multisystem inflammatory syndrome in children secondary to COVID-19 infection in 2020, which was complicated by the development of GCAs of the entire coronary tree. In addition to immediate treatment with intravenous immunoglobulin and steroids, he was prescribed rivaroxaban and aspirin for his GCAs. He was in his usual state of health until he recently presented to a nearby emergency department with several hours of substernal chest pain that awoke him from sleep and radiated to his neck, jaw, and left arm. Examination was notable for stable hemodynamics. Serial electrocardiograms showed dynamic and progressive anterolateral ST elevations, and the initial troponin I concentration was 0.5 ng/mL. An urgent coronary computed tomography angiogram (CCTA) revealed serial GCAs of the right coronary artery and left circumflex artery and an occluded GCA of the proximal left anterior descending (LAD) coronary artery (Figure 1A, C). GCAs measured ≤12.4 mm in the right coronary artery, 13.5 mm in the left circumflex artery, and 9.6 mm in the LAD.Figure 1LAD before intervention. CCTA images (A) and 3D reconstruction (C) showed proximal occlusion of aneurysmal LAD, which was corroborated on angiography (B). Postangioplasty angiography demonstrated restoration of flow to the distal LAD (E). CCTA images (D) and 3D reconstruction (F) 48 hours later showed continued vessel patency. CCTA, coronary computed tomography angiogram; LAD, left anterior descending coronary artery
Given the acute myocardial infarction in the setting of a thrombosed proximal LAD GCA, the patient was emergently transferred to our institution where coronary angiography confirmed the findings on CCTA (Figure 1B; Supplemental Videos 1 and 2). We successfully crossed the organized thrombus using a Fielder XT coronary guide wire within a microcatheter. We deferred aspiration thrombectomy given the massive size of the thrombus and consequently low likelihood of efficacy. Rather, we performed serial percutaneous transluminal coronary angioplasty (using ≤3.0-mm semicompliant balloon), which resulted in restoration of TIMI grade II flow to the distal vessel (Figure 1E and Supplemental Video 3) and resolution of the patient’s symptoms. We elected against stent placement for GCAs because it would have resulted in severe malapposition. Finally, owing to extensive residual thrombus burden, we chose to prescribe the patient a robust antiplatelet/anticoagulant regimen of aspirin, ticagrelor, intravenous heparin (48 hours), and eptifibitide (24 hours).
The patient remained chest pain free, and the troponin I level peaked at 100 ng/mL. Repeat CCTA 48 hours later showed a patent LAD with a good distal flow (Figures 1D, F; Supplemental Video 4). A transthoracic echocardiogram demonstrated hypokinesis in the LAD territory and a left ventricular ejection fraction of 40% (previously at a normal range). He was discharged on short-term triple therapy (aspirin, ticagrelor, and warfarin) with planned discontinuation of aspirin at 1 month. At the 3-month follow-up, the patient reported no further chest pain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pham V.Hemptinne de Q.Grinda J.M.Duboc D.Varenne O.Picard F.Giant coronary aneurysms, from diagnosis to treatment: a literature review Arch Cardiovasc Dis 1131202059693186617310.1016/j.acvd.2019.10.008 · doi ↗ · pubmed ↗
- 2Villacis-Nunez D.S.Hashemi S.Nelson M.C.Giant coronary aneurysms in multisystem inflammatory syndrome in children associated with SARS-Co V-2 infection J Am Coll Cardiol Case Rep 31320211499150810.1016/j.jaccas.2021.06.043PMC 849405634642670 · doi ↗ · pubmed ↗